
From the 1Department of Community Medicine and Rehabilitation, Rehabilitation Medicine, Umeå University, Umeå, 2Department of Medical and Health Sciences, Linköping University, Linköping and 3Department of Community Medicine and Rehabilitation, Physiotherapy, Umeå University, Umeå, Sweden
Objective: To explore patient experiences of participating in multimodal pain rehabilitation in primary care.
Subjects: Twelve former patients (7 women and 5 men) in multimodal rehabilitation in primary care were interviewed about their experiences of multimodal rehabilitation.
Methods: The interviews were analysed using qualitative content analysis.
Results: Analysis resulted in 4 categories: (i) from discredited towards obtaining redress; (ii) from uncertainty towards knowledge; (iii) from loneliness towards togetherness; and (iv) “acceptance of pain”: an ongoing process. The results show that having obtained redress, to obtain knowledge about chronic pain, and to experience fellowship with others with the same condition were helpful in the acceptance process. However, there were patients who found it difficult to reconcile themselves with a life with chronic pain after multimodal rehabilitation. To find what was “wrong” and to have a medical diagnosis and cure were important.
Conclusion: Patients in primary care multimodal rehabilitation experience a complex, ongoing process of accepting chronic pain. Four important categories were described. These findings will help others to understand the experience and perspective of patients with chronic pain who engage in multimodal rehabilitation.
Key words: chronic pain; multimodal rehabilitation; primary healthcare.
Accepted Sep 21, 2017; Epub ahead of print Oct 27, 2017
J Rehabil Med 2018; 00: 00–00
Correspondence address: Elisabeth Pietilä Holmner, Department of Community Medicine and Rehabilitation, Rehabilitation Medicine, Umeå University, SE-901 85 Umeå, Sweden. E-mail: elisabeth.pietila.holmner@vll.se
Approximately 20% of the Swedish population has chronic pain of significant intensity, defined as persistent or intermittent pain of at least 3 months’ duration (1–3). Women have a higher prevalence of chronic pain than men (4). Surveys show that 20–40% of primary care visits are the result of pain, and half of these are due to some form of chronic pain (5).
Pain is a complex multifaceted condition, since it is influenced by, and interacts with, different physical, emotional, psychological and social factors. In addition to an individual’s daily function, activity and participation, these problems often result in high economic costs for society. The costs include high utilization of healthcare resources, long-term sick leave, absence from work, and lost productivity (6, 7). A growing body of evidence supports multimodal rehabilitation (MMR), compared with unimodal rehabilitation, for the treatment of patients with chronic pain. MMR has been shown to have long-term and positive effects on return to work and sick leave (1, 3, 8–11).
MMR is based on a bio-psychosocial model that considers somatic, psychological, environmental and personal characteristics. MMR includes a combination of physical and psychological interventions performed by an interdisciplinary team with a common goal, over a lengthy period of time. The patients collaborate actively with the team in goal-setting and reaching the goals (1).
MMR has traditionally been provided in specialty care, but after the introduction of the Swedish rehabilitation warranty in 2008, MMR programmes have also been performed in primary healthcare for patients with less complex chronic pain. There is limited research into how MMR works in primary care (1). In a previous study healthcare professionals perceived MMR to be a helpful treatment for patients with chronic pain (12). In another primary care study, patients attributed the staff with having an important role in understanding individual needs and confidence-inspiring alliances (13). Ekhammar et al (14). studied experiences of change related to MMR and found that, after MMR, patients felt a sense of “increased living space”. Since primary care MMR is a relatively new method, gaps in knowledge remain about patient participation experiences. As studies of primary care MMR are often conducted in local settings, we decided to perform a qualitative study with a broader perspective among participants from 2 county councils and several primary healthcare centres in Sweden. The aim of this study was to explore patient experiences of participating in primary care MMR.
A qualitative method was used, since it is suitable for exploring human experiences (15, 16).
The study was carried out in 2 Swedish county councils; 1 in northern Sweden, the other in southern Sweden. The MMR programme was based on a bio-psychosocial approach, carried out by an interdisciplinary team, and the patient was an active team member. Involved professions were suitable for the bio-psychosocial approach, e.g. physiotherapist, occupational therapist, physician, psychologist. MMR was conducted as a group intervention, or as a combination of a group intervention and individual components. The programmes included, e.g. physical activities, relaxation, training in coping strategies, and education in pain management. Inclusion criteria for MMR were: age 18–65 years, disabling chronic pain, potential for an active life change, and no other disease or other state that precluded participation in the programme. Patients needed to be on sick leave, or experiencing major interference in daily life due to chronic pain and thus at risk of sick leave.
Patients were referred from healthcare professionals at primary healthcare centres. Before participating in MMR, each patient was assessed and selected for MMR by an interdisciplinary team in primary care. According to Swedish guidelines there is a medical indication for MMR if the patient has chronic pain that significantly limits the patient’s daily life, and if the patient has the potential to improve despite the pain (17).
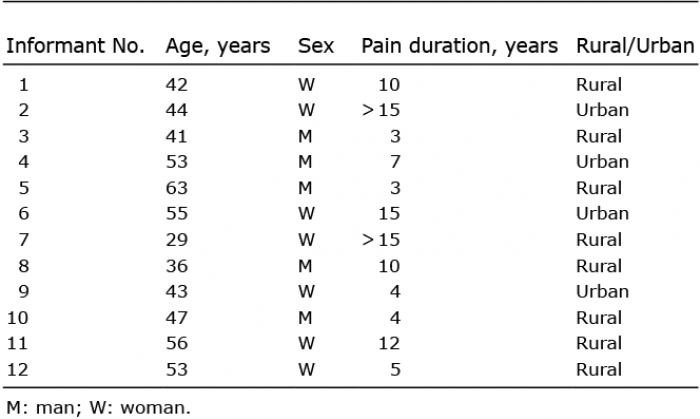
The informants for this study were former participants in primary care MMR programmes. Thirteen informants were invited to participate. One person dropped out due to the acute illness of a close relative. Twelve informants were included (7 women and 5 men). The informants came from rural and urban areas. Some were on part-time sick leave and some were in vocational training. Background data for the informants are shown in Table I.
Table I. Background data for the informants
Rehabilitation coordinators at 12 primary healthcare units in the 2 county councils were contacted and received written information about the study’s purpose and approach. Rehabilitation coordinators were asked to consider former MMR informants who could be interviewed about their experiences of MMR. Seven coordinators responded and informants from these healthcare units were recruited through purposive sampling. This method was used to select informants who share particular characteristics and have the potential to describe rich, relevant and diverse data pertinent to the research question (18). Hence, coordinators were instructed to recruit informants with different perspectives, both positive and negative views on MMR, women and men, and of different ages. If the informants agreed to participate, they were contacted by one of the researchers to plan the practical issues. The informants decided where they wanted to be interviewed: in their home, at a healthcare centre, or at another official location. Each informant provided written informed consent prior to the interview. The interviews took place within 12 months of finishing the MMR programme. The interviews lasted from 27 to 88 min.
An interview guide was prepared by the research group. The interview guide was primarily used to remind the interviewer of which topics to include, and was not adhered to strictly. All interviews began with the open-ended question, “What are your experiences of participating in MMR?” The first author (EPH) and last author (GS) conducted 6 interviews each. Interviews were audiotaped and transcribed verbatim.
The interviews were analysed by qualitative content analysis (15, 16).
The analysis started with reading the interviews several times to gain an overview of the entire text. Next, the coding process began with division of the text into meaning units. Each meaning unit was labelled with a code. The coding process was done with Open Code 4.0 Umeå software (Umeå University; 2013 ICT Services and System Development and Division of Epidemiology and Global Health) (19). The first author (EPH) coded the entire material. Two authors (BMS, GS) each coded 3 interviews for triangulation. The codes were sorted and grouped into subcategories and categories during discussion and negotiation between all authors. Interpretation were made on a manifest content level according to the depth of the interviews. Table II gives an example of the coding process.
This study was approved by the Regional Ethical Review Board in Umeå, Medical Faculty of Umeå University (Dnr 2013-192-31 M).
The analysis resulted in 4 categories: (i) from discredited towards obtaining redress; (ii) from uncertainty towards knowledge; (iii) from loneliness towards togetherness; and (iv) “acceptance of pain”: an ongoing process. The results showed that having obtained redress, to obtain knowledge about chronic pain and experience fellowship with others with the same condition was helpful in the acceptance process. The analyses did not show any patterns regarding age, sex, location or pain duration.
The emergent categories are presented below. Quotations are in italics and exemplify the category in which they are presented (Table II).
Table II. Experience of multimodal rehabilitation in primary care: qualitative analysis categories and subcategories
Informants had previous, lengthy contact with healthcare, and each received a number of different rehabilitation interventions before participating in MMR. They reported divergent expectations of former experiences. Those with positive experiences were optimistic, hopeful, and wished to obtain treatment other than medication. Some described a desire to prevent sick leave by engaging in MMR. Those who had negative experiences described doubts, a fear of not being listened to, and that the healthcare service would not see them as whole human beings.
I feel that it is difficult…. that you will not be trusted when you come here (healthcare in general) and say something. The doctors do not really believe it. And because I have been on strong medications, they think I’m looking for drugs more than any other (treatment). (Informant 10)
Informants sometimes felt that their pain problems were simplified, and that they were not allowed to have pain. Medical staff, social insurance, and closely related parties (relatives, friends, and co-workers) sometimes believed that their pain could be fixed. Their suggestions for action were described as frustrating.
Everyone says that it should be fine. Yes, everyone has a solution….do this, you know, try this. Eat rosehip powder…. (Informant 3)
Such simplifications and to be discredited were compared with the relief they felt when MMR professionals verified what the patients already knew: that the pain cannot be fixed.
…. All the previous treatments dealt with taking away the pain. This is the first time one gets a treatment that focuses on acceptance of the pain, and you really understand that this is chronic pain that will never disappear; it’s the first time one has received the message from this angle.” (Informant 3)
For most informants, participation in MMR meant that they had obtained redress. That is, they felt they were validated, believed, and taken seriously. During MMR, they had had the opportunity to talk about their pain condition, to obtain knowledge about chronic pain, and to be medically assessed.
Informants felt that, during MMR, they were treated by rehabilitation teams who acted in professional ways that helped them reach an understanding. Through their way of asking questions, the team encouraged the informants to reflect on their own thoughts and behaviours. They felt that this stimulated them to initiate behavioural changes
For some informants, uncertainty about the cause of the pain led to worries about the future. Worries could be, for example, about their future finances and ability to work. These informants expressed feelings of worthlessness related to having chronic pain, e.g. feelings of not being good enough at home or work. Having to ask for help, or needing the spouse to do things that they had previously done were other examples that led to feelings of worthlessness.
Informants described how participation in MMR increased their knowledge of chronic pain and the consequences of living with chronic pain. This resulted in reduced fear and anxiety, and an increased sense of being able to manage in spite of their pain. Understanding that pain was not “in your mind” was also described as valuable. The ability to manage their pain was expressed as a benefit for dealing with practical issues in future everyday life.
…. In the past, I have encountered a lot of strange things. And you wonder, “what the heck is so wrong?” But now you have been given an explanation for it. So, you don’t get as frightened (as before). (Informant 8)
MMR also led to insights about the complexity of chronic pain, e.g. what might influence how the informants perceived their pain, what might have contributed to the development of chronic pain.
…. There is a lot you carry with you. I have learned that now. All that has happened in life until now, I sort of carry with me, and it influences me physically. Although, it is in here, or the pain…it comes from the inside obviously, (and) I had not thought about that before. But then you think, well, maybe, maybe I carry a lot of baggage in some ways. (Informant 1)
Informants described how they became aware of their negative thinking, and MMR participation taught them that it was important to change their ways of thinking. They found new ways to look at their chronic pain, with a new understanding of important factors for the onset of pain, and knowledge that pain persisted despite the fact that an injury was healed. Examples of these insights were learning that previous stressful events affected their psychological mood, and how participating in MMR had resulted in more positive thinking.
Other insights were that pain medication was not sustainable in the long term, and that other treatments were needed. Informants expressed a need for other tools that they could link to their pain, such as new ways of thinking and acting.
Some informants set individualized goals for their rehabilitation in MMR. This helped them better understand how pain influenced their lives, and how they should focus on what was important to them. They realized that it could take a long time to achieve their goals.
This category describes the informant experiences of being in a MMR group with other people.
The realization of not being alone while living with pain, and sharing experiences with others who had similar pain problems was positive.
To meet people who suffered from more pain than me, led to an awakening, and gave distance to my own problem. .... in other words, I am still fortunate. You know there are those who experience tremendous pain day and night every day. So, it is also very useful to see that yes, but I am actually quite lucky. (Informant 11)
Most informants reported positive experiences of fellowship with other participants in the MMR programme. Meetings with individuals who had similar problems, who listened and understood how it is to live with chronic pain, gave a sense of safety and togetherness.
.… it feels a little good that there are, sort of, those who have what I have (same problem) …. the others (participants in the group) understood what I meant…. (Informant 1)
However, there were also negative expectations and experiences of participating in group sessions. This was explained as fear that their pain might be reinforced if they listened to other people’s pain descriptions. Someone even felt provoked when participating in group sessions where negative experiences were discussed.
…. Should one keep on talking about one’s pain?.... I felt it became…. or I was afraid that it would become, some sort of self-fulfilling prophecy. (Informant 9)
Some informants did not think they had anything to learn from the group sessions, and that they already knew all about rehabilitation. Some even thought that they had more to give to the group than they would get out of participation.
…. But I have learned so much myself in my journey (earlier rehabilitation), that I thought I had done all of that several times. So therefore, I did not think it gave me so much, but…I already knew … what you have to do and not (do)…. (Informant 4)
The analysis showed that the task of accepting pain was an ongoing process and that having obtained redress, learning about chronic pain, being with others who had chronic pain, and sharing the same condition were helpful in the acceptance process.
After participating in the MMR programme, the informants used terms such as “to accept” or “had started to learn one must accept pain”. Some informants found it difficult to reconcile themselves to live with chronic pain, and they did “not accept” the pain.
“To accept” pain was described as not allowing pain to take control over their life, and as how they adjusted to the current pain. They explained that it could take a long time to understand and totally accept that their pain would remain.
…. It (pain) doesn’t get improved by fighting against it, it is there and will always be there. Sure, pain pills and pain relief and so on, that works now and then, and sometimes I’m really bad so I need them…. (Informant 3)
Other informants explained that MMR was the start of accepting their pain, and one must accept that one cannot do what one did before.
…Somehow you have to accept that you have the pain you have, and some things you can’t do because then you get a backlash if you do. And it (MMR) has, well, somehow, it has helped a little bit to realize that you can’t do everything you want. (Informant 8)
Some informants said MMR helped them become aware of how pain limited their lives and affected participation in work and leisure. After MMR, they changed their way of thinking and acting to achieve more balance in everyday life, and they reduced demands on themselves. Some said that they learned how to balance everyday life activities, although they often forgot and had to be reminded to do so. The importance of setting limits, both for themselves and towards others, was described. This could include saying no to participation in social events, or setting limits with their children. Limits could also be set through involving others by asking for help, or that these changes were not associated with feeling guilt. When informants talked about how they established their changing strategies, they mentioned ways to reduce workloads, develop relaxation habits, and increase their daily physical activities. Some decided to reduce their work hours.
…It’s OK not to work 8 hours a day. I don’t need to make so much money now that we have sold the apartment…. I’m starting to think differently. (Informant 3)
But among those who said they did not accept their pain, the goal of becoming pain-free was most important. They wanted to be cured, and found it difficult to reconcile themselves to a life with chronic pain. There were those who still did not feel they had received complete medical investigation, and they waited for specialist assessments after MMR. To find what was “wrong” and to get a medical diagnosis and a cure were important. They expected that a physician with speciality competency should decide about further investigations and treatments, and these were essential for whether or not they could assimilate what they learned in MMR.
….I need an evaluation (medical).... It is the hospital that must make the evaluation, if I should have surgery or not. (Informant 10)
The acceptance or non-acceptance of living with chronic pain can thus be expressed as an ongoing process. The analyses showed that acceptance is not a static condition. Some informants could describe themselves as accepting the pain in one moment, but in next, they talked about searching for a cure.
This study focused on patient experiences of participating in MMR in primary care. It showed that most informants felt believed by the health professionals, and that they had obtained redress. The MMR programme contributed to informants’ increased knowledge and understanding of chronic pain and its complexity. Shared experiences in group meetings had led to fellowship and less feelings of loneliness for certain informants. Acceptance of living with chronic pain was not a straightforward process. After the rehabilitation programme, some informants were still searching for a treatment in order to be free from pain.
The category “From discredited towards obtaining redress” includes distrusting the concepts about living with chronic pain that are similar to previous research. Experiences such as not being listened to, not believed, and not seen as a whole human being are reported (20, 21). The importance of receiving a diagnosis was reported in our study and has been found in previous research (22, 23).There is a view among patients with chronic pain that a diagnosis of pain symptoms serves as evidence to legitimize their pain (23). LaChapelle et al. argue that having a diagnosis is key in the process of accepting pain, and the starting point of self-management strategies (22). Their study showed that the type of diagnosis obtained played a role. Those who were diagnosed with fibromyalgia felt that they needed to search for information on their own, and that health professionals did not know much about their diagnosis (compared with patients diagnosed with arthritis) (22). Although most of our informants had a benign, chronic musculoskeletal pain diagnosis, they found consolation in having a confirmatory diagnosis and obtaining knowledge. The informants’ earlier experiences of lack of support both in healthcare and private were frustrating. LaChapelle et al. (22) identify lack of support and acceptance from others, e.g. healthcare professionals, family, and friends, as a barrier to acceptance of pain.
The informants in our study were also given differing solutions in healthcare. A previous study found that MMR team personnel expressed fear of not adequately investigating the patient and they were afraid they might have missed a serious medical condition (12). This attitude increases the chance that a patient is referred for a wide variety of assessments and will get different solutions suggested for solving the pain. The national guidelines for chronic pain rehabilitation recommend that, before a decision is made about MMR, a patient should be adequately investigated, and not moved into other assessments (17).
According to our informants, an important part of MMR was the professional team work that contributed to informants feeling that they had obtained redress. In another study of MMR in primary care, collaboration between patient and personnel was found to be fundamental to rehabilitation (13). In our study, getting an explanation about chronic pain and its related consequences led to less uncertainty. These results are consistent with previous research about the importance of pain education (24, 25). Knowledge was also important, although it led to less fear and anxiety related to pain. Previous studies have similar conclusions (25–27).
The informant’s social context, e.g. related experiences of the impact of their role in the family relations or with healthcare professionals, is important in addition to taking part in rehabilitation in primary care. To live with chronic pain and be in different social contexts was associated with various experiences. This was explained as not being able to perform the same duties as before, or having to ask for help. Living with chronic pain meant a change in perception of themselves, and was a challenge, for example, in relation to their family life. Kostova et al. (28) identified the family as the most important social support, emotionally and practically, in supporting independence of the individual to manage different life roles and motivate the individual to not be a passive victim. The family has an important role in balancing between support and providing individual space and independence. The programmes that our informants participated in included limited participation of relatives. Since this seems to be important for the acceptance process, family involvement in rehabilitation might help them make progress.
Most informants in our study reported benefiting from being in the MMR group. There were some who preferred to receive individual rehabilitation. When a patient is considered for MMR, it is important to assess whether rehabilitation should be done individually or as MMR in a group (17). Professional experiences of working with MMR showed that it sometimes was difficult to get enough participants in a group. They wondered why all patients who seek care for chronic pain were not referred to MMR (12). This might be because MMR was a new intervention in primary care.
There are different facets of accepting or not accepting life with chronic pain. We explored the acceptance process as an ongoing dynamic process. This was shown in another study in which patients were divided into different steps of acceptance, e.g. receiving a diagnosis, realizing there is no cure, and realizing it could be worse (22).
Our informants commonly used the word “acceptance”. At some of the healthcare centres, acceptance and commitment therapy (ACT) (29) was included in MMR, and the personnel were trained in this method.Since including ACT in MMR is relatively new, there is a risk that the method is not sufficiently known among all personnel in the programs to implement it. Thompson et al. warn that the term “acceptance” can be misunderstood, both generally and in relation to chronic pain, and that healthcare professionals may oversimplify what acceptance means (30).
How a group of women understood the word “acceptance” was examined (22). Most participants in that study explained the term as meaning “giving up” or “giving in” to their pain. This is so even though they also explained situations corresponding to components proposed as marks of accepting pain defined in another study (31).
The overall purpose of the present study was to explore patient experiences of participating in multimodal pain rehabilitation in primary care. Since this is a group of patients with long experience in healthcare and rehabilitation before participating in MMR, they had a great need to talk about their previous experiences. At times, this was a limitation during the interviews, since some informants needed to talk about the past rather than focusing on MMR experiences. Nevertheless, this also provided valuable background knowledge for the current analysis. This study has several strengths. It was conducted in 2 county councils, which included urban and rural areas; 1 in southern Sweden and 1 in northern Sweden. This provided a range of different settings. Rehabilitation was conducted at small primary care clinics and primary healthcare centres. The strategic sample with variations in ages and sex is a strength.
The research group consisted of men and women with different professions, and included clinicians and academics, working in primary and specialist care. This was a strength during the study analyses. This approach may strengthen the credibility of the results, through the opportunity to supplement and challenge one another’s views.
One shortcoming of this study was that the informants were not given the opportunity to reflect on the findings. Another shortcoming may be that the interviews were conducted up to 1 year after MMR, and it may have been difficult for informants to remember their expectations before rehabilitation. On the other hand, MMR deals with lifestyle changes that are long-term processes. In order to obtain sufficient perspective, some distance is important.
MMR within primary care has a short history, and research in the field is limited. This study focused on patient experiences and adds information through patient voices. This will contribute to further development of MMR implementation for pain rehabilitation in primary care.
In conclusion, this study provides new insights through patient voices. Acceptance of living with chronic pain is an ongoing process, and is not static.
Patients who participated in primary care MMR felt that the rehabilitation was valuable. Knowledge about pain and its consequences, fellowship with others with chronic pain, being believed, and obtaining redress were important components of the accepting process. However, there are those who found it difficult to reconcile themselves to a life with chronic pain, even after MMR. To find out what was “wrong” and get a medical diagnosis and cure were important.
This study was supported by grants from Västerbotten County Council.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize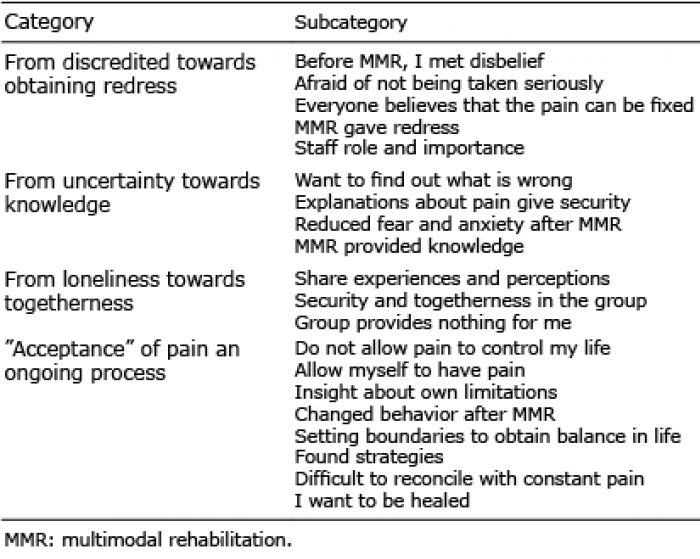 Click to show fullsize
Click to show fullsize