
From the 1Postgraduate College of Guizhou Medical University and Guizhou Provincial People’s Hospital, 2Nursing College of Guizhou Medical University, 3Department of Emergency Neurology, Affiliated Hospital of Guizhou Medical University, Guiyang City, Guizhou Province, 4Department of Endocrinology, First Affiliated Hospital of Jinan University, Guangzhou City, Guangdong Province and 5Department of Nursing Management, Guizhou Provincial People’s Hospital, Guiyang, Guizhou Province, China. #These authors contributed equally to this publication
Objective: To evaluate the mean treatment effect of mirror therapy on motor function of the upper extremity in patients with stroke.
Data sources: Electronic databases, including the Cochrane Library, PubMed, MEDLINE, Embase and CNKI, were searched for relevant studies published in English between 1 January 2007 and 22 June 2017.
Study selection: Randomized controlled trials and pilot randomized controlled trials that compared mirror therapy/mirror box therapy with other rehabilitation approaches were selected.
Data extraction: Two authors independently evaluated the searched studies based on the inclusion/exclusion criteria and appraised the quality of included studies according to the criteria of the updated version 5.1.0 of the Cochrane Handbook for Systematic Review of Interventions.
Data synthesis: Eleven trials, with a total of 347 patients, were included in the meta-analysis. A moderate effect of mirror therapy (standardized mean difference 0.51, 95% confidence interval (CI) 0.29, 0.73) on motor function of the upper extremity was found. However, a high degree of heterogeneity (χ2 = 25.65, p = 0.004; I2 = 61%) was observed. The heterogeneity decreased a great deal (χ2 = 6.26, p = 0.62; I2 = 0%) after 2 trials were excluded though sensitivity analysis.
Conclusion: Although the included studies had high heterogeneity, meta-analysis provided some evidence that mirror therapy may significantly improve motor function of the upper limb in patients with stroke. Further well-designed studies are needed.
Key words: stroke; upper extremity; recovery of function; rehabilitation; meta-analysis; mirror therapy.
Accepted Sep 26, 2017; Epub ahead of print Oct 27, 2017
J Rehabil Med 2018; 00: 00–00
Correspondence address: Yonghong Guo, Nursing College of Guizhou Medical University, 550025 Guiyang, China. E-mail: yonghong
0920@126.com and Guofeng Wu, Emergency Neurology in the Affiliated Hospita of Guizhou Medical University, No. 28, Guiyijie Road, Liuguangmen, 550004 Guiyang, Guizhou, China, E-mail: wuguofeng3013@sina.com
Stroke is a leading cause of morbidity and mortality worldwide (1–4). It commonly causes partial or total impairment of motor function of the upper extremity in survivors (5). More than 50% of stroke survivors have impairment of motor function of the upper extremity (6, 7) that seriously affects their life (8). There is clearly a need for stroke survivors to rebuild upper extremity motor function (9).
A variety of rehabilitation programmes that aim to promote motor function of the affected upper extremity in patients with stroke have been studied, e.g. constraint-induced movement (10), motor re-learning (11), electromyographic biofeedback (12) and robot-assisted therapy (13). Standard multi-disciplinary rehabilitation programmes for stroke survivors are challenging (14), labour-intensive and costly to carry out (15, 16). Mirror therapy (MT), a simple, cheap and less labour-intensive rehabilitation method (17), has been proposed as a promising rehabilitation approach for recovery of motor function of the upper limb in patients with stroke (18).
MT was first described by Ramachandran et al. as an effective method of relieving amputee pain (19). In their study, a mirror was placed vertically on the desk and the patient’s unaffected arm placed in front of the mirror, while the affected one was placed behind the mirror. Patients received visual feedback from the unaffected arm by watching its movement in the mirror, which was intended to make patients feel that their affected arm was restored.
MT was first used as a possible method to help stroke survivors rehabilitate motor function of the affected arm by Altschuler et al. (18). In their study, patients reported that it was helpful in improving the recovery of hand function. However, the sample size was small (9 participants) and outcome measurement was by subjective comments from patients, which may significantly impact on the generalizability of the result (20). Following Altschuler et al.’s study (18), further studies of MT in patients with stroke found that it had a positive effect on recovery of motor function of the upper limb (8, 16, 21–27). However, the mechanism of MT is not clearly understood (28). It has been proposed that MT promotes motor function of the upper extremity in stroke patients via activation of the primary motor cortex (M1) (29) or mirror neurones (30). However, some authors consider that the right superior temporal gyrus and the right superior occipital gyrus (31, p. 675) are facilitated during MT. In addition, some authors found that the activity of the precuneus and the posterior as well as cingulate cortex increased when stroke patients received MT, while no activation of M1 or mirror neurones was observed (32).
In recent years, an increasing number of randomized controlled trials (RCTs) have been performed to examine the effectiveness of MT on motor function of the upper limb in stroke patients (8, 16, 21–27). The mean treatment effect size of MT remains unclear (33), however, due to small sample size (20), and various characteristics of the target samples (i.e. different duration and severities of stroke). In this case, a meta-analysis could be used to combine and compare various studies to evaluate the mean treatment effect size (34). Although there are a few systematic reviews of the effectiveness of MT on motor function of the upper extremity (20, 33, 35, 36), they contain various limitations or underpowered issues in the empirical evidence. Only 1 systematic review (36) performed a meta-analysis to evaluate the mean effect of MT, while another 3 did not (20, 33, 35). In addition, there are some limitations in the search strategies in previous reviews. More importantly, since the evidence is continually updated, an updated meta-analysis is needed to provide the highest level of evidence (37) about the effect of MT on motor function of the upper extremity in patients with stroke.
The aim of the current study was to evaluate whether MT is effective in the recovery of motor function of the upper extremity in patients with hemiparesis following stroke and, if so, to explore the mean treatment effect size of MT on motor function.
Types of studies. RCTs and pilot RCTs that compared MT/mirror box therapy with other rehabilitation approaches were examined.
Participants. RCTs conducted in patients with hemiparesis after stroke, including either ischaemic or haemorrhagic subtypes defined by a recent definition updated by the American Heart Association/ American Stroke Association, were examined (38). Motor function of the upper extremity in stroke patients was impaired, as evaluated by the upper extremity part of the Fugl-Meyer Assessment (FMA-UE) (scores < 55 points) (39, 40). There were no limitations on age, sex, stroke lesions, severity levels, or time since onset of stroke. Patients with hemiparesis due to any other disease or trauma were excluded.
Types of intervention. MT or mirror box training/therapy, the intervention in the experimental group, was compared with conventional therapy or conventional rehabilitation in a control group. There are 3 strategies involved in performing MT (41): (i) patients attempt to simulate movements by using their impaired limb actively when they directly watch the reflection of movements of their good limb; (ii) participants need to imagine movements of their affected limb when moving their unaffected arm; and (iii) participants are assisted to move their impaired extremity in order to be synchronous with movements of the intact arm. The current meta-analysis included studies with no restrictions on the strategy of MT, the timing of the start of the intervention, or the duration of the intervention. However, studies were excluded if a different form of MT or other types of rehabilitation that were not routinely recommended for use in clinical settings were performed in the control group.
Outcome measures. The outcome was improvement in motor impairment evaluated with the FMA-UE.
Searches were performed for studies published in English in electronic databases, including PubMed (Publication year: within 10 years; Language: English; Article types: clinical trial; Species: human), Embase (Publication year: 2007–2017; Evidence based medicine: randomized controlled trials; Language: English), MEDLINE Complete (Date of publication: January 2007– June 2017; Language: English), Cochrane Library (trials; Publication year: between 2007 to 2017), and CNKI (2007–2017, English language). Key words used to search the literature were: (“stroke” OR “apoplexy” OR “cerebral stroke” OR “cerebrovascular stroke” OR “cerebrovascular apoplexy” OR “cerebrovascular accident”) AND (“recovery of function” OR “rehabilitation” OR “convalescence”) AND (“upper extremity” OR “upper limb” OR “membrum superius”).
All records were imported into Endnote X7 and duplicate records were removed. Two independent authors assessed the titles and abstracts of the records to remove irrelevant studies based on the inclusion and exclusion criteria. Then they classified the remaining records into “relevant” and “unsure” categories. Finally, the full-text articles of both “relevant” and “unsure” studies were searched. In case of disagreement, the 2 authors discussed the article and a third author was involved in the process of consensus and consultation.
When extracting data from primary studies, a customized form that included publication status (i.e. authors and year), sample size, demographic features (i.e. age, lesions of stroke, time since stroke onset, and severity of impairment of motor function), methods (i.e. randomization and blinding), interventions (i.e. intervention and duration), outcome measures, and findings. In case of disagreement, consensus between the 2 authors was used. Occasionally, the authors of the primary studies were contacted by email for clarification.
In order to appraise the quality of a study, 2 independent authors assessed the risk of bias according to the criteria of updated version 5.1.0 of the Cochrane Handbook for Systematic Review of Interventions (42). The main types of risk assessed according to the criteria were: risk of random sequence generation (selection bias), allocation concealment (selection bias), blinding of participants and personnel (performance bias), incomplete outcome data (attribution bias), selective outcome reporting (reporting bias), and other source of bias. In case of disagreement, the 2 authors would discuss the study in order to reach a consensus.
The objective was to combine and compare the primary studies to evaluate the effect of MT on motor function of the upper extremity in stroke patients. Thus, the outcome of interest from the original studies was imported into Review Manager 5.3 and Stata 14.0. Since the outcome was continuous data, the fixed effects model and the statistical method of inverse variance were chosen to compare MT intervention and conventional therapy. In addition, the standardized mean difference (SMD) and 95% confidence intervals (95% CI) were used to assess the mean effect size of MT. A χ2 test was used to analyse heterogeneity among studies. If heterogeneity was detected through the statistical test, Review Manager 5.3 was used to perform sensitivity analysis and Stata 14.0 to conduct moderator analyses (i.e. meta-regression and publication bias) to investigate the sources of heterogeneity (34). Statistical inference was identified as a p-value less than 0.05.
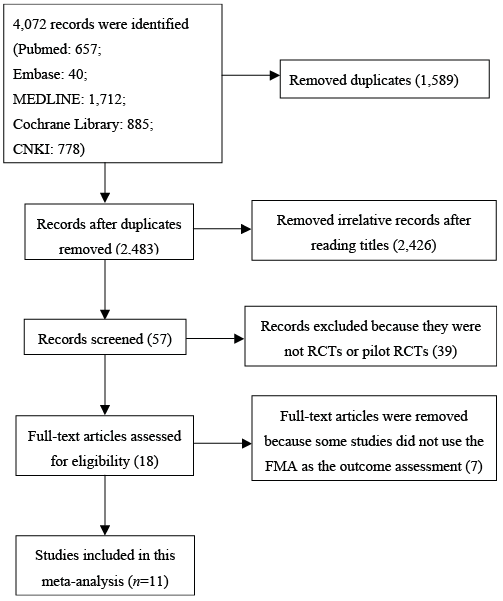
A total of 4,072 records were identified, of which 11 eligible trials (16, 24–27, 36, 43–47) were included in the final meta-analysis. Details of records searched and selection are shown in Fig. 1.
Fig. 1. Literature search and study selection.
FMA: Fugl-Meyer Assessment; RCT: randomized controlled trial.
The included studies were published between 2011 and 2017. A total of 347 patients were included, of whom 172 received MT and 175 underwent conventional or standard rehabilitation therapy. The characteristics of the 11 included trials are summarized in Table I. The mean age of the participants in different studies ranged from 45 to 64.9 years. The onset time of stroke in the included studies varied from less than 3 months to over 12 months.
Table I. Descriptive summary of characteristics of the 12 included trials
Seven studies (16, 24, 27, 43–46) were conducted in patients whose stroke onset time was more than 6 months, while the onset times of stroke in the other studies (8, 25, 26, 47) were less than 6 months. The total duration of the intervention in different studies ranged from 400 to 1920 min. Fig. 2 shows the authors’ judgements about the risks of bias for the included studies. In terms of random sequence generation, 8 studies (8, 25–27, 44, 45–47) randomized participants into experimental and control groups by computer-generated random numbers, random cards, a randomization table, or throwing dice, while the other 3 studies (16, 24, 43) did not report sufficient information about randomization.
Fig. 2. Authors’ judgements about each risk of bias item for included studies.
Performance biases of the 11 studies were high because of the nature of the trials. It was difficult to blind the participants and the researchers as to whether subjects had received MT. However, outcome assessors in most trials (8, 16, 24, 25, 27, 43, 44, 46) were blinded, while this factor was unclear in other 3 studies (26, 45, 47).
Fig. 3 shows the meta-analysis of the effect of MT on motor function of the upper extremity in patients with stroke. A medium effect size (SMD 0.51, 95% CI 0.29, 0.73) was detected for the effect of MT on motor function of the upper extremity and the value of test for overall effect was 4.58 (p < 0.00001).
Fig. 3. Forest plot of the fixed effects meta-analysis of mirror therapy (MT) on motor function of the upper extremity.
SD: standard deviation; 95% CI: 95% confidence interval.
The heterogeneity statistic was significant (χ2 = 25.65, p = 0.004; I2 = 61%). After the heterogeneity was detected, sensitivity analysis was used to exclude studies that might have caused the heterogeneity. This resulted in the heterogeneity decreasing dramatically (χ2 = 6.26, p = 0.62; I2 = 0%) when 2 trials (27, 45) were removed (Fig. 4).
Fig. 4. Sensitivity analysis for the effect of mirror therapy (MT) on motor function of the upper extremity.
SD: standard deviation; 95% CI: 95% confidence interval.
Moreover, meta-regression was used to investigate whether sample size, duration of MT and onset time of stroke caused the heterogeneity. Table II shows the result of the meta-regression. However, it was not determined whether sample size (p = 0.825), duration of MT (p = 0.267) or onset time of stroke (p = 0.517) might cause the heterogeneity (p > 0.05). In addition, no publication bias was detected (p >0.05) (Table III).
Table II. Results of meta-analysis regression
Table III. Results of publication bias
One of the main objectives of this meta-analysis was to investigate the mean treatment effect of MT on motor function of the upper extremity in patients with stroke. Eleven RCTs, with a total of 347 participants, were included to explore the effect of MT on motor function of the upper extremity. The SMD of MT on motor function of the upper extremity assessed by the FMA was 0.51 in our meta-analysis. Some authors could not draw a firm conclusion about whether MT could improve motor function of the upper limb over a long period (33, 35). This may be because they included case studies and non-randomized controlled trials as well as RCTs in their studies, and the heterogeneity among different types of studies prevented a firm conclusion being reached via statistical methods (33, 35). However, the results of the current meta-analysis showed that MT was significantly associated with immediately improved motor function of the upper extremity in patients with stroke. This finding was consistent with those of Thieme et al. (36) and Ezendam et al. (20), which suggested that MT may improve the motor function of the upper extremity in patients with stroke and could be used in clinical practice as a rehabilitation intervention (36). The possible mechanism of MT improving motor function was that the primary motor cortex (M1) was activated by visual feedback from the mirror when movement of the unaffected hand was performed (48). However, some authors argued that the activation was “the mismatch between the movement one performs and the movement that is observed” (43, pp. 11–12) and not the effect of mirror illusion.
However, there was a slight difference between our meta-analysis and the meta-analysis by Thieme et al. (36); for example, the effect size in our meta-analysis (SMD 0.51, 95% CI 0.29, 0.73) was smaller (36) (SMD 0.61, 95% CI 0.22, 1.00). A total of 14 studies were included in Thieme et al.’s study (36), all of which were published before 2011. Of the 14 studies in the former meta-analysis, only 1 (43) was included in our meta-analysis due to the inclusion/exclusion criteria. All of the studies included in our meta-analysis were published after 2011. Our meta-analysis investigated only the effect of MT on motor function of the upper extremity evaluated by the FMA. However, the former meta-analysis (36) synthesized outcomes of motor function of the upper limb, as assessed by the FMA, Action Research Arm Test (ARAT), and Wolf Motor Function Test (WMFT). Furthermore, studies included in our meta-analysis were RCTs, while Thieme et al. (36) included both RCTs and cross-over design studies. The difference in included studies may have led to the different outcomes between the 2 meta-analyses.
Despite the favourable outcome, the results of the included studies were variable, and a large heterogeneity was detected among the original studies (χ2 = 25.65, p = 0.004; I2 = 61%), which indicated that some factors may impact on the outcome of MT. Meta-analysis regression was used to investigate the factors (i.e. sample size, duration of MT and onset time of stroke) causing heterogeneity. In addition, publication bias was analysed. However, no factors that might cause the heterogeneity were detected.
It is possible that other factors, which were not analysed due to insufficient information, may contribute to the high heterogeneity in our meta-analysis, e.g. mean age of participants, and severity of motor impairment before intervention (Table I). The mean age of participants varied from 45 to 64.9 years in the studies in our meta-analysis. Although some authors concluded that age was not associated with the final outcome of rehabilitation (49), others argued that age was an important factor impacting the scores of motor function that were assessed at admission or at 5 years post-stroke (50). Similarly, Jongbloed (51) believed that older patients were less likely to have positive functional outcomes than younger ones. In addition, among the included studies participants had a different degree of severity, varying from Brunnstrom stage I to IV or above (Table I). A previous study found that baseline upper limb functional status was “consistently identified as being strongly associated with upper limb recovery following stroke” (49, p. 308).
Other factors may contribute to the high level of heterogeneity. First, the difference in risks of bias in the different studies might be an important contributor to heterogeneity. For example, in this meta-analysis, the risks of bias of random sequence generation in 3 studies (16, 24, 43) remained unclear due to insufficient information, while the other 8 studies (8, 25–27, 44–47) had low risks of bias in random sequence generation. Second, in terms of allocation concealment, only 4 studies (24, 27, 44, 49) had low risks, and 1 study (46) had high risks, while the others were unclear about the bias of allocation concealment. Third, as for blinding outcome assessment, 8 studies (8, 16, 24, 25, 27, 43, 44, 46) used an assessor blinded method, while the other studies were unclear (3). Finally, different MT strategies may also contribute to the heterogeneity in the current meta-analysis. As stated above, MT consists of 3 strategies. Participants in the MT group of 8 trials (8, 26, 27, 43–47) were asked to use their impaired limb directly to imitate movements of the unaffected limb in a mirror. However, subjects in the MT group of the other 3 trials (16, 24, 25) were required to mentally picture movements of their impaired extremity when watching movements of their unaffected limb. We hypothesized that such characteristics might contribute to the heterogeneity in this meta-analysis.
Sensitivity analysis revealed that the heterogeneity decreased dramatically if we excluded 2 studies (27, 45). These 2 studies were re-read carefully. The primary outcome assessment in Colomer et al.’s (27) study was the WMFT and the secondary outcome was measured with the FMA. In addition, the results of their study showed that there was no significant difference in the FMA scores between the 2 groups after intervention. It is possible that such issues might cause heterogeneity among studies.
This meta-analysis has some limitations. First, only those studies that were published in English in electronic databases were included, thus we may not have identified studies written in other languages or unpublished studies. Secondly, although our meta-analysis investigated some relative factors that caused the heterogeneity, the included studies varied in a wide range of aspects, such as study location and area, baseline status, intervention methods and so on, which might confound the results. However, these factors could not be assessed due to lack of reported data. Thirdly, we only included studies for which the outcome assessment was the FMA. Thus, the generalizability of this meta-analysis was suitable only for stroke patients whose motor function was evaluated with the FMA. Therefore, further well-designed studies, with a large sample size, are required in order to explore the effect of MT on motor function in patients with stroke. More outcome measures of motor function should be included in a meta-analysis of the effect of MT.
In conclusion, MT was associated with improved immediate motor functional outcome, assessed with the FMA, in patients with stroke. Further well-designed studies are needed to investigate the effect of MT.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize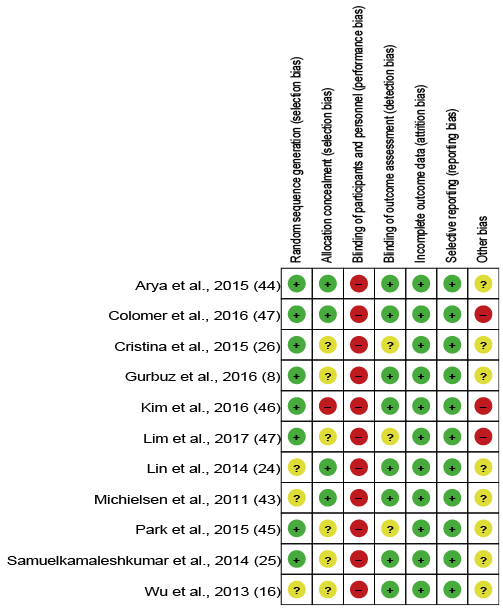 Click to show fullsize
Click to show fullsize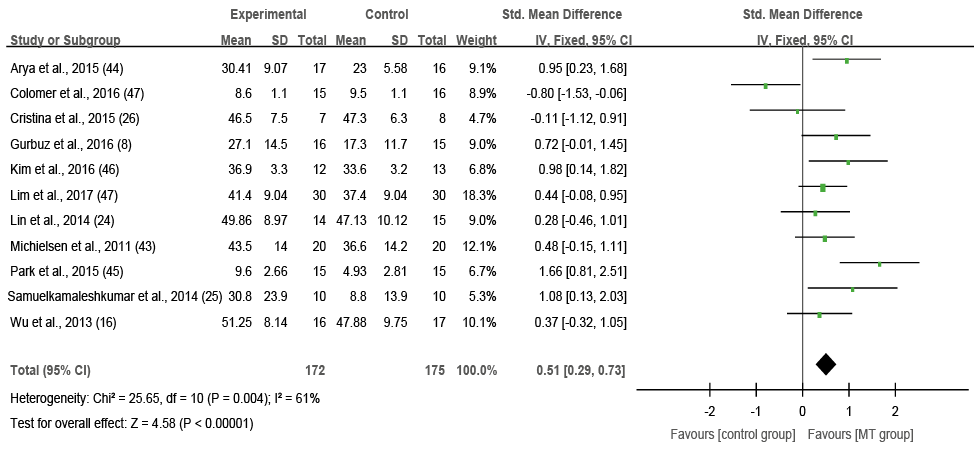 Click to show fullsize
Click to show fullsize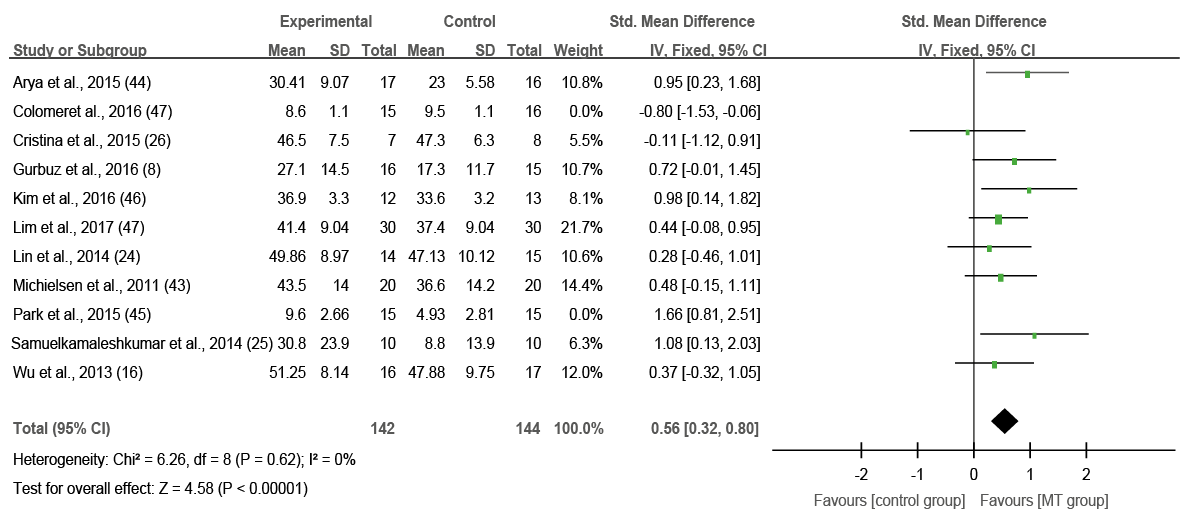 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize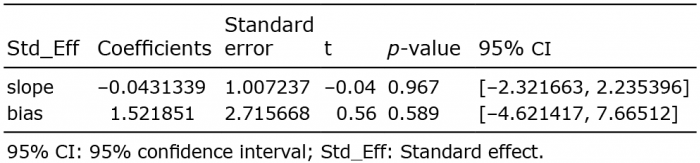 Click to show fullsize
Click to show fullsize