
From the 1Clinical Department of Rehabilitation Medicine, Region Östergötland, Linköping and 2Department of Clinical and Experimental Medicine, Faculty of Health Sciences, Linköping University, Linköping, Sweden
Objective: To explore whether bladder irrigation with chlorhexidine: (i) can reduce bacteriuria, and (ii) is a practically feasible option in subjects with spinal cord injury practicing intermittent self-catheterization.
Design: A prospective, non-controlled, open, multi-centre study.
Methods: Fifty patients with spinal cord injury, practicing intermittent self-catheterization, with a history of recurrent urinary tract infections were screened for bacteriuria at follow-up visits to 4 spinal cord injury centres in Sweden. Twenty-three patients had a positive urine culture (> 105 CFU/ml of > 1 bacterial species), of which 19 completed the study. Subjects proceeded with bladder irrigation, using 120 ml of 0.2% chlorhexidine solution twice daily for up to 7 days. Urine samples were taken twice daily. Response to treatment was defined as reduction in bacterial counts to < 103 CFU/ml.
Results: Fourteen of 19 subjects reduced their bacterial counts to or below the set limit. Subsequent return of above-endpoint bacteriuria was seen in most of the subjects. However, there were significantly fewer subjects with bacteriuria after treatment (p < 0.005).
Conclusion: Bladder irrigation with chlorhexidine, using intermittent self-catheterization, reduced bacteriuria in the majority of subjects with spinal cord injury and bacteriuria. The addition of bladder irrigation was practically feasible in the short time-frame of this study.
Key words: bladder irrigation; bacteriuria; clean intermittent catheterization; spinal cord injury.
Accepted Oct 30, 2017; Epub ahead of print Jan 22, 2018
J Rehabil Med 2018; 50: 181–184
Correspondence address: Madeleine Wikström, Clinical Department of Rehabilitation Medicine, Region Östergötland, SE-581 85 Linköping. E-mail: madeleine.wikstrom@regionostergotland.se
Spinal cord injuries (SCI) comprise a major subgroup of neurological disorders, which typically impair bladder storage and emptying. SCI may be congenital (e.g. myelomeningocele; MMC) or acquired. Acquired SCI may be traumatic or non-traumatic (e.g. due to infection, inflammation, neoplasia or vascular compromise). The neurological consequences of focal spinal cord lesions, regardless of aetiology, are summarized according to an internationally endorsed clinical classification system (1). Urologically, SCI typically leads either to a spastic or a flaccid bladder dysfunction. Intermittent catheterization (IC), either via the urethra or, more rarely, a continent urostomy, is advocated as an effective bladder management strategy in patients with neurogenic bladder dysfunction (2). IC, compared with indwelling catheters (transurethral or suprapubic), carries a lower risk of urinary tract infections (UTI), especially in subjects with SCI (3, 4).
Despite the current preference for IC as the bladder emptying method of choice, recurrent UTI is nevertheless a frequent complication among patients who practice IC (5). Patients with SCI may be significantly affected by a UTI, which can cause malaise, hyperpyrexia, abdominal pain, increased spasticity and symptoms of autonomic dysreflexia (4). In the long term, there is a risk of impaired kidney function (6).
Prevalence of bacteriuria and UTI varies widely in the literature. Publications indicate that 12–88% of subjects practicing IC have bacteriuria, but far from all develop symptomatic UTI (5, 7).
Sterilization of urine can be achieved, at least temporarily, by systemic antibiotic treatment, but concerns regarding overprescription of antibiotics demand restraints (8), not least in patients who are vulnerable to recurrent infections, such as those with SCI (9, 10). Thus, there is a need for antibiotic-sparing measures in UTI prevention and treatment. One such measure is bladder irrigation (BI) with bacteriostatic solutions (11, 12). A literature review yields inconclusive results: most previous studies were conducted on patients using indwelling catheters, rather than IC, and different irrigants were used in varying concentrations and regimes (13–17). Furthermore, objectives varied, e.g. UTI prevention, UTI treatment (13), risk reduction for catheter-associated UTI (CAUTI) (17) and reduction in bacterial counts (14, 15).
To complicate matters further, the distinction between “symptomatic” and “asymptomatic” UTI is difficult to define in many persons with bladder dysfunction secondary to neurological lesions, such as SCI. Due to diminished sensation, classic UTI symptoms, such as pain or discomfort at micturition, are typically lacking. Instead, patients may experience only unspecific symptoms, such as malaise, fatigue and/or increased spasticity. Since many patients with SCI have chronic bacteriuria, the stage is set for both over-diagnosing and under-diagnosing UTI (3, 18). Prophylactic treatment with low-dose antibiotics is currently recommended only in certain risk populations (8). However, preventing pathogenic bacterial colonization is advocated as a relevant way of preventing UTI (19, 20).
For the purpose of this study, antibiotic irrigants were not considered, since the aim was to study antibiotic-free methods of reducing bacteriuria. The most commonly used antiseptic irrigants are chlorhexidine digluconate and povidone-iodine, in varying concentrations (11). While the efficacy of short-time treatment regimens for preventing or eliminating UTI appears to be low (13, 14), some results indicate at least a temporary reduction in bacteriuria (14, 15). Chlorhexidine has a widespread use, and only negligible side-effects have been demonstrated following BI (15).
The present study was intended as an initial, explorative and hypothesis-generating pilot, in order to assess whether BI with chlorhexidine: (i) can reduce bacteriuria, and (ii) is a feasible option in subjects with SCI practicing IC.
This was a prospective, non-controlled, open, multi-centre study. The purpose was explorative and hypothesis-generating, aiming to assess primarily the practical feasibility of the intervention and its impact on pre-existing bacteriuria.
The target population comprised subjects with: (i) SCI, (ii) using IC as the chief method of bladder management, (iii) with asymptomatic bacteriuria, and (iv) a history of recurrent symptomatic UTI. For purposes of this study, “bacteriuria” was operationalized as a urinary culture with bacteriuria of > 105 CFU/ml of > 1 bacterial species (11) verified at a routine regular follow-up visit (where urinary culturing is included in the clinical pathway). Exclusion criteria comprised: (i) current symptomatic UTI requiring treatment; (ii) ongoing antibiotic treatment regardless of indication, (iii) known hypersensitivity to, or current use of, chlorhexidine and/or other instillation products; (iv) current pregnancy; and/or (v) current use of other local or systemic medications with urinary tract bacteriostatic/bactericidal effect (e.g. methenamine hippurate) (11).
A total of 50 otherwise healthy subjects with SCI were screened, 23 of whom had a positive urinary culture. Of these, 21 fulfilled the study criteria, and gave informed consent to participate in the study. Two of these subjects spontaneously (i.e. prior to start of BI) converted to urine bacteria levels below the set cut-off at the pre-treatment urinary culture, and were thus excluded from the study.
BI with chlorhexidine (Fresenius Kabi AB), was performed twice daily, in the morning and in the evening. The instilled solution was kept in the bladder for approximately 15 min, after which it was drained using IC. Urine samples for culture were taken just prior to and 3 h after, morning irrigation. Twenty out of 21 subjects performed the BI and the urine samples by themselves in their home settings, one out of 21 subjects had the irrigation performed by a trained study nurse while in hospital for SCI follow-up. The subjects were well informed and instructed according to the clinical study protocol and were contacted by phone after 2–3 days by study personnel, to ensure compliance to the study protocol and for safety monitoring. Subjects were treated as described and followed until: (i) their bacteriuria was reduced to or below the set cut-off, or (ii) otherwise up to 7 days. After completion, participation ended with a termination visit.
A pre-study power analysis was conducted, based on the assumption that at least 80% of subjects with bacteriuria would reach the set cut-off within a treatment period of 7 days. This resulted in a desired test sample of at least 22 subjects (80% power, p = 0.05). Descriptive statistics were calculated for each variable. The hypothesis was tested using an exact one-sided binomial test. In addition, the number of subjects with and without bacteriuria (according to defined thresholds), before and after treatment, were compared using McNemar’s test.
The local ethics committee in the Västra Götaland Region of Sweden approved this study for all participating centres (reference number 924–12).
Subject descriptors, including neurological classification and urological data, are summarized in Tables I and II.
Table I. Number of patients by sex and by outpatient/hospitalized
Table II. American Spinal Injury Association (ASIA), neurological level of injury and urological history
A total of 14/19 (74%) subjects reached reduction in bacteriuria to the set cut-off. Significantly fewer subjects had bacteriuria above this level after treatment (p < 0.005). Nine subjects reached reduction below cut-off after 1 initial irrigation. See Table III for details. Because of the time needed for analysing urinary culture samples, subjects reaching the endpoint continued to leave samples unaware of the obtained endpoint.
Table III. Time (days) to reduction in bacteriuria (<103 CFU/ml)
Table IV shows the proportion of subjects with subsequent return of bacteriuria above the cut-off level. Notably, 8 of the 14 subjects with reduced bacteriuria had a relapse above this level after just one day. Twelve subjects had ≥ 2 consecutive counts below this level.
Table IV. Return to > 103 CFU/ml and return to ≥ 105 CFU/ml any time after day 1, Before (n = 19)
A total of 7 adverse events were reported by 6 subjects: leakage of urine, cramping sensation in the bladder, increased urine leakage, diarrhea, and one instance of symptomatic UTI after treatment.
The results of this explorative study imply that adding BI with chlorhexidine to the IC bladder regime in subjects with SCI with bacteriuria (i) is practically feasible and without serious side-effects, at least in the short run, and (ii) may reduce bacteriuria. In addition, and in accordance with previous studies (14, 15), the present study suggests that sporadic irrigations may be insufficient for maintaining reduced bacteriuria.
The study design, small study sample, and absence of control group impose undisputable limitations as to the conclusions that may be drawn from this explorative study. Furthermore, the chosen cut-off level is admittedly arbitrary, and it is not even clear that a reduction in asymptomatic bacteriuria has any value in reducing the risk of symptomatic infections. Nevertheless, the findings of this pilot study do provide a rationale for performing larger, randomized studies of longer duration, where the usefulness or otherwise of BI with chlorhexidine as an adjunct to an IC regime as a means of reduction of symptomatic UTIs in subjects with neurogenic bladder dysfunction may be properly evaluated.
In conclusion, this explorative pilot study indicates that BI with chlorhexidine significantly reduces urine bacterial count in some subjects with neurogenic bladder dysfunction and a history of recurrent UTIs, and seems practically feasible as an add-on to IC, at least in the short term. As recurrent UTI is a challenge to many patients with neurogenic bladder dysfunction, any antibiotic-sparing option for the reduction of UTI is relevant. The results serve as an impetus for further research. Critically, it needs to be assessed whether a reduction in asymptomatic bacteriuria in fact leads to a reduction in frequency of UTIs. Future studies will also examine whether long-term treatment is necessary to reach a sustainable effect.
This study was sponsored by the company Wellspect HealthCare. The device is manufactured by Fresenius Kabi AB. The authors have no affiliation with any company with a direct or indirect financial interest in the subject matter discussed in this publication.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize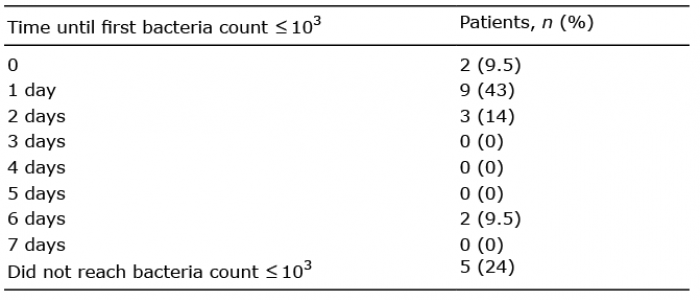 Click to show fullsize
Click to show fullsize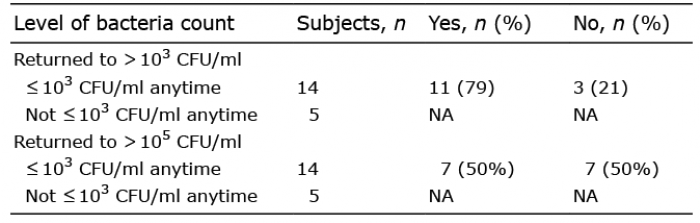 Click to show fullsize
Click to show fullsize