
From the 1Department of Physical Medicine and Rehabilitation, Innlandet Hospital Trust, Ottestad, 2Department of Research, Innlandet Hospital Trust, Sanderud, 3Department of Psychosocial Science, 4Department of Clinical Medicine, Haukeland University Hospital, University of Bergen and 5Department of Public Health, Høgskolen i Innlandet, Elverum, Norway
Objective: To assess the predictive effect of a multidisciplinary intervention programme, pain, work-related factors and health, including anxiety/depression and beliefs, on return-to-work for patients sick-listed due to musculoskeletal pain.
Design: A randomized clinical study.
Methods: A total of 284 patients were randomized to either a multidisciplinary intervention programme (n = 141) or to a less resource-demanding brief intervention (n = 143). Work participation was estimated monthly from register data for 12 months. Return-to-work was defined as increased work participation in 3 consecutive months.
Results: In the adjusted model, return-to-work by 3 months was associated with a multidisciplinary intervention programme (odds ratio (OR) = 2.7, 95% confidence interval (95% CI) = 1.1–6.9), the factor “belief that work was cause of the pain” (OR = 2.2, 95% CI = 1.1–4.3), anxiety and depression (OR = 0.5, 95% CI = 0.2–0.98), and by an interaction between the multidisciplinary intervention and perceived support at work (OR = 0.3, 95% CI = 0.1–0.9). At 12 months, only duration of sick leave was associated with return-to-work (OR = 0.6, 95% CI = 0.5–0.8).
Conclusion: Multidisciplinary intervention may hasten return-to-work and benefit those who perceive low support at work, but at 12 months only duration of sick leave at baseline was associated with return-to-work.
Key words: multidisciplinary rehabilitation; return-to-work; sickness absence; sick leave; randomized clinical trial; prognostic factors; musculoskeletal pain.
Accepted Oct 24, 2017; Epub ahead of print Dec 5, 2017
J Rehabil Med 2018; 50: 00–00
Correspondence address: Randi Brendbekken, Department of Physical Medicine and Rehabilitation, Innlandet Hospital Trust, 2312 Ottestad, Norway. E-mail: randi.brendbekken@sykehuset-innlandet.no
Musculoskeletal pain is a major cause of sickness absence and work disability worldwide. In Western countries, painful disorders of the back, neck and upper limbs are the most frequently reported causes, with work disability, long-term absence and permanent disability as consequences (1). The prevalence of sick certification and incapacity benefits due to these conditions has increased substantially in most Western countries in recent decades (2), while, in Norway, approximately half of all sickness absences are due to musculoskeletal pain (3). Most of these conditions are non-specific with little objective pathology, but research has revealed an extensive psychiatric and somatic comorbidity in this patient group (4). In a cohort of 635 patients on long-term sick leave, 55% had psychiatric-somatic comorbidity, with the combination of fibromyalgia/myalgia and depression being the most frequent (5).
Pain is a multidimensional phenomenon, comprising biological, psychological, social and existential elements. Thus, a number of predictors have been associated with the development and persistence of muscular pain. Some of these are work-related, such as physical demands at work or low job satisfaction, while others are psychiatric and affective risk factors, such as anxiety, expectations, fear avoidance or low mood (6, 7). To date, there is general consensus that chronic musculoskeletal pain conditions are multi-causal and comorbid (8), with multidisciplinary treatment being a recommended approach in the treatment of chronic pain (9, 10). The effectiveness of treatment with regards to health and quality of life could, however, differ from its effects on occupational outcomes. The literature on occupational outcomes has focused more on identifying predictors for disability than RTW among these patients (11, 12). Systematic reviews of the effectiveness of RTW programmes have concluded that knowledge, psychosocial, physical and work conditioning, possibly combined with relaxation exercises, are effective treatment components (12, 13). Studies of predictors of RTW have identified factors associated with the patient (functional ability, pain intensity, beliefs and expectations about recovery, RTW and low levels of education), the therapists (healthcare provider type, communication in therapy) and work (physical demands at work, job satisfaction, having unskilled work) (14, 15). In addition, depressive symptoms are associated with prolonged sick leave (16).
The process of RTW following a period of long-term sick leave reflects the complexity of the clinical picture, as medical, psychological, work and social factors often need to be addressed. This complies with the biopsychosocial model of disability. A multidisciplinary approach is recommended, but there is still no consensus on the content or dosage of these resource-demanding interventions. More information about the predictors of the effect of multidisciplinary programmes on RTW is needed (12) in order to tailor interventions and possibly avoid applying resource-demanding programmes to individuals who might benefit to the same extent from a more limited intervention.
A major motivation for this paper was the desire to analyse predictors for a more sustainable RTW on an individual level, with RTW defined as increased work-participation in 3 consecutive months, and to determine whether the 2 interventions had different effects on RTW defined in this way. In addition, the analysis aimed to determine whether patient- or work-related factors, measured at baseline, could predict (sustainable) RTW by 3 and 12 months’ follow-up. Former publications from this study have examined differences in improvements in health, physical functioning, coping and RTW between groups at 3 and 12 months’ follow-up (17, 18).
The aims of this study were, therefore (i) to assess the predictive effect of a multidisciplinary intervention (MI) vs the active comparator and less resource-demanding brief intervention (BI) on RTW in patients with long-term musculoskeletal pain problems; and (ii) to assess whether RTW in this group of patients is predicted by work-related factors and/or subjective experience of pain and health.
The study was a randomized clinical trial with a 12-month follow-up period, exploring the effect of 2 different interventions (MI and BI), including possible predictive factors on RTW, at the 3- and 12-month follow-up stages. The effects of the interventions on sick leave, RTW and secondary outcomes have been published elsewhere (17, 18).
Trial registration. The trial was registered at the US National Library of Medicine’s ClinicalTrials.gov (http://www.clinicaltrials.gov), registration number NCT01346423.
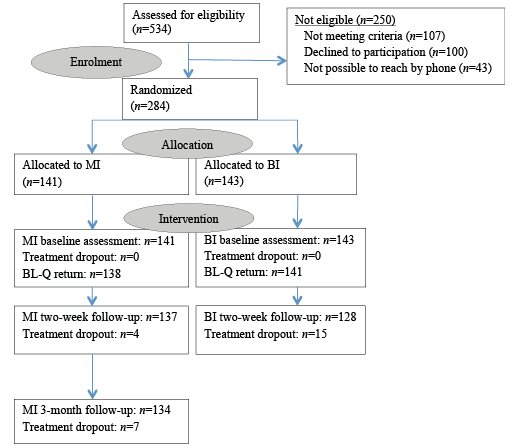
A total of 284 patients, with a mean age of 41.3 years, of whom 53% were women, were randomized to either MI (n = 141) or BI (n = 143) (Fig. 1). They were recruited from a list of patients who were on sick leave due to musculoskeletal pain and who were referred to the Department of Physical Rehabilitation, Innlandet Hospital Trust, Norway, in the period 2011–2013. Patients were referred by their general practitioner (GP) who had no knowledge that their patient might be enrolled on a clinical trial. Inclusion criteria were: age 20–60 years, at least 50% sick leave for no longer than 12 months due to musculoskeletal pain, and at least 50% employed. Exclusion criteria were: pregnancy, current cancer, osteoporosis, recent physical trauma/injury, serious mental illness, rheumatic inflammatory diseases, not capable of understanding and speaking Norwegian, or being involved in an ongoing health insurance claim.
On inclusion, all participants completed a comprehensive set of questionnaires before they received baseline treatment.
Fig. 1. Allocation and treatment flowchart. BL-Q: baseline questionnaire; MI: multidisciplinary intervention; BI: brief intervention.
All lawful residents of Norway are included in the Norwegian public insurance system. This system, which provides health service benefits and pensions, is administered by the Norwegian Welfare and Labour Administration (NAV). When a worker is certified sick by their GP, the workers’ compensation programme, administered by the NAV, provides 100% coverage for lost income from day 1 until the person can work again, for up to 52 weeks. The first 16 days are covered by the employer. After 1 year, the NAV covers long-term rehabilitation benefits or a disability pension, equating to approximately 66% of the person’s former income. These benefits can also be combined with work if the disability constitutes a minimum of 50%.
The MI included 3 consultations at the outpatient clinic: at baseline, after 2 weeks and after 3 months. The baseline assessment was the most comprehensive part, lasting approximately 3.5 h. The patient met each of the 3 members of the multidisciplinary team in succession, with each therapist assessing different aspects of the patient’s health and work situation, as follows. The social worker interviewed the patient about their work situation, family life, social life, education and economics. The physician interviewed the patient about their former and present health, and that of their family, and conducted a physical examination, which concluded with a diagnosis according to the International Classification of Diseases, 10th edition (ICD-10). The physiotherapist assessed the patient’s musculoskeletal problems and conducted a physical examination. In addition, the social worker and the physician collaborated with the patient using the novel Interdisciplinary Structured Interview with a Visual Educational Tool (ISIVET) (17). The ISIVET comprises a manual and 2 star plots with 7 axes. The first star plot, named “Working conditions”, evaluates 7 different aspects of the patient’s work situation, while the second star plot, named “Quality of life”, evaluates 7 aspects of health and social life. The evaluation itself involves a scoring process that results in a coloured area for each of the 2 star plots, thereby visualizing the resources (coloured area) and the challenges (non-coloured area) connected to the work and life situation. In this study, the 2 figures with their areas were central when the team and the patient, at the end of the baseline consultation, were evaluating the situation in order to make a rehabilitation plan. The main aim of the MI was to strengthen the patient’s motivation and ability to make changes in their own life and, in particular, choose activities and RTW in spite of the pain problems. Details of the ISIVET method are given in this randomized clinical trial (RCT) (17).
The patient had a follow-up with the physiotherapist after 2 weeks and with the whole team after 3 months. Both follow-ups lasted approximately 1 h and included working through the ISIVET once more, leading to an evaluation and, eventually, adjustment of the rehabilitation plan. The total face-to-face-time spent with the patient during the MI was 5.5 h.
The BI comprised 2 sessions: a baseline session lasting approximately 2.5 h, including separate consultations with a physician and a physiotherapist, and a 2-week follow-up with the physiotherapist for approximately 1 h. The BI applied in this study was based on a study by Molde Hagen (19). BI programmes have proven beneficial for low back pain, neck pain and fibromyalgia/widespread pain (20, 21).
The BI is based on a non-injury model, whose goal is to reduce fear and concern, as well as help the patient to stay active despite pain, unless serious pathology is identified, emphasizing the fact that the body is a strong and robust structure and that return to normal activity is beneficial. Essential features of the method include giving the patient time to express problems, worries and thoughts, followed by a thorough medical, educational examination, where any somatic findings are explained to the patient. The patient is informed about the positive prognosis and the importance of staying active. The total face-to-face-time spent with the patient during the BI was 3.5 h.
The comprehensive questionnaires at baseline comprised demographic variables, information on education and different aspects of work, self-ratings on health, fitness and physical activity, information related to the sick certification, and the duration and initial/actual extent of sick leave. The clinically validated questionnaires described below were applied.
The Subjective Health Complaints (SHC) inventory is a reliable instrument measuring somatic and psychological complaints over the previous 30 days using 29 questions rated on a 4-point scale (from 0 to 3) (22). The instrument has 5 subscales: “musculoskeletal complaints” (8 items), “gastrointestinal problems” (7 items), “pseudoneurological problems” (7 items) and “flu” and “allergy” symptoms (7 items in total), in addition to a total score (SHC total), with a maximum value of 87 indicating the highest possible level of complaints that can be measured by this instrument. The subscale “musculoskeletal complaints” correspondingly has a maximum value of 24. Cronbach’s alpha for musculoskeletal complaints = 0.65, gastrointestinal problems = 0.71, pseudoneurological problems = 0.70, flu = 0.65, allergy = 0.48.
The Hospital Anxiety and Depression Scale (HADS) assesses anxiety and depression disorders (23). HADS consists of 14 items that create subscale scores for anxiety (7 items) and depression (7 items) and a sum-score for both scales. The score for each subscale is calculated by adding the scores of the individual items (0–3) and ranges from 0 (good) to 21 (poor). Only the sum-score anxiety/depression was used in this study, and Cronbach’s alpha for this scale was = 0.86.
The Eysenck Personality Questionnaire-Nordic (EPQ-N) is a 12-item true-false questionnaire measuring neuroticism as a personality trait. The maximum score of 12 indicates a high degree of neuroticism. EPQ-N is derived from the 90-item EPQ (24), which measures neuroticism, psychoticism and extroversion. Cronbach’s alpha for EPQ-N=0.84.
The Chronic Pain Acceptance Questionnaire (CPAQ) is a 20-item assessment divided into 2 subscales: pain willingness (9 items) and activities engagement (11 items). The scores are set according to a numerical scale from 0 to 6 (highest degree of willingness or engagement), with the CPAQ sum has a maximum score of 120, indicating the highest possible level of willingness to tolerate pain and engage in activities measured by this instrument (25). Cronbach’s alpha for CPAQ sum= = 0.64, pain willingness = 0.81, activities engagement = 0.84.
Physical burden of work and psychological burden of work were assessed by the question: “Do you experience your work as a physical (correspondingly psychological) burden?” The 3 possible answers (yes, no, some) were dichotomized into “yes/some” = 1 and “no” = 0.
Perceived support at work was measured by 6 items from Theorell, while answers were made using a 4-point numerical scale from minimum support to highest degree of support (1–4), with a maximum score of 24, indicating high support at work from leaders and colleagues (26). Cronbach’s alpha for support at work = 0.82.
Burden of work was measured as the demands/control fraction of Karasek et al. (26), including questions on job demands (5 items) and questions on job control (decision latitude). The job control scale is the sum of 2 subscales: skill discretion (4 items) and decision authority (2 items). The answers are given on the range of 1–4, where 4 represents the most burdensome situation. Cronbach’s alpha for job demands = 0.73, skill discretion = 0.55 and decision authority = 0.78.
Regarding cause of the pain, the study participants were asked about what they believed was the cause of the pain problem, with the possibility of choosing a specific cause (e.g. actual work, strain at home, injury, leisure activity, incorrect treatment, deformity of the body or just “don’t know”).
The national register data was used to define the work/social insurance status in each calendar month after inclusion in the trial. The register data provided follow-up data on every participant in both treatment groups for 12 months of follow-up, as well as information on the GP diagnosis that led to sick certification at baseline. Every month of the follow-up period, each participant was either out of work, partly working or fully working. At baseline, due to inclusion criteria, they were either out of work or partly working. The status of every follow-up month was compared with the status in the baseline month for every participant and defined a “success month” as a month with increased work participation compared with the baseline, while a “non-success month” was a month with unchanged or decreased work participation compared with the baseline. If a person had 3 consecutive “success month” statuses, this was defined as RTW, with the first out of the 3 months defined as the RTW month.
The odds of RTW within 3 and 12 months, respectively, were analysed using binary multiple logistic regression models, including all the following a priori selected, independent variables (1–4):
1. Intervention variable (MI = 1 and BI = 0).
2. Variables that were dichotomized by splitting the median score (above median score = 1, median score and below = 0):
3. Variables dichotomized to either yes or no by the given answers:
4. Duration of sick leave was categorized into: 0–91; 92–153; 154–213; and 214–365 days.
For adjustment, the models also included sex and age (20–29; 30–39; 40–49; 50–60 years). Each predictor variable was assessed for interaction with the intervention in the models according to hierarchical elimination. The models’ goodness of fit was tested by the Hosmer-Lemeshow test. The significance level was set at 5% for all tests. The odds ratios (ORs) with 95% confidence interval (95% CI) are reported.
Baseline characteristics are shown in Table I. The mean duration of sick leave by inclusion was 147 days (SD 60.1 days). As there was some waiting time (1–2 weeks) from inclusion to baseline assessment, 8 patients (MI = 2, BI = 6) were no longer certified sick, but worked full-time at baseline. These patients were included in the analyses as non-RTW as they were unable to increase their degree of work participation compared with baseline.
Table I. Baseline characteristics of participants (n = 284) divided according to multidisciplinary intervention (MI) and brief intervention (BI)
The dominant diagnoses according to the International Classification of Primary Care 1998 (ICPC-2) (27) were low back pain (39.5%), neck pain (12.1%), widespread pain/fibromyalgia (10.7%) and shoulder pain (7.8%). The sample comprised a total of 51 different diagnoses, of these 238 (83.8%) were musculoskeletal diagnoses, while 14 (4.9%) were psychiatric diagnoses, 11 (3.9%) were neurological diagnoses, and 21 (7.4%) were other diagnoses. However, all patients were referred because of musculoskeletal pain problems. The ICPC diagnoses on the sickness certificates were available when we received the social insurance register data at the end of the study.
By the 3-month follow-up stage, 25.5% (n = 36) in the MI group and 20.3% (n = 29) in the BI group were categorized as RTW (p = 0.29). By the 12-month follow-up, the proportions were 63.8% (n = 90) and 58.7% (n = 84), respectively (p = 0.38).
The adjusted OR for RTW within 3 months in the MI group, compared with the BI group, was 2.69 (95% CI: 1.06–6.85), while it was 1.13 (0.67–1.91) within 12 months (Table II). RTW after 3 months was also significantly associated with believing that pain was caused by work (OR: 2.17, 95% CI: 1.11–4.26) and with anxiety/depression (OR: 0.45, 95% CI: 0.20–0.98). There was an interaction between intervention and perceived support at work (OR: 0.24, 95% CI: 0.07–0.85), indicating that those with low perceived support at work benefitted significantly more from MI compared with BI (Table III). For RTW after 12 months, duration of sick leave was the only significant predictor (OR: 0.63, 95% CI: 0.49–0.82). All interaction variables were eliminated from the 12-month model. Five baseline questionnaires (MI = 3, BI = 2) were never returned, and baseline information on these individuals were included as missing values.
Table II. Adjusted odds ratios (OR) and 95% confidence interval (95% CI) for return to work (RTW) by 3- and 12-month follow-up
Table III. Return-to-work (RTW) at 3-month follow-up, split by intervention and support at work (high vs low)
By the 3-month follow-up, patients who received the MI seemed more prone to RTW than patients who received the BI, adjusted for confounders and the other study factors. This result was not found 12 month follow-up. RTW was also predicted by believing that pain was caused by work, while anxiety and depression was a negative predictor. The subgroup reporting low support at work (LSW) (lower than median) benefitted more from the MI, compared with the BI, with an OR for RTW = 4.2 (95% CI = 1.2–14.2). This was the only study factor that interacted significantly with the intervention. By the 12-month follow-up, the duration of sick leave at baseline was a negative predictor for RTW.
Both interventions in this study are based on the biopsychosocial model of disability (28) and both practiced patient education. The MI, which had an additional 2 h therapist time and a social worker in the team, was a more comprehensive intervention than the BI, focusing on work in particular, as well as psychosocial factors and communication.
Reviews on the efficacy of MIs on RTW, compared with other treatment modalities, have shown conflicting results (10, 12, 13, 29). However, our findings are in accordance with studies in which a clinical intervention combined with an occupational intervention is associated with a faster RTW (30, 31). A recent Cochrane review concluded that workplace interventions reduce the time to RTW, as well as improve pain and functional status in workers with musculoskeletal disorders (32). This RCT found that the MI group improved more rapidly than the BI group in terms of physical and mental symptoms, along with reporting less use of health services and a better ability to cope (17). Van der Giezen et al. (33) found that interventions combining psychosocial aspects, health and work predicted RTW in chronic low back pain, which is in line with our results. On the other hand; the potential for increasing RTW rates by applying more extensive interventions, such as the MI, might be through the earlier mobilization of individuals who would have chosen to RTW at a later time, as the MI did not predict RTW by 12 months. From a 1-year perspective, this effect of a hastened RTW represented sustainable work participation.
Improved communication between patients and therapists can improve coping and outcomes (34). The application of the ISIVET could have contributed to our results on RTW, by supporting and encouraging the patient to choose work in spite of pain problems when areas on the star plot were large, or to apply for alternative work or employment when areas were small. The therapists argued that work is generally beneficial for health and well-being. The MI also included initiatives directed at improving the work situation, where relevant. These aspects of the MI may also explain why individuals with LSW benefitted more from an MI than a BI in terms of RTW.
More therapist time has proven beneficial in treatments for psychiatric disorders (35), but the differences are comprehensive. The additional 2 h of therapist time in the MI compared with the BI is unlikely to explain RTW differences between the groups on its own, given that the patients were mainly chronic pain patients with complex problems.
The participants in our study were referred by their GP to specialist treatment and, on average, had been certified sick for 5 months on entering the study. They presumably represented a selection of patients who are difficult to help in primary care. This could explain the relatively low rates of RTW by 3 months follow-up and could explain why a more comprehensive intervention was more effective than a BI. In a comparable RCT within specialist healthcare, patients with comprehensive problems were found to RTW at a higher rate after receiving an MI compared with those receiving treatment as usual (36).
Fear-avoidance beliefs and negative expectations are significant prognostic risk factors for improvements in relation to chronic pain and RTW (6, 37). Fear avoidance related to work has furthermore been found to be more prevalent among those experiencing chronic pain than acute pain (38). This could be associated with our own finding, that RTW within 3 months was predicted on the belief that work was the cause of the pain, given that this belief was a major reason behind leaving work, while the interventions applied contributed to a correction of this belief. Both interventions were based on the non-injury model (39), both practised patient education, and therapists argued that activity is beneficial as long as there are no signs of serious disease. The MI and BI are both designed to deal with fear-avoidance beliefs. The correction of these beliefs could explain why patients who believed that work was the cause of pain seemed to RTW more quickly.
Comorbidity in chronic musculoskeletal pain is extensive and influences chronicity and disability (4, 5). The presence of psychological distress, in particular, is a predictor for chronicity and disability (40). This corresponds to our findings that anxiety/depression at baseline was a negative predictor for RTW.
Duration of sickness absence is a well-known predictor of disability in chronic pain (40), which corresponds with our findings at 12 months.
The primary strengths of this study were its design, randomization (which allowed for comparable groups), relatively large sample size and use of register data, which provided us with information on work participation and sickness compensation for every patient for all months of follow-up. In addition, both treatments were based on written manuals and were easy to describe. As separate teams provided the MI and the BI, this reduced the possibility of mixing the 2 methods. The BI was well known to the therapists involved, who had recently been videotaped and quality assured in performing BI on another trial. The therapists performing the new MI participated in regular meetings and supervision to ensure adherence to the protocol and consistent practice of the method. The sick certificates were issued by the GP in cooperation with the patient, rather than by physicians on the study, reducing the possibility of a biased diagnosis. Finally, the dropout rate from treatment was low in both groups, indicating that the treatment was feasible in terms of clinical practice and that the results are reliable.
Education was omitted as an adjustment factor because information on education was reported inaccurate on questionnaires for 12% (MI = 7%, BI = 16%) of the study sample. This might be a weakness of this study, as level of education can be associated with outcomes (2). However; the possibility that the 2 groups differ significantly in terms of education level, is reduced by the randomization. Another limitation concerned the similarities in the 2 treatment methods. Both were short-term interventions based on a non-injury and biopsychosocial models for pain assessment, and both practised patient education. There was no use of audiotaping in order to ensure adherence to the protocol in this study; nor was there any blinding of patients or therapists for practical reasons. Audiotaping might have strengthened the study due to quality control of treatment teams.
The MI, focusing, in particular, on the work situation, appeared to hasten RTW in patients who were certified sick with musculoskeletal pain, and to be beneficial for those who perceive LSW, compared with the BI. However, from a 1-year perspective, there was no difference between the MI and BI regarding RTW. Patients who believed work was the cause of their pain were found to RTW faster in both groups. Psychiatric comorbidity was a negative predictor for RTW at the 3-month follow-up, as was duration of sick leave by baseline at the 12-month follow-up.
The MI, as applied in this study, represents a novel approach. Further studies are needed to draw conclusions about the effects of this method compared with those of BI.
The authors would like to thank Nina Konglevoll for quality assurance and data entry and health secretaries Ann-Helen Tårnby and Hanne Berntsen for their help in the inclusion process of this study. Thanks are also due to Eli Molde Hagen, whose initiative led to this clinical trial, and to the Innlandet Hospital Trust, Norway, which funded the study.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize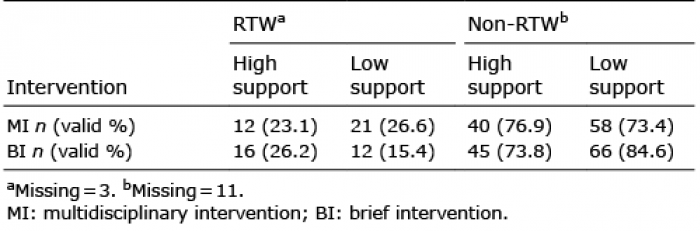 Click to show fullsize
Click to show fullsize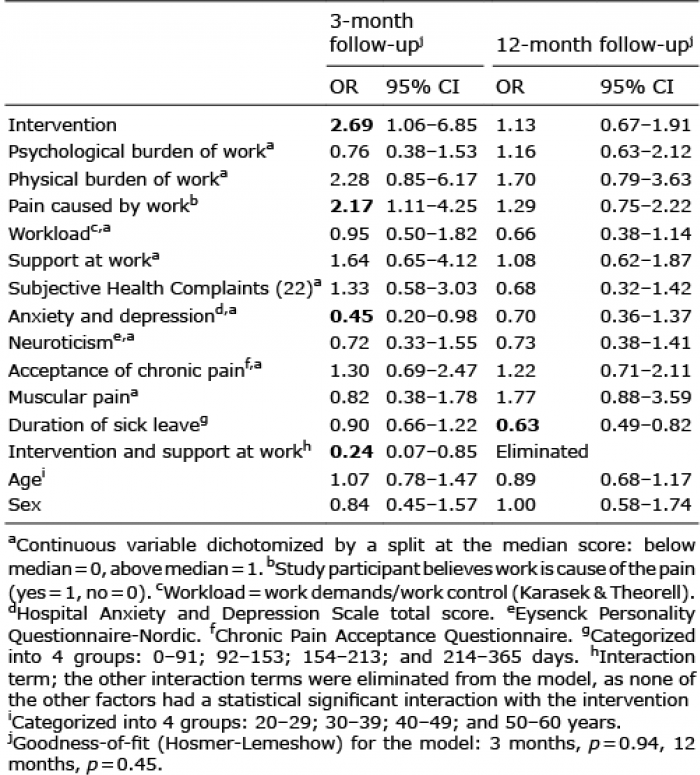 Click to show fullsize
Click to show fullsize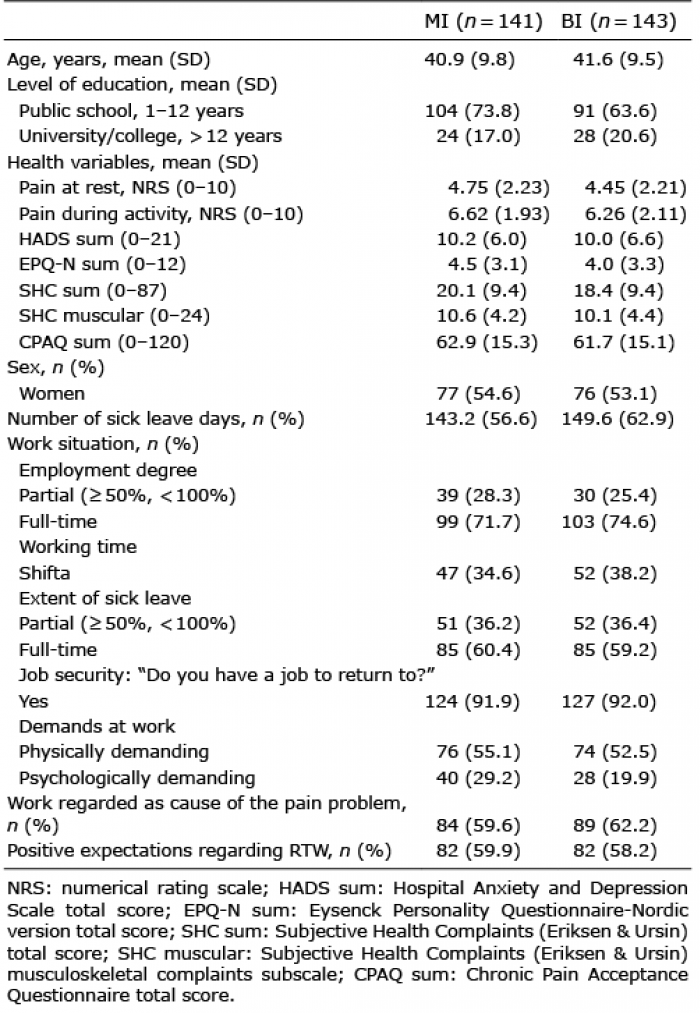 Click to show fullsize
Click to show fullsize