
From the 1Faculty of Medicine, and 2Department of Rehabilitation Medicine, MS Center Amsterdam, Amsterdam Public Health Research Institute, VU University Medical Center, Amsterdam, The Netherlands
Objective: To investigate whether aerobic capacity explains the level of self-reported physical activity, physical functioning, and participation and autonomy in daily living in persons with multiple sclerosis-related fatigue.
Design: A cross-sectional study.
Patients: Sixty-two participants with multiple sclerosis-related fatigue.
Methods: Aerobic capacity was measured with a leg ergometer and was expressed as maximal oxygen uptake (VO2max, in ml/kg/min). Physical activity was measured with the Physical Activity Scale for Individuals with Physical Disabilities (PASIPD), physical functioning with the Short Form 36 – physical functioning (SF36-pf), and participation and autonomy in daily living with the Impact on Participation and Autonomy questionnaire (IPA). Multiple regression analyses were performed, adjusted for potential confounders (gender, age, body mass index, educational level, and employment status).
Results: Mean maximal oxygen uptake (VO2max) was 23.9 ml/kg/min (standard deviation (SD) 6.3 ml/kg/min). There was no significant relationship between VO2max and physical activity (PASIPD): β = 0.320, 95% confidence interval (95% CI) = –0.109 to 0.749, R2 = 10.8%. Higher VO2max correlated with better physical functioning (SF36-pf): β = 1.527, 95% CI = 0.820–2.234, R2 = 25.9%, and was significantly related to IPA domains “autonomy indoors” (β = –0.043, 95% CI = –0.067 to –0.020, R2 = 20.6%), “autonomy outdoors” (β = –0.037, 95% CI = –0.062 to –0.012, R2 = 18.2%) and “social life and relationships” (β=–0.033, 95% CI = –0.060 to –0.007, R2 = 21.3%).
Conclusion: Maximum aerobic capacity was severely reduced in persons with multiple sclerosis-related fatigue. This partly explains the limited physical functioning and restrictions in participation and autonomy indoors, outdoors and in social life and relationships in these persons.
Key words: multiple sclerosis; aerobic capacity; physical functioning; participation; physical activity.
Accepted Nov 15, 2017; Epub ahead of print Jan 9, 2018
J Rehabil Med 2018; 50: 00–00
Correspondence address: Heleen Beckerman, Department of Rehabilitation Medicine, VU University Medical Center, PO Box 7057, NL-1007 MB Amsterdam, The Netherlands. E-mail: h.beckerman@vumc.nl
Multiple sclerosis (MS) is a neurodegenerative disease of the central nervous system (CNS). The major pathological mechanisms that cause clinical manifestations are inflammation, axonal degeneration and demyelination (1). Although the aetiology of MS is poorly understood, evidence points to a role for immunological, genetic and environmental factors (1). MS mainly affects young and middle-aged people, with women twice as likely to be affected as men. MS causes a variety of clinical symptoms, such as neurological impairments, fatigue, depression and pain (1, 2).
Fatigue is one of the most often reported and disabling symptoms of MS, and restricts societal participation and performance in daily life at home, at work and in leisure activities (3). When the contextual energy demands of daily activities and societal participation in fatigued persons with MS approach their aerobic capacity, participation is likely to be restricted. Fatigue is suggested to occur if the oxygen consumption of daily activities over an 8-h day demands more than 40–50% of an individual’s maximal aerobic capacity (4). Cardiopulmonary fitness is related to the ability of large muscles to perform dynamic, moderate-to-high intensity exercise for prolonged periods. Performance of such exercise depends on the functional state of the cardiovascular, respiratory, and skeletal muscle systems (5). Maximal oxygen uptake (VO2max) is accepted as the criterion measure of cardiopulmonary fitness, and defines a person’s aerobic capacity (6).
In people with severe MS-related fatigue, the possible relationship between aerobic capacity and physical activity and participation in daily living has received little attention to date. Persons with MS are less physically active in daily living compared with healthy peers. It has been suggested that demographic characteristics and MS severity are more relevant than cognitive-behavioural and social support variables in determining a patient’s physical activity (3, 7). In physically disabled persons, the threat of a downward deconditioning spiral is obvious. Aerobic capacity may affect physical activity and participation in daily living and, in turn, physical activity and participation in daily living may affect aerobic capacity. In addition, over the life-span, ageing leads to a decrease in maximal aerobic capacity of 5 ml/kg/min per decade (4). Depending on the living environment and the degree of social support available, independent living requires at least a maximal aerobic capacity of approximately 15–18 ml/kg/min (4). Understanding the energy cost of daily tasks and physical functioning relative to aerobic capacity may provide insight into the importance of an individual’s aerobic capacity for physical activity, societal participation and an autonomous independent living (8, 9).
The aim of this study of severely fatigued patients with MS was to investigate whether aerobic capacity compromises their physical activity, physical functioning and participation in daily living. First, we expected that the aerobic capacity in fatigued patients with MS is smaller than in age- and sex-matched healthy peers. Secondly, we hypothesized that patients with a lower aerobic capacity are also less physically active, show reduced physical functioning, and would be less autonomous in societal participation taking place outdoors.
This cross-sectional study used baseline data from a single study centre of the Treating Fatigue in Multiple Sclerosis – Cognitive Behavioural Therapy randomized clinical trial (TREFAMS-CBT) (10). For the present correlational study we did not perform a separate sample size calculation. Only patients with primary MS-related fatigue were included in this study. Aerobic capacity was measured with the cardiopulmonary exercise test (CPET). Patients were also asked to complete 3 questionnaires on levels of physical activity and participation in daily living.
The medical ethics committee of the VU University Medical Center approved the TREFAMS-ACE program (METc VUmc no: 2010.289). In addition, local feasibility statements were obtained from each participating medical centre (Central Committee on Research involving Human Subjects CCMO NL33451.029.10).
Participants received written and oral information about the study objectives, and the goals and possible risks of testing their aerobic capacity in the context of the Treating Fatigue in MS study. In addition to general patient information letter, study participants received a manual in which all test procedures were explained. All patients gave their written informed consent prior inclusion in the study.
Patients participating in the TREFAMS-CBT trial had to fulfil the following inclusion criteria: (i) a definitive diagnosis of MS; (ii) be severely fatigued (Checklist Individual Strength 20r, subscale fatigue ≥35); and (iii) had to be ambulatory (an Expanded Disability Status Scale (EDSS) score ≤ 6; able to walk at least 100 m using no more than 1 single-sided walking aid). Exclusion criteria were: (i) evident signs of an exacerbation, or a corticosteroid treatment in the past 3 months; (ii) current infections; (iii) anaemia; (iv) thyroid dysfunction; (v) depression (Hospital Anxiety and Depression Scale, subscale depression >11); (vi) primary sleep disorders; (vii) severe co-morbidity (Cumulative Illness Rating Scale item scores ≥3); (viii) current pregnancy or gave birth in the past 3 months; (ix) pharmacological treatment for fatigue initiated in the past 3 months (e.g. amantadine, modafinil, ritalin, pemoline); and (x) non-pharmacological therapies for fatigue that took place in the past 3 months (10).
To evaluate aerobic capacity, participants performed a CPET on an electromagnetic bicycle ergometer (Corival, Lode, Groningen, the Netherlands). The gas exchange of each patient was measured using breath-by-breath analysis (Quark CPET, COSMED, Rome, Italy). VO2max, defined as the rate of oxygen consumption required to move a kg of body weight per min, was calculated from gas exchange, and expressed in ml/kg/min (11). VO2max can be considered a valid measure of aerobic capacity, in at least ambulant persons with MS (12). In the present context, VO2max was defined as the highest recorded 30-s mean during the final 2 min of exercise. In fact, the most common primary criterion for attainment of maximum aerobic capacity in adults is a VO2 plateau despite a further increase in work rate. As only one-third of healthy persons are able to reach a VO2 plateau, secondary criteria are often added (12). Therefore, the respiratory exchange ratio (RER) was also measured; this is the ratio of CO2 produced and O2 consumed in 1 breath, and increases with workload (13). Heart rate (HR) was measured continuously with a heart rate monitor (COSMED, S.r.l, Rome, Italy). Patient measurements commenced in a sitting position at rest for 3 min, after which the patient performed a 3-min warm-up by cycling at ≥ 60 rpm with a workload of 25 Watts (W). After the warm-up, the workload progressively increased each minute by 10 W for women and 15 W for men. The patients continued to cycle at a cadence of ≥ 60 rpm throughout the test. The exercise test was terminated due to volitional exhaustion, a cadence < 45 rpm or for safety reasons; stopping criteria compliant with the American College of Sports Medicine guidelines for clinical exercise testing (5). At the end of the CPET, participants were asked to rate their perceived exertion on the validated Borg Scale, which rates from 6 (“no exertion at all”) to 20 (“maximal exertion”) (14). The secondary maximal exercise criteria are met at a perceived exertion ≥ 17 on the Borg scale, an RER > 1.10, or an HR within 90% of calculated maximal HR (220 – age, in years) (11, 12). To draw inferences from the VO2max in fatigued patients with MS, their scores were compared with recently published age- and sex-matched VO2max values of healthy persons (15).
Participants completed 3 questionnaires concerning their physical activities and participation in daily living: the Dutch versions of the Physical Activity Scale for Individuals with Physical Disabilities (PASIPD) (16–18) and the Short Form 36-physical functioning (SF36-pf) (19, 20), and the Impact on Participation and Autonomy, originally a Dutch questionnaire (IPA) (21, 22).
PASIPD. The PASIPD calculates physical activity on the basis of the number of days and hours of daily participation in recreational, household, and occupational activities, over the past 7 days. The PASIPD score is generated by multiplying the mean number of hours per day for each item by a metabolic equivalent (MET) value and then summing over the items (18). One metabolic equivalent (MET) is defined as the amount of oxygen consumed while sitting at rest and is equal to 3.5 ml O2/kg body weight/min. The MET concept represents a simple, practical, and easily understood procedure for expressing the energy cost of physical activities as a multiple of the resting metabolic rate (23). METs are a useful and convenient way to describe the intensity of a variety of physical activities (17). Light physical activity is defined as requiring < 3 METs, moderate activities 3–6 METs, and vigorous activities > 6 METs. The PASIPD was translated into Dutch, question 10 (lawn work or yard care) and 11 (outdoor gardening) of the original questionnaire were integrated into a single question, since this better represents the Dutch situation (17). The total PASIPD score ranges from 0 to 182.3 MET h/week (17). The PASIPD test–retest reliability and criterion validity are comparable to well-established self-reported physical activity questionnaires from the general population (17). In addition to the total score, 3 domains were identified in the PASIPD: i. Leisure time activities; ii. Household activities; and iii. Work-related activities.
SF36-pf. The SF36-pf subscale is a generic outcome measure designed to examine a person’s perceived limitation in physical functioning. The SF36-pf seeks to evaluate whether an individual is limited by their health in physical functioning, and as such is useful for measuring physical functioning in patients with MS (20). The SF36-pf consists of 10 questions, with a total score that ranges from 0 to 100. A higher score represents better physical functioning (19).
IPA. The IPA assesses autonomy and participation as perceived by the individual. It has been reported to be a reliable and valid instrument in patients with chronic disorders (21). The participation domains include: autonomy outdoors (e.g. visiting friends, leisure time; 7 questions), autonomy indoors (e.g. self-care; 5 questions), family role (e.g. housework; 7 questions), social relations (7 questions), paid work and education (6 questions). On every question, the perceived participation is rated as “0 = very good”, “1 = good”, “2 = fair”, “3 = poor” or “4 = very poor” (21, 22). The total mean score on each IPA domain ranges from 0 to 4, with higher scores representing poorer participation and autonomy (22).
Gender, age, body mass index (BMI), educational level and employment status were considered as potential confounders of the relationship of aerobic capacity and physical functioning and participation, because it has been described that in healthy persons aerobic capacity is higher in men than in women, is decreased in the later years of life, and is lower in people with a higher BMI (15, 24, 25). With regard to physical activity, levels are higher in males, at a younger age, with higher educational levels, with higher income status, and a lower BMI (25, 26).
Socio-demographic variables (e.g. gender, age, educational level and employment) were provided by the participants. Educational level was classified into 3 groups (high, moderate and low educational level) according to the Dutch conversion of the International Standard Classification of Education (27). Disease severity was determined by an experienced rehabilitation physician using Kurtzke’s Expanded Disability Status Scale (EDSS) (28).
The statistical analyses were conducted using SPSS, version 20.0 (SPSS Inc., Chicago, IL, USA). Multiple regression analyses of VO2max and PASIPD, of VO2max and SF36-pf, and of VO2max and IPA domains were carried out. In each of the 7 regressions models, VO2max was used as (independent) explanatory determinant, and the total scores and/or sub-scores of the questionnaires were used as (dependent) outcomes. Potential bias due to the confounders gender, age, BMI, educational level, employment (unemployed persons vs persons working full-time or part-time, and students) was investigated. Confounders were included in the final regression models if they caused a 10% change in the univariate regression coefficient of VO2max. The linear regression models were checked for any violations of the assumptions of normality, linearity, and equality of variances.
Three trial participants were excluded from the analyses. In one participant, the CPET was medically contraindicated. Furthermore, during warming-up on the bicycle it was noticed that 2 participants were unable to reach the required 60 rpm, and the CPET was discontinued.
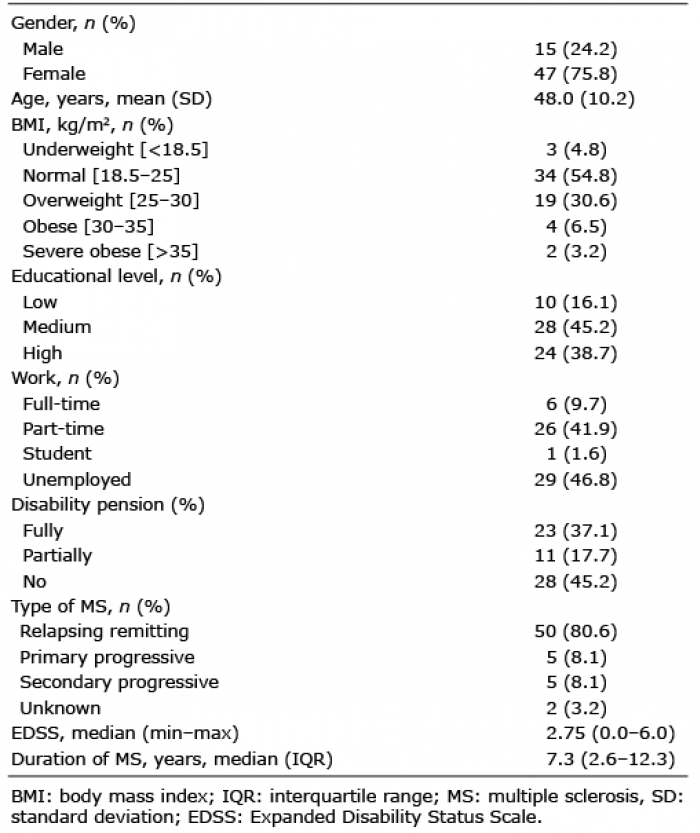
Of the 62 participants included, 15 were men and 47 women. The mean age for all participants was 48.0 years (SD 10.2 years) and the median duration of MS was 7.3 years (IQR 2.6–12.3 years). The median EDSS score was 2.75 (minimum 0.0, maximum 6.0) and 50 participants had MS of the relapsing remitting type. Socio-demographic characteristics are presented in Table I.
Table I. Demographic and disease characteristics of the participants (n = 62)
The mean VO2max was 23.9 ml/kg/min (SD 6.3 ml/kg/min), with a mean maximal HR of 152.5 bpm (SD 18.5 bpm) (Table II). The median Borg score was 17 (IQR 15–19). None of the participants experienced temporary deterioration of their MS symptoms or other adverse events after the CPET.
Table II. Scores on cardiopulmonary exercise test, Physical Activity Scale for Individuals with Physical Disabilities, Short Form 36-physical functioning, and Impact on Participation and Autonomy questionnaire
Table III shows the difference between the mean VO2max in healthy people and in the participants with MS. The VO2max of patients with MS was lower than age- and sex-specific reference data of a healthy population of Norwegian men and women aged 20–90 years (15). In this healthy reference group, exclusion criteria were cancer, cardiovascular disease, obstructive lung disease and use of blood pressure medication. Maximal levels of VO2 were measured during treadmill running, using an individualized graded protocol (15). Participants with MS achieved a VO2max of between 38% and 103% of the VO2max in their age- and sex-matched reference group (15).
Table III. Maximal oxygen uptake (VO2max) of the 62 patients with multiple sclerosis (MS)-related fatigue compared with reference values of healthy individuals
None of the participants reached a VO2 plateau despite an increasing workload. As to the secondary criteria, 39 (63%) participants achieved a score of ≥ 17 on the Borg scale, 36 (58%) participants achieved an RER of >1.10, and 29 (47%) participants reached an HR within 90% of the calculated maximal HR. Only one participant did not achieve any of these criteria. Of the 5 participants using beta-blockers, 4 did not achieve 90% of the maximal calculated heart rate.
The median total score on the PASIPD was 12.80 MET h/week (minimum 0.44, maximum 39.08). Most MET hours were achieved with leisure-time activities and the least with work-related activities. The median score on the SF36-pf was 60 (range 15–95). The IPA scores showed that work and education are the most affected and that autonomy indoors was the least affected domain in our study population. The PASIPD, SF36-pf and IPA scores are shown in Table II.
The results of the multiple regression analyses are shown in Table IV. We investigated the relationships between VO2max and 7 outcomes (PASIPD, SF36-pf and IPA (5 domains)). A significant, for confounding adjusted, relationship was found between VO2max and SF36-pf and the IPA domains “autonomy indoors”, “autonomy outdoors” and “social life and relationships”. A trend towards significance was noted for the relationship between VO2max and IPA domain “family role”. VO-2max was not significantly related to PASIPD or the IPA domain “work and education”. VO2max explained 10.8–25.9% of the variance in the self-reported levels of physical activity, physical functioning and participation (Table IV, and Fig. S11).
Table IV. Multiple regression analyses with the Physical Activity Scale for Individuals with Physical Disabilities, Short Form 36-physical functioning, and Impact on Participation and Autonomy questionnaire as outcomes
This study investigated the aerobic capacity of patients with MS compared with an age- and sex-matched healthy reference group, and the relationship between aerobic capacity and the self-reported level of physical activities and participation in daily living of severely fatigued patients with MS. We expected that patients with a lower aerobic capacity would also be less physically active, would show reduced physical functioning and would be less autonomous in terms of societal participation taking place outdoors.
First, we have shown that maximal aerobic capacity (i.e. the maximal amount of oxygen that a person is able to use for physical activities) is severely reduced in fatigued persons with MS relative to age- and sex-matched healthy peers. In patients with MS, disease symptoms, such as muscle weakness, spasticity, or ataxia, might result in higher than normal energy expenditure during daily activities (8, 29). Therefore, the energy cost of daily activities and societal participation might easily approximate the maximal aerobic capacity.
Patients with MS can be limited in their performance of daily tasks and societal participation due to inadequate aerobic capacity. The direct relationships found in this cross-sectional study between VO2max and SF36-pf, and the IPA domains “autonomy indoors”, “autonomy outdoors” and “social life and relationships” seem to indicate this.
Nevertheless, no significant relationship was found between VO2max and self-reported physical activity as measured with the PASIPD. The opposite findings have been reported by Ceaser et al. (30), who found that healthy individuals with a higher estimated VO2max had higher MET h/week. We anticipated that this relationship would be the same for fatigued patients with MS. An initial explanation for this unexpected finding might be that MS impairment causes a higher than normal energy expenditure during daily activities (29). These impairments may have interfered with the relationship between VO2max and physical activity, since relatively higher energy expenditure generally leads to an increase in perceived fatigue and probably a reduced activity level (8, 9, 29). A second possible explanation is related to the intensity of physical activities. In the PASIPD, light physical activity is defined as requiring < 3 METs, moderate activities 3–6 METs, and vigorous activities > 6 METs. An earlier study in persons with MS showed that, according to international guidelines for regular physical activity, 64% (68/106) of the participants were insufficiently physically active and only 16.5% of the participants performed activities with a vigorous intensity (7). It is reasonable to suppose that patients with MS score most of their MET h/week on “light physical activities” and healthy participants relatively more on “vigorous activities”. Controlled for exercise volume, vigorous-intensity exercise is more effective in improving VO2max than light-intensity exercise in healthy adults (31). A third possibility is that PASIPD, as a self-reported questionnaire, may provide inaccurate scores. Van den Berg-Emons et al. (32) compared the score on the PASIPD with an activity monitor in patients with bilateral spastic cerebral palsy, meningomyelocele and spinal cord injuries. They found that daily duration of physical activity was overestimated by the PASIPD. This was especially true for persons with higher physical activity levels. In addition, recall questionnaires have previously been shown to lead to an overestimation of time spent on activities (33).
We found a positive relationship between VO2max and SF36 physical functioning, a result consistent with the study by Koseoglu et al. (34), in which they also showed that SF36-pf was related to the level of aerobic capacity in patients with MS. A positive relationship has also been found in patients with systemic lupus erythematosus (35) and in patients with congenital heart disease (36), which supports the results of the current study.
Aerobic capacity was significantly related to better participation in “autonomy indoors”, “autonomy outdoors” and “social life and relationships”.
Regarding autonomy indoors, a positive relationship between aerobic capacity and ADL in patients with MS was shown in an earlier study (36). Moreover, this study also added that VO2max was related to the way in which a person performed these activities in daily living (37).
The current study showed that a higher aerobic capacity resulted in less impact on autonomy outdoors. The IPA domain “autonomy outdoors” asks patients to rate perceived possibilities to visit friends and relatives, travel and make trips, spend leisure time, meet other people, and live life the way they desire (21, 22). In a study of 75- to 90-year-old community-dwelling persons, a poor physical performance on the 6-min walk test was associated with a more limited sense of autonomy outdoors (38).
However, we found no significant relationship between a higher aerobic capacity and less impact on participation in family roles. Six out of the 7 questions on the IPA domain “family role” are about activities in and around the house (21). The participants were asked if they are able to do things around the house, either done by themselves or by others, in the manner they wish. In the event of participants not performing these activities by themselves, a relationship with aerobic capacity is not necessarily a logical outcome.
The analysis of VO2max impact on participation in work and education was limited to the working part of our study population (n = 36). The questions about work and education did not apply to the other 26 participants. Therefore, the small regression coefficient found may be biased, and may underestimate the real association in the total population including those who have retired early or dropped out from the labour market due to their MS and/or impaired aerobic capacity. It might be interesting to investigate whether a reduction in aerobic capacity results in an early exit from the employment market (39).
The results of the current study may have the following implications for clinical practice. In rehabilitation medicine, physical strain is an important concept, because it reflects the relative intensity of daily activities. Physical strain is defined as the oxygen demand (VO2) of daily activities expressed as a percentage of VO2max. A higher aerobic capacity provides a greater aerobic reserve, and thus a larger margin for intermittent daily tasks, and may provide more energy for work and leisure over and above that required to perform routine daily activities (e.g. personal care, household activities, family role) (4, 8, 9). In our study population, the mean VO2max was 23.9 ml/kg/min, which equals 6.8 metabolic equivalents (METc), assuming that the resting metabolic rate in this population also equals 3.5 ml/kg/min. The energy demands of low, moderate and high intense daily tasks in elderly people were on mean 6, 8, and 9.4 ml/kg/min (9). Fatigue is likely to occur if daily activities over an 8-h day demand more than 40–50% of an individual’s maximal aerobic capacity (4, 8). With a mean VO2max of 23.9 ml/kg/min, middle-aged patients with MS would be able to sustain only a very limited range of activities requiring an energy expenditure of less than 2.7–3.4 METs.
Therapeutic measures aiming at reducing the energy demands of daily activities and or improving the aerobic capacity may both be ways to reduce the physical strain. Systematic evidence in patients with MS suggests that progressive endurance training and high-intensity aerobic exercise training can boost the aerobic capacity by at least 3.5 ml/kg/min, potentially delaying worsening of physical functioning and societal participation and individual autonomy (12). Furthermore, it is likely that regular aerobic exercise programmes make a clinically useful contribution, not only in enhancing cardiorespiratory fitness, but also in preventing a further decline in various other components of physical fitness.
A higher aerobic capacity was directly associated with a lower impact on social life and relationships. To the best of our knowledge, no previous study has evaluated the relationship between aerobic capacity and social life in persons with MS. Several randomized clinical trials have investigated the effectiveness of exercise interventions on social participation (40–42). These trials showed contradictory findings, with some studies suggesting that group exercise programmes, in isolation, may have contributed to some of the beneficial effects on socialization (40, 41). Obviously, it should be noticed that VO2max explained up to 26% of the total variance in our study population, leaving room for other modifiable and non-modifiable variables that may contribute in explaining the variability in self-reported physical activity, physical functioning, and participation and autonomy.
The main limitation of the current study is the cross-sectional nature, which precludes conclusions on the causality of aerobic capacity on physical activity, physical functioning and participation. The direction of the relationships found, might also be from physical activity, physical functioning and participation towards aerobic capacity. This study only included patients with severe primary MS-related fatigue. Almost all participants performed this maximum bicycle ergometer test for the first time. Only 2 of them reported that they had previously performed such a maximum exercise test many years previously. Therefore, the results of this study are valid for this subset of patients.
Arguably some of the participants did not reach their maximum aerobic capacity level. Aerobic capacity outcomes in these participants may be limited by neurological impairment and disability due to MS or their inexperience with the test, rather than by cardiopulmonary fitness (3, 43).
In conclusion, in persons with MS-related fatigue the maximum aerobic capacity is severely reduced. This partly explains the limited physical functioning and restrictions in participation and autonomy indoors, outdoors and social life and relationships in these subjects.
Funding. This study was part of the Treating Fatigue in Multiple Sclerosis: Aerobic Training, Cognitive Behavioural Therapy, Energy Conservation Management (TREFAMS-ACE) research programme, which was funded by The Fonds NutsOhra (grant number ZonMw 89000005). Trial registration. ISRCTN 58583714.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize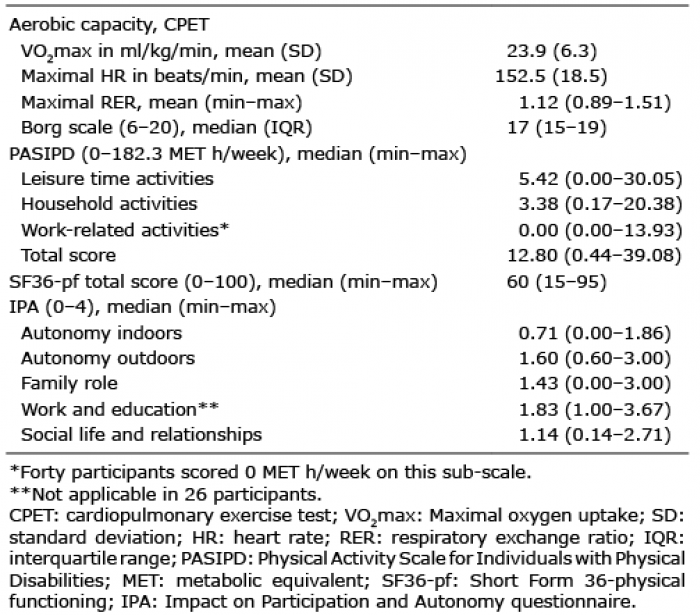 Click to show fullsize
Click to show fullsize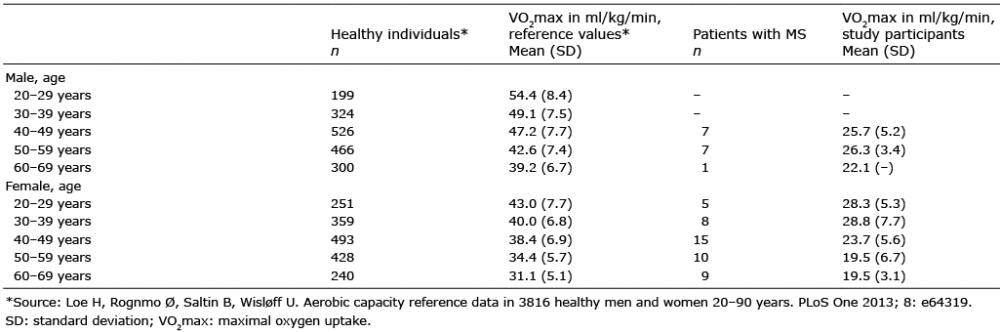 Click to show fullsize
Click to show fullsize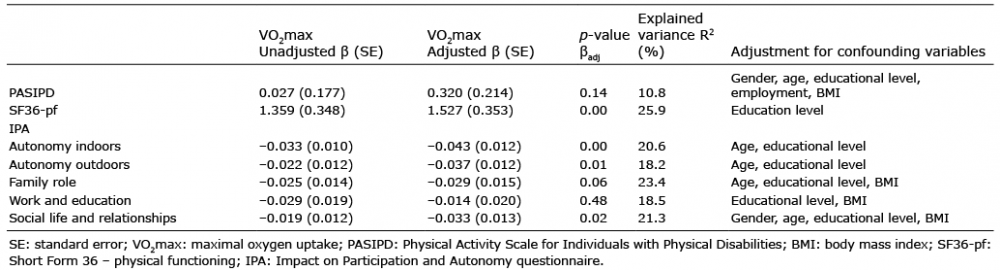 Click to show fullsize
Click to show fullsize