
From the 1Faculty of Medicine, University of Iceland, 2The Icelandic Gerontological Research Centre, 3Department of Physiotherapy, Landspitali, University Hospital of Iceland, Reykjavik, 4Akureyri Hospital, Akureyri, Iceland, and 5Department of Physical Therapy, University of Pittsburgh, Pittsburgh, PA, USA
Objectives: To investigate vestibular function, foot sensation, postural control and functional abilities, and to evaluate whether these variables are associated with fall-related wrist fracture.
Methods: A case-control study was conducted with 98 subjects, age range 50–75 years, who had sustained a fall-related wrist fracture. Forty-eight sex-,
age- and physical activity-matched individuals, with no previous history of wrist fracture, served as controls. Measurements included: head-shake test (HST), tuning fork, biothesiometer, Semmes-Weinstein monofilaments (MF), Sensory Organization Test (SOT), Five-Times-Sit-to-Stand Test (FTSTS), 10-m walk test (10MWT), Activities-specific Balance Confidence (ABC), and the Dizziness Handicap Inventory (DHI) scales. Logistic regression models were used to determine associations of variables with a fall-related wrist fracture.
Results: Vestibular asymmetry was apparent in 82% of wrist fracture subjects and 63% of controls (p = 0.012). Plantar pressure sensation (p <0.001), SOT composite scores (p < 0.001), 10MWT (p <0.001), FTSTS (p <0.001), ABC (p <0.001) and DHI (p <0.005) were significantly poorer among cases than controls. A positive HST (odds ratio (OR) 5.424; p = 0.008) and monofilament sensation (OR 3.886; p = 0.014) showed the strongest associations with having a fall-related wrist fracture.
Conclusion: Asymmetrical vestibular function and reduced plantar pressure sensation are associated with fall-related wrist fractures among the ageing population. These factors are potential targets for future interventions.
Key words: wrist fracture; vestibular-asymmetry; plantar sensation; postural control; functional ability.
Accepted Nov 17, 2017; Epub ahead of print Dec 22, 2017
J Rehabil Med 2018; 50: 00–00
Correspondence address: Bergthora Baldursdottir, Department of Physiotherapy, Landspitali, University Hospital of Iceland, Tungata 5, IS-101 Reykjavik, Iceland. E-mail: bergbald@landspitali.is
Falls and fractures in older adults are a major health issue and socioeconomic challenge for Western societies. Each year approximately one-third of people over 65 years of age sustain a fall (1), which can result in a fracture. Wrist fracture (distal forearm fracture) is the most common first fracture among Icelandic women, with a sharp increase in incidence between 45 and 60 years of age, and is the third most common first fracture among men (2). Wrist fracture is a strong predictor of future fracture risk (3) and is often a precursor to the more serious hip fracture (4), which can result in decreased quality of life, death, and increased health cost (5).
Our upright posture is unstable from a biomechanical point of view. In order to control it, coordinated muscular activity, dependent on sufficient and coherent mechanoreceptive, proprioceptive, vestibular and visual information, is needed (6). Multisensory input is syn-chronized at several levels within the central nervous system (CNS). Appropriate motor patterns are then selected for postural adjustments and movements (7). Age-related degenerative changes affect all domains involved in postural control and become apparent between the ages of 40 and 50 years (8). Decreased vibration sensation in the lower limbs has been associated with increased postural sway among healthy older adults (9). An association of vestibular asymmetry with falls and wrist fractures (10, 11), as well as hip fractures (12), has been reported. Body-orienting reflexes, muscle strength and tone, and step length and height all decline with age, and impair the ability to avoid a fall after an unexpected trip or slip (13).
Fear of falling has been recognized as an important psychological factor associated with falls (14). Fear of falling can lead to decreased confidence in daily activities and a vicious circle of increased disability and risk of further falls. In addition, fear of falling has been shown to be an independent predictor of decline in physical function (15). The prevalence of dizziness among older adults is substantial (16) and has been identified as a risk factor for falls (17).
Limited research has been performed into mechanoreceptive sensation in the lower limbs among people who have sustained a wrist fracture, and the prevalence of asymmetrical vestibular function among this group has not been compared with matched controls. In addition, the associations between postural control, vestibular function, mechanoreceptive sensation in the lower limbs, functional ability, perceived dizziness, fear of falling, and wrist fractures are not clear.
The aim of this case-control study was to investigate vestibular function, mechanoreceptive sensation in the lower limbs, postural control, functional abilities, perceived dizziness and confidence in individuals in the age range 50–75 years with and without fall-related wrist fractures. The associations between sensory and physical dysfunction and age were examined. In addition, multivariate models were used to determine whether vestibular, mechanoreceptive and physical functions are independently associated with being in the wrist fracture group.
A total of 146 persons agreed to participate in this case-controlled study. Of these, 98 (85 women, 13 men) had sustained a fall-related wrist fracture (mean age (standard deviation; SD): 61.9 (7.1) years; range 50–75). They were identified from medical records at the emergency department of Landspitali, University Hospital in Iceland and recruited for the study 2–5 months after the fracture. They were screened for eligibility from a total of 440 consecutive patients during a 12-month period. Exclusion criteria were a confirmed diagnosis of degenerative CNS disease, such as Parkinson’s disease, Alzheimer’s disease, and other diseases that impair mobility and cognitive function. Half of the patients (n = 219) did not fulfil the inclusion criteria, thus 221 patients were invited to take part in the study. The participation rate of eligible patients was 44%. The enrolled subjects were healthy, although some were taking medication for hypertension (n = 29), high cholesterol (n = 14), diabetes type 2 (n = 2) and vitamin B12 deficiency (n = 1). Fourteen subjects had a previous history of benign positional postural vertigo (BPPV). A comparison group was comprised of a convenience sample of 48 healthy individuals (38 women, 10 men) without previous history of fall-related wrist fractures, matched according to age, sex and weekly physical activity level during the previous 12 months. The control group was identified through a network of colleagues, friends and family members. Reported duration of physical activity was divided into 3 groups: < 1 h/week, 1–3 h/week, and > 3 h/week. The size of the control group was determined as 1:2 in relation to the size of the fracture group due to homogeneity among control subjects. The study was approved by the Icelandic National Bioethics Committee (VSNb2013110036/03.11) and performed in accordance with the ethical standards laid down in the 1964 Declaration of Helsinki and its later amendments. All persons gave their informed written consent prior to inclusion in the study.
Participants answered questions regarding their general health, including medication, previous falls and fractures, and level of weekly physical activity (h/week) during the previous 12 months. They were also questioned about the circumstances of the fall that had caused the distal forearm fracture.
Activities-specific Balance Confidence Scale (ABC). Participants rated their level of confidence while performing 16 activities of daily living, on a percentile scale from zero (no confidence) to 100 (complete confidence) (18). Individual items ranged in difficulty, from walking on level surfaces inside the home to walking outdoors on icy pavements.
Dizziness Handicap Inventory Scale (DHI). The DHI was utilized to assess the individual’s handicap because of his/her dizziness and/or unsteadiness. The scale comprises 25 items relating to physical, emotional and functional domains. The range of possible scores on the DHI is 0–100; the higher the score, the greater the level of self-perceived handicap (19). If participants perceived themselves as dizzy they were assessed with the Dix-Hallpike manoeuvre to exclude BPPV (20).
Each of the measurements shown below was conducted once per participant.
Vibration perception. A tuning fork (128 Hz) was used to assess vibration perception in the lower limbs. The sensation was graded from 1 to 3 according to the following criteria: Sensation 1: vibration detected at the base of first metatarsal bone, medial malleolus and tibial tuberosity. Sensation 2: vibration detected at the medial malleolus and tibial tuberosity. Sensation 3: vibration detected only at the tibial tuberosity. This method was used in accordance with other studies, on estimation of vibration sensation in the lower limbs among elderly subjects (9, 12, 21).
Biothesiometer electronic device. A biothesiometer (Model EG electronic BioThesiometer, Newbury, OH, USA) that generated a 120 Hz vibration of varying amplitude (in µm) was used to measure vibration perception on the plantar surface of the foot. Vibration was applied to the plantar surface of the first metatarsal bone (the base of the big toe), the fifth metatarsal bone (the base of the little toe) and the centre of the plantar surface of the heel. Subjects were asked to indicate to the examiner whether they were able to feel the vibration (yes/no) (22). Vibration was applied once in ascending intensity until the subject could feel the vibration and then in descending intensity until the subject could no longer feel the vibration. Vibration was applied again in ascending intensity until the subject could feel the vibration, which was registered as the perception threshold, in line with operational instructions from the manufacturer of the biothesiometer.
Tactile sensitivity. Semmes-Weinstein pressure aesthesiometer (Semmes-Weinstein Mono-filaments, San Jose, CA, USA) was used to measure tactile sensitivity. The aesthesiometer is composed of 20 nylon filaments of equal length, with varying diameters. The filaments were applied to the plantar surface of the same 3 points as the biothesiometer, and participants were instructed to report whether they felt it on the “heel”, “at the big toe”, or “at the little toe”. The tactile sensation threshold was determined by presenting suprathreshold filaments initially, then applying thinner and thinner filaments until the subject could no longer detect them (23). The examiner then applied thicker filaments until the subject could detect them, which was determined as the touch threshold and presented as pressure (in g).
A head-shake test (HST) was used to assess vestibular function. Goggles, equipped with an infrared-charged device camera (no visual cues), were used to record eye movements. Participants were exposed to a passive head shaking test (~2 Hz/20 s) in the supine position with the head in 30° of neck flexion with the eyes closed. After an abrupt halt of the head shaking, the eyes were immediately opened and eye movements were recorded (24). A specialist in neuro-otology experienced in nystagmoscopy, blinded to whether the recordings were from wrist fracture subjects or controls, evaluated the eye movements from the recordings. The test is considered positive for vestibular asymmetry when eye deviation occurs with 3 or more interposed fast phases, i.e. nystagmus (25). An eye deviation of more than one interposed fast phase is considered a sign of weak asymmetry, especially if it prevails on repeated testing (10). In this study we used 2 or more fast eye beats as being a positive test as has been used in previous studies (10, 12). The HST was preferred to caloric irrigation as it is a functional test depending on both labyrinths simultaneously in the high frequency range. Furthermore, the HST was chosen to be able to compare results with previously published studies (10, 11).
Sensory Organization Test in the Smart Balance Master (SOT); (Neurocom Inc., Clackamas, OR, USA) was utilized to measure postural control. The test evaluates the subject’s ability to make effective use of somatosensory, visual and vestibular inputs and suppress inappropriate sensory information. Composite scores of postural sway from the 6 different sensory conditions were used for analysis. Further description of the SOT and the measuring procedure has been published previously (26).
Five-Times-Sit-To-Stand Test (FTSTS). Functional lower limb muscle strength was measured with the FTSTS. The participants were instructed to rise from a chair with a seat height of 43 cm, as fast as possible, 5 times, with their hands crossed on their chest. The time (in s) was recorded (27).
10-m walk test (10MWT). Gait speed was measured with the 10MWT to assess locomotion as a part of balance control. A 20-m straight path was used, with 5 m for acceleration, 10 m for steady-state walking, and 5 m for deceleration. Markers were placed at the 5- and 15-m positions along the path. Participants began to walk at one end of the 20-m path and continued walking until they reached the other end. Timing started at the first marker and stopped when the participants crossed the second marker. The test was performed at their preferred walking speed and repeated at the subject’s fastest speed. Gait speed was calculated (in m/s) as the distance covered divided by the time it took the individual to walk the distance (28).
Statistical analysis was conducted using SPSS for Windows version 24.0 (SPSS, Chicago, IL, USA) and the level of significance was set at p < 0.05. Data were checked for normality using the Kolmogorov–Smirnov test and are shown as median and ranges for not normally distributed variables and as mean (SD) for normally distributed variables. Comparisons between groups were made using the Mann–Whitney U test (not normally distributed variables) or independent samples t-test (normally distributed variables). Correlations between variables were calculated using Spearman’s rho.
The Kruskal–Wallis test (not normally distributed variables) and one-way ANOVA, including Fisher’s least significant difference (LSD) post hoc test (normally distributed variables), were used to find characteristics of variables by age group, each covering approximately one-third of the age range in the present study (group 1: 50–58 years, group 2: 59–66 years, group 3: 67–75 years). Logistic regression models were used to find associations of variables with having obtained a fall-related wrist fracture (see Table IV). Model 1 included mechanoreceptive sensation and vestibular function; model 2 additionally included postural control; model 3 additionally included perceived dizziness handicap and confidence; and model 4 additionally included walking speed and strength in the lower limbs.
Characteristics of participants and differences between the wrist fracture and the control groups are shown in Table I. There were significant differences between the groups for most of the variables, indicating poorer plantar pressure sensation and poorer vestibular and physical function in the wrist fracture group. Vestibular asymmetry was apparent in 82% of the wrist fracture subjects, but in only 64% of the controls (p = 0.012). Vibration sensation did not differ between the groups. The fracture group used, in mean, 1.7 medications (range 0–9) and the control group 1.1 (range 0–6).
Table I. Characteristics of participants categorized by group
Tripping was the most frequently reported reason for the fall, accounting for 41% of subjects, followed by 36% slipping on an icy surface, 14% slipping on a wet surface, 6% during sport activities, and 3% associated with sudden head movements.
Table II shows correlations of sensation (monofilaments, tuning fork, biothesiometer and HST) and physical function (10MWT and FTSTS) with postural control, perceived dizziness handicap and confidence. Walking speed and lower extremity strength (FTSTS) had a weak to moderate correlation with the SOT (R = 0.342/–0.506), ABC (R = 0.395/–0.497) and DHI (R = –0.265/0.310) and monofilaments had a weak correlation with ABC (R = –0.295).
Table II. Spearman’s rho correlations for monofilaments, tuning fork, biothesiometer, head-shake test (HST), 10-m walk test (10MWT) and 5-Times-Sit-To-Stand (FTSTS) compared using the Sensory Organization Test (SOT), Activities-specific Balance Confidence Scale (ABC) and Dizziness Handicap Inventory (DHI). (All subjects included, n=146)
Characteristics of the participants categorized by age group are shown in Table III. Vibration sensation, i.e. biothesiometer (p ≤ 0.001) and tuning fork (p = 0.02), walking speed; comfortable walking speed (p = 0.001), fast speed (p ≤ 0.001) and lower limb functional muscle strength (p = 0.038) were the only variables that were significantly different between age groups.
Table III. Characteristics of the participants categorized by age group. (All subjects included, n = 146)
Multivariate linear models in Table IV show that mechanoreceptive sensation; biothesiometer (OR 0.843; 95% confidence interval (95% CI) 0.737–0.965) and monofilament (OR 5.643; 95% CI 2.363–13.473), a positive HST (OR 3.874; 95% CI 1.544–9.724), SOT (OR 0.899; 95% CI 0.835–0.968) and FTSTS (OR 2.040; 95% CI 1.389–2.997]) were associated with being in the wrist fracture group, but not walking speed, perceived dizziness handicap and confidence.
Table IV. Logistic regression models for a fall-related wrist fracture
The association between SOT and a fall-related wrist fracture was partly explained by perceived dizziness handicap and confidence, although the SOT composite score remained significant (OR 0.921; 95% CI 0.850–0.998). The association between the SOT and a fall-related wrist fracture disappeared when corrected for walking speed and functional strength in the lower limbs. In the final model a positive HST (OR 5.424; 95% CI 1.570–18.740) and monofilaments sensation (OR 3.886; 95% CI 1.318–11.457) showed the strongest associations with having obtained a fall-related wrist fracture.
The results of this case-control study show that individuals aged 50–75 years with fall-related wrist fractures have a higher incidence of asymmetrical vestibular function, decreased plantar pressure sensation and poorer postural control compared with matched controls. They also have slower walking speed and reduced strength in their lower limbs. In addition, wrist fracture subjects perceived more dizziness handicap and less confidence during daily activities and they had sustained a higher number of previous falls and fractures than controls. According to multivariate analysis, a positive HST and decreased plantar pressure sensation had the strongest associations with being in the wrist fracture group.
Subjects were recruited 2–5 months after the fracture, and during that time some of the subjects had been referred to physical therapy, consisting of exercises to improve movement and strength in the wrist and decrease pain. These exercises were conducted in a sitting position and therefore it is unlikely that they had an impact on the variables being analysed in the study.
The individuals in the wrist fracture group and comparison group were matched according to age, sex and amount of physical activity level (h/week). Physical activity is known to stimulate the function of both the sensory and motor systems and, by matching this with sex and age, comparison of the fracture group and the control group became more meaningful. The definition of physical activity was fairly broad and encompassed strenuous activities of daily living and recreation. With regard to possible impact of retirement on level of physical activity, information about this was not collected. However employment is high in the age range 50–66 years in Iceland and the most common retirement period is in the age range 67–70 years. After the age of 70 years retirement is nearly 100%. In light of this, the level of employment was considered comparable between the 2 groups.
The vestibular organs play a major role in coordinating head and eye movements and modifying muscle tone for postural adjustments (29). They also contribute to the estimation of the internal representation of body vertical and the subject’s mental representation of position in space (30). Nystagmus after head shaking is generally considered pathological (31) and demonstrates asymmetry of the vestibular system (32). A previous study by Kristinsdottir et al. (10) found a high prevalence of asymmetrical vestibular function (76%) among patients with fall-related wrist fractures, similar to that found in our study. Ekvall Hansson et al. (11) found a somewhat lower incidence of vestibular asymmetry (65%) in a similar patient group; however, they used ≥ 3 fast eye beats as a threshold value for a positive HST which may explain observed differences between studies.
Vestibular asymmetry appears to be frequent in older adults as the control group also displayed a high prevalence of a positive HST in our study. However, as the prevalence of vestibular asymmetry was significantly higher in persons after wrist fracture than in controls, our findings indicate a possible association between vestibular asymmetry and fall-related wrist fractures. In our group of participants, the occurrence of nystagmus was seen, yet the subjects were asymptomatic, physically active, and not complaining of dizziness or unsteadiness, as demonstrated by the low DHI score. There also was no relationship between perceived dizziness handicap, confidence and postural control scores on the SOT among the participants.
Previous studies have reported a correlation between decreased vibration sensation (9, 33, 34) and tactile sensitivity (35) with increased postural sway among the older adults. In our study we did not find correlations between mechanoreceptive sensation, i.e. tuning fork, biothesiometer, monofilaments and SOT. Monofilament sensation was correlated with ABC scores, possibly indicating the importance of detecting weight distribution on the soles of the feet to feel confident during daily activities. As measurements of vibration perception (tuning fork and biothesiometer) were mostly in the normal range in our participants, this could explain the lack of significant associations between these variables and the SOT composite scores. According to data provided by the manufacturer, almost all our participants had diminished light touch and some participants in the fracture group had diminished protective sensation. Rinkel et al. recently reported normative data for cutaneous threshold in the feet among 196 healthy adults (36). Our findings indicate that tactile sensitivity (monofilament) in the control group were within the normal range, whereas, some participants in the fracture group had diminished sensitivity, as defined by Rinkel et al.
According to previous studies, sensation, strength and physical function decrease with age (36–39). However, it is not clear whether clinically relevant changes occur between the ages of 50 and 75 years. Our study shows that age was related to a lower vibration sensation, slower walking speed, and poorer functional muscle strength in the lower limbs in our participants. This is in accordance with the results of other studies (9, 27, 38). However, there were no differences between age groups in SOT, DHI and ABC, possibly indicating that relevant changes in these variables occur later in life. There were no differences in monofilament sensation between age groups, which is in contrast to findings by Rinkel et al, who reported age-related changes in monofilament sensation among healthy individuals in the age range 20.8–89.8 years, arranged into 7 groups, each with a 10-year span (36). The apparent discrepancy in monofilament sensation and age could possibly be explained by the use of different test locations in the 2 studies. Rinkel et al. used 5 locations: the pulp of the first and fifth toes, medial heel, first web, and lateral foot, chosen in concordance with the nerve distribution of the foot. In the present study 3 locations were used; plantar surface of the first metatarsal bone, the fifth metatarsal bone and the centre of the plantar surface of the heel, chosen as points playing a role in detecting weight distribution on the soles of the feet.
According to multivariate logistic regression models, by having 2 or more fast eye beats on the HST, the risk of a wrist fracture increased 5 times. With each additional g needed to sense plantar pressure the risk of being in the wrist fracture group increased almost 4 times, and with each additional µm needed to sense plantar vibration the likelihood increased 18%. These associations were independent of postural control, perceived dizziness handicap and confidence, walking speed or lower limb muscle strength. We also found a positive association between lower limb functional muscle strength and fall-related wrist fracture. With each additional second on the FTSTS the likelihood of being in the fracture group increased 2 times.
Given the importance of prevention of falls and wrist fractures, these variables represent potential targets for future interventions. In the current emergency care settings in Iceland, people aged 50–75 years, who have sustained a fall-related wrist fracture, receive treatment for the fracture. Postural control, vestibular function, sensation in the feet and lower-limb strength are usually not evaluated. Future studies are necessary to investigate whether training that facilitates the vestibular, somatosensory and physical functions can decrease the incidence of recurrent falls and fractures.
To the best of our knowledge, no previous studies have compared the function of the sensory systems, postural control and functional abilities between individuals with and without a fall-related wrist fracture, matched according to age, sex and weekly physical activity level.
However, it should be noted that an observed association in a case-control study does not necessarily imply causality. Future epidemiological studies with a longitudinal design or intervention studies are needed to confirm these findings.
People with wrist fracture have a higher incidence of asymmetrical vestibular function, reduced plantar pressure sensation and poorer standing and dynamic postural control compared with matched controls. Asymmetrical vestibular function and reduced plantar pressure sensation could be important contributing factors to falls and subsequent wrist fractures among the ageing population.
This study was funded by the St Josef’s Hospital Fund, Reykjavik, Iceland, the Icelandic Physiotherapy Association Research Fund, the Landspitali University Hospital Research Fund, the Icelandic Gerontological Society Research Fund and the Helga Jonsdottir and Sigurlidi Kristjansson Geriatric Research Fund.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize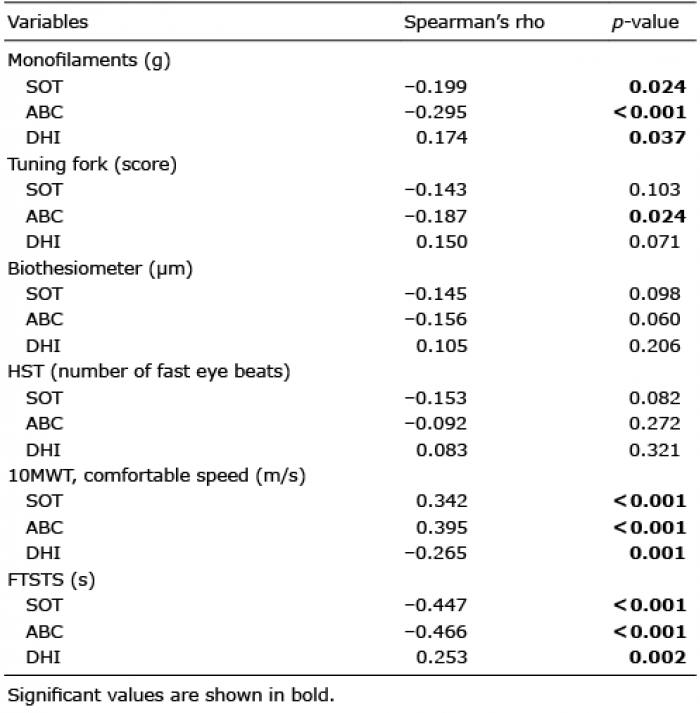 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize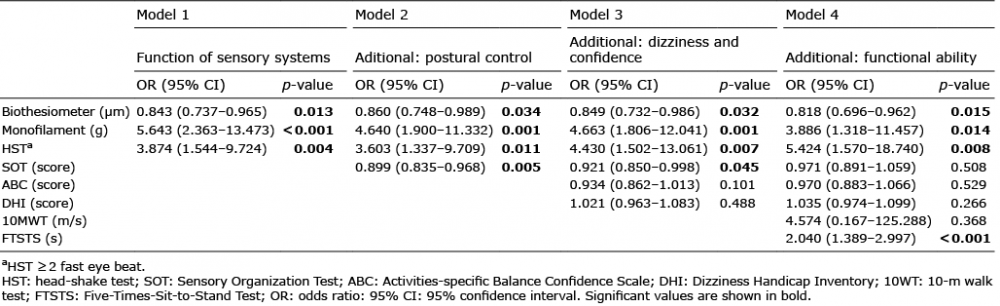 Click to show fullsize
Click to show fullsize