
From the Department of Exercise and Nutritional Studies, San Diego State University, College of Health and Human Services, San Diego, CA, USA
Objective: To investigate the effects of overground bionic ambulation with variable assistance on cardiorespiratory and metabolic responses in persons with motor-incomplete spinal cord injury.
Design: Case series.
Subjects: Four participants with chronic, motor-incomplete spinal cord injury.
Methods: Subjects completed a maximal graded exercise test on an arm-ergometer and 3 6-min bouts of overground bionic ambulation using different modes of assistance, i.e. Maximal, Adaptive, Fixed. Cardiorespiratory (oxygen consumption) and metabolic (caloric expenditure and substrate utilization) measures were taken using a mobile metabolic cart at each overground bionic ambulation assistance.
Results: Cardiorespiratory responses ranged from low (24% VO2peak) for the least impaired and fittest individual to supramaximal (124% VO2peak) for the participant with the largest impairments and the lowest level of fitness. Different overground bionic ambulation assistive modes elicited small (3–8% VO2peak) differences in cardiorespiratory responses for 3 participants. One participant had a large (28% VO2peak) difference in cardiorespiratory responses to different modes of overground bionic ambulation. Metabolic responses mostly tracked closely with cardiorespiratory responses. Total energy expenditure ranged from 1.39 to 7.17 kcal/min. Fat oxidation ranged from 0.00 to 0.17 g/min across participants and different overground bionic ambulation modes.
Conclusion: Overground bionic ambulation with variable assistance can substantially increase cardiorespiratory and metabolic responses; however, these responses vary widely across participants and overground bionic ambulation modes.
Key words: walking; cardiovascular; exoskeleton; spinal cord injury.
Accepted Aug 28, 2017; Epub ahead of print Oct 25, 2017
J Rehabil Med 2018; 1: 00–00
Correspondence address: Jochen Kressler, 5500 Campanile Drv, San Diego, CA 92182, USA. E-mail: jkressler@mail.sdsu.edu
Walking is the most common form of human locomotion. Spinal cord injuries (SCI) causing lower limb paralysis limit a persons’ ability to walk, often resulting in the use of a wheelchair for general means of transportation. In able-bodied adults, walking stimulates the cardiorespiratory system to increase metabolic responses that are notably higher than resting rates. Walking, performed at a sufficiently high intensity and duration, is seen as an attainable way to increase energy expenditure and decrease risk of metabolic and cardiorespiratory-related disease (1).
SCI often causes secondary health problems associated with immobility. These may include impaired metabolic function, decreased cardiorespiratory fitness, increased adiposity/obesity, and accelerated physical deconditioning (1). Recently, a class of lower limb bionic suits (exoskeletons) has been developed that enable overground walking in persons with SCI. These suits give rise to additional therapy options that may lessen secondary complications from reduced physical activity.
Preliminary evidence has shown several potential health benefits from overground bionic ambulation (OBA) training in which maximal (complete) assistance is provided during walking (1, 2). In studies in which participants had motor complete SCI, OBA with maximal assistance showed increases in VO2/Mets/heart rate (HR) outputs (1, 3). During OBA with maximal assistance, the exoskeleton continually provides all of the power necessary to facilitate the participant’s stepping motion during the swing phase of gait. Newer versions of these devices can provide variable levels of assistance. This enables the participant to use any residual motor function they may have instead of moving the limbs passively through the walking trajectory. Little is known about the effects of variable assistance during OBA on cardiorespiratory and metabolic responses for people with motor-incomplete SCI.
The aim of this descriptive study is to understand how OBA with variable assistance affects energy expenditure during walking in persons with motor-incomplete SCI. In particular, the cardiorespiratory and metabolic responses to exoskeleton-supported walking with different levels of assistance were investigated in people with motor-incomplete SCI.
The bionic exoskeleton used in this study was the Ekso GT (Ekso Bionics, Richmond, CA, USA). Detailed descriptions of the device (Ekso) have been published elsewhere (4, 5). In brief, the device is a lower extremity robotic exoskeleton with 2 legs connected to a torso structure. The device has 4 motors that actuate the hip and knee joints in the sagittal plane.
Each participant is assigned a swing phase trajectory that they are asked to follow while walking in the Ekso. The swing phase trajectory is based on parameters chosen by the experimenter (a physical therapist). These parameters include step height, step length, and swing time. Based on these parameters, the robot has an expectation of the position of the leg at each time point of the swing phase. If the user does not follow the assigned trajectory and/or does not reach a position at the expected time, then the robot provides assistance to keep the user on track. The final parameters used during testing were chosen through an iterative process, based on user feedback, observation of the gait pattern by the physical therapist, and minimizing the assistance from the motors.
Participants completed all overground walking tests in different assistive modes of the Ekso: Maximal, Fixed, or Adaptive. Maximal assist mode gives the most tightly constrained powered robotic assistance, where the participant does not have to contribute any muscle power to complete steps.
During Adaptive mode the robot provides variable (0–100%) power of the motors to either or both of the legs during swing phase. Adaptive mode reacts to how well the participant is able to complete the assigned trajectory and provides the remaining amount of assistive power needed to complete each step within the prescribed trajectory.
In Fixed mode the maximum amount of robotic assistance is manually set at a fixed level by the experimenter. If the participant needs less than the set assistance level to complete a step, the motors will adapt and only provide as much assistance as needed. If the participant needs more robotic assistance than is assigned in Fixed mode, the movement during swing will stop and the participant will be given a set amount of time (200% of swing time) to correct their trajectory on their own. If they are unable to do so in that time period, the robot provides full assistance to complete the step. The level for Fixed mode was set to minimize the assistance as much as possible while minimizing such movement interruptions.
Inclusion and exclusion criteria were based on those given by the manufacturer of the bionic exoskeleton. Inclusion criteria were: history of SCI, weight under 100 kg, height between 152 and 188 cm, normal or near-normal lower extremity range of motion, enough upper extremity strength to manage transfers and/or assistive devices, medically stable and candidate for full weight-bearing gait training (users should have previously been practicing standing), able to follow commands, able to express discomfort and pain. Exclusion criteria were: spinal instability (or spinal orthotics unless cleared by a medical doctor), unresolved deep vein thrombosis, decreased standing tolerance due to orthostatic hypotension, significant osteoporosis that prevented safe standing or may have increased the risk of fracture caused by standing or walking, uncontrolled spasticity, uncontrolled autonomic dysreflexia, skin integrity issues on the buttocks or on surfaces that were in contact with the Ekso, upper leg length discrepancy greater than 1.3 cm or lower leg discrepancy greater than 1.9 cm, significantly impaired balance, cognitive impairments resulting in motor planning or impulsivity concerns, pregnancy or colostomy.
The study was approved by the institutional review board of the university. Written informed consent was obtained from all participants. Four participants were recruited from a sample of participants in a pilot rehabilitation programme (Table I).
Table I. Subject demographics
Subject 1 was a woman, age 43 years, with SCI at T12 that had occurred 9 years prior to testing. She weighed 57 kg, was 155 cm tall and identified as Latina. She was non-ambulatory, with a manual wheelchair as her primary means of mobility, and was independent with transfers using a sliding board. Manual muscle test scores of her lower extremities (hip flexion, hip extension, hip abduction, knee extension, ankle dorsiflexion and ankle plantarflexion) ranged from 0 to 1 on the left side and 0 throughout on the right side (Table II). For Subject 1, the swing phase trajectory parameters were set to: step length = 38.1 cm, step height = 0.3 cm and swing time = 1.0 s. She used forearm crutches during OBA. She was experienced in OBA, having trained at least 1×/month for 27 months for a total of 85 training sessions before the assessments. For the last 10 sessions, the minimum OBA time was 20:29 min (783 steps) and the maximum was 44:24 min:s (1,729 steps).
Table II. Manual muscle test scores for the lower extremities (L/R)
Subject 2 was a woman, age 48 years, with SCI at T12 that had occurred 9 years prior to testing. She weighed 70 kg, was 156 cm tall and identified as White. She walked independently with a rolling walker for short distances, but used a manual wheelchair in the community. Her walking speed with the rolling walker was 0.23 m/s, and her Berg Balance Scale (BBS) score was 29/56 (6). Manual muscle test scores in the lower extremities ranged from 3 to 5 on the left side and 3 to 5 on the right side (Table II). Ekso swing phase trajectory parameters for this subject were set to step length = 38.1 cm, step height = 0.5 cm and swing time = 1.3 s. She used a rolling walker during OBA. She was experienced in OBA, having trained at 1–2 × /week for 3 months for a total of 25 training sessions before the assessments. For the last 10 sessions, the minimum OBA time was 9:28 min:s (330 steps) and the maximum was 22:22 min:s (713 steps).
Subject 3 was a man, age 42 years, with SCI at T6 that had occurred 2 years prior to testing. He weighed 84.5 kg, was 173 cm tall and identified as Latino. He walked independently with a rolling walker for short distances, but used a manual wheelchair in the community. His walking speed with the rolling walker was 0.33 m/s, and his BBS score was 31/56 (medium fall risk). Manual muscle test scores in the lower extremities ranged from 0 to 2 on the left side and 2 to 5 on the right side (Table II). Ekso swing phase trajectory parameters for this subject were set to: step length = 40.6 cm, step height = 0.3 cm and swing time = 0.8 s. He used a rolling walker during OBA. He was experienced in OBA, having trained 1–2 times per week for 3 months for a total of 24 training sessions before the assessments. For the last 10 sessions, the minimum OBA time was 18:14 min:s (754 steps) and the maximum was 52:22 min:s (2,472 steps).
Subject 4 was a woman, age 24 years, with SCI at C5 that had occurred 2 years prior to testing. She weighed 45.5 kg, was 160 cm tall and identified as Latina. She was a power wheelchair user, and walked with a rolling walker for exercise only. She required minimal to moderate assistance with sliding board transfers. Manual muscle test scores in the lower extremities ranged from 0 to 2 on the left side and 2 to 5 on the right side (Table II). Ekso swing phase trajectory parameters for this subject were set to: step length = 38.1 cm, step height = 0.3 cm and swing time = 1.1 s. She used a walker as assistive device during OBA. She was experienced in OBA, having trained at least 1–2 times per week for 3 months for a total of 26 training sessions before the assessments. For the last 10 sessions, the minimum OBA time was 19:03 min:s (695 steps) and the maximum was 51:38 min:s (1,897 steps).
Peak graded exercise test. Participants completed a peak graded exercise test to volitional exhaustion on an arm cycle ergometer (Rehab Trainer 881E, MONARK, Vansbro, Sweden) on a non-exoskeleton walking day. The Graded Exercise Testing (GXT) started at an initial workload of 0 Watts for 3 min. Resistance was increased by 10–15 W every 3 min for females and 15–20 W every 3 min for males. VO2 peak was calculated as the maximal value for the mean of a 15-breath running, as described by Robergs et al. in 2010 (7). Cardiorespiratory values were collected from a mobile metabolic cart fitted with an integrated heart rate monitor with a rubber mask (Oxycon Mobile, CareFusion, Yorba Linda, CA and Polar Electro Inc., Lake Success, NY, USA).
6-minute overground bionic ambulation bouts. Data collection for oxygen consumption began with 3 min of seated resting values. The participants then stood for 3 min while data was collected. Participants were offered 2–5 min of easy walking as a warm-up, with a 3-min rest to follow. Participants completed consecutive bouts of 3 modes of assisted walking, with 5-min rest periods in between each bout or until CR values return to resting levels. Maximal mode was always completed first, followed by Fixed mode or Adaptive mode in randomized order. During Maximal mode, participants were instructed to walk with the machine as smoothly and efficiently as possible. During Fixed or Adaptive modes, participants were instructed to contribute the maximal voluntary effort to maintain the prescribed walking trajectory. At the end of each stage, heart rate, blood pressure and rate of perceived exhaustion were collected. Participants completed all OBA bouts over flat hardwood flooring on a 30 × 15 m rectangular-shaped course. After trials with variable assistance, the mean robotic assistance for the last 30 steps per leg was recorded.
VO2 and VCO2 (cardiorespiratory) measurements were used to calculate the fat and carbohydrate (CHO) (metabolic) utilized during exercise, using stoichiometric formulas based on exercise intensity with assumptions of negligible protein oxidation contribution, as described previously (8):
The total energy (kcal) utilized during exercise was calculated by multiplying total g of fat or carbohydrates by 9.75 kcal for fat, 3.95 kcal for CHO (< 50% VO2peak) or 4.07 kcal for CHO (> 50% VO2peak). If the R-value (VCO2/VO2) was greater than 1, fat oxidation rate was set at 0. Total energy expenditure (TEE) was estimated by adding fat and carbohydrate kcal oxidations.
Mean arterial pressure (MAP) was calculated as DBP + 1/3(SBP–DBP).
Rated Perceived Exertion (RPE) were measured on a 0 (no effort) – 10 (maximal effort) scale, as originally described by Borg (9).
Rate pressure product (RPP) was calculated as HR × SBP.
Distance walked was estimated from the number of steps recorded by the exoskeleton multiplied by the step-length setting.
Individual descriptive statistics were used to describe the outcomes of the measures.
Subject 1 reached a VO2peak of 12.4 ml/kg/m. Levels of robotic assistance provided are presented in Table III. Fixed mode elicited the highest VO2 (43% VO2peak, Fig. 1), economy (0.49 ml/kg/m, Fig. 2), HR (70% HRpeak, Fig. 3) and RPE (6). BP response was highest during the Maximal mode with MAP = 90 mmHg, resulting in a RPP = 17,000 (Fig. 4).
Table III. Exoskeletal assistance levels during all overground bionic ambulation (OBA) modes averaged over the last 30 steps per leg of each trial
Fig. 1. Oxygen uptake (VO2) response to rests and different overground bionic ambulation modes in absolute (A) and relative (B) terms.
Fig. 2. Overground bionic ambulation (OBA) speed (A) and economy (B) for each mode.
Fig. 3. Heart rate (HR) response to rests and different overground bionic ambulation (OBA) modes in (A) absolute and (B) relative terms.
Fig. 4. Cardiovascular stress responses to rests and different overground bionic ambulation (OBA) modes, as indicated by (A) mean arterial pressure (MAP) and (B) rate pressure product (RPP).
Subject 2 reached a VO2peak of 20.9 ml/kg/m. Fixed mode elicited the highest VO2 (93% VO2peak), economy (0.13 ml/kg/m), HR (94 % HRpeak) and RPE (10), as well as MAP (117 mmHg) and RPP (23,000).
Subject 3 reached a VO2peak of 25.3 ml/kg/m. Fixed mode elicited the highest VO2 (32% VO2peak), economy (0.57 ml/kg/m), HR (67% HRpeak), and RPE (3). MAP was highest during the Adaptive and Fixed modes at 91 mmHg, resulting in a RPP of 16,000.
Subject 4 reached a VO2peak of 7.7 ml/kg/m. Maximal mode elicited the highest VO2 (124% VO2peak), economy (0.46 ml/kg/m), HR (93% HRpeak), but not BP, which was highest for Fixed mode (6). We were unable to collect BP from this subject during OBA.
Subject 1 utilized the most calories during the Fixed setting, at a TEE rate of 1.72 kcal/min. Substrate partitioning was heavily reliant on CHO (0.43 g/min) and negligible fat contribution (< 0.1 g/min, Fig. 5).
Fig. 5. Participant total energy expenditure (TEE) rate (A) in response to rests and different overground bionic ambulation (OBA) modes and (B) estimated for a 1-h steady-state exercise bout.
Subject 2 utilized the most calories during the Fixed setting, at a TEE rate of 7.17 kcal/min. Substrate partitioning was heavily reliant on CHO (1.76 g/min) and negligible fat contribution (< 0.1 g/min, Fig. 5).
Subject 3 utilized the most calories during the Fixed setting, at a TEE rate of 3.29 kcal/min. Substrate partitioning was equally distributed between CHO (0.42 g/min (51% of TEE)) and fat (0.17 g/min, Fig. 5).
Subject 4 utilized the most calories during the Maximal setting, at a TEE rate of 1.58 kcal/min. Substrate partitioning was divergent with less reliance on CHO (0.16 g/min, 40% of TEE) and more on fat (0.10 g/min, Fig. 5 and Fig. 6).
Fig. 6. Total substrate utilization rate and substrate partitioning of total energy expenditure (TEE) during rests and different overground bionic ambulation (OBA) modes for each subject. CHO: carbohydrate.
The responses to each OBA mode varied substantially, with no clear tendency across subjects. Subject 1 showed responses in line with light-to-moderate physical activity for all OBA modes (10). Slightly higher respiratory, cardiac and metabolic responses (5–15%) were observed for Fixed compared with the other 2 modes. This corresponded to lower levels of assistance provided by the robot in Fixed compared with Adaptive mode (no feedback data available during Maximal mode). This indicates that, for Subject 1, limiting assistance to the lowest amount possible could stimulate larger physiological responses and therefore potentially optimize training effects. Despite these higher responses in Fixed mode, substantially higher RPP during Maximal mode and higher fat oxidation during Adaptive mode OBA were observed for Subject 1. The higher RPP resulted from a substantially higher systolic blood pressure with walking, and indicates higher cardiac stress than for the other modes, albeit still well within normative submaximal ranges (11). Higher levels of fat oxidation during Adaptive assistance probably result from lower exercise intensity, which is indicated by lower VO2 and HR responses during this mode of OBA in Subject 1. Lower intensities are associated with higher proportions of fat oxidation (12). Low levels of fat oxidation are associated with increased obesity and disease and are a particularly pertinent issue for people with SCI (13–18). Targeting maximal levels of fat oxidation is therefore a potential target for health-focused exercise interventions, and for Subject 1 this would be achieved in Adaptive mode.
All OBA modes for Subject 1 were substantially below ventilatory threshold (i.e. 6.6 ml/kg/min, 53% of VO2peak). Coupled with light-to-moderate RPE this would indicate that the subject should be able to sustain OBA in all 3 modes for prolonged periods (i.e. a standard therapy session). Depending on the therapy goal, different OBA modes would be advisable for Subject 1. To maximize physiological adaptations and caloric expenditure and potentially resulting health benefits, Fixed mode would be recommended. The estimated energy expenditure during OBA in Fixed mode would be ~100 kcal/h, which is similar to 1 mile of walking for an able-bodied individual (19). On the other hand, the higher step counts, speed and lower values for OBA economy were observed for Maximal and Adaptive mode. These modes may therefore be more suitable for training sessions in which higher repetition is favoured, or when the participant is experiencing fatigue.
Subject 2 showed increasing respiratory and metabolic responses from Maximal to Adaptive to Fixed modes, corresponding to lower levels of assistance across these modes. While Maximal mode also resulted in the lowest CR responses, there were virtually no differences in Adaptive and Fixed mode in HR or BP. Subject 2’s exercise intensities during OBA reached vigorous (for Maximal and Adaptive modes) to near maximal levels (for Fixed mode) (10). Both Adaptive and Fixed mode intensities were well above ventilatory threshold (i.e. 15.7 ml/kg/min, 75% of VO2peak), indicating that Subject 2 would not be able to maintain these OBA modes for prolonged sessions. This might also explain why mean HR and BP values were similar, as both Fixed and Adaptive mode may have maximally stressed the cardiovascular system. Maximal mode OBA, however, was below ventilator threshold, yet still resulted in substantial energy expenditure (~260 kcal for an hour) and the highest level of fat oxidation. Maximal mode could then potentially be used as a training mode to enhance cardiorespiratory capacity and subsequent transition to Adaptive and Fixed modes. In addition, due to the large differences in exercise intensity, the possibility to intersperse Maximal mode OBA with higher intensity intervals of Adaptive or Fixed mode OBA present an opportunity to maximize physiological adaptations and health benefits for Subject 2, as interval training has been shown to elicit larger responses compared with isocaloric steady state exercise (20).
Subject 3 had the highest respiratory, cardiac and metabolic responses during Fixed mode OBA, followed by Maximal mode and Adaptive mode. Only MAP was almost identical across modes. This was probably due to the fact that the exercise intensity was only very light to moderate (10) for Subject 3 during all modes. It is, however, unclear why Maximal mode elicited 4–17% larger responses than Adaptive mode OBA. Given Subject’s 3 proficiency with OBA and relatively high level of functional capacity he did not have as much experience in Maximal mode as in the other 2 modes. We have previously reported on higher responses for people unfamiliar with OBA (21). As mentioned, exercise intensity was only very light to moderate during all modes of OBA which fell well below the ventilatory threshold (17.3 ml/kg/min, 68% of VO2peak) and barely stressed Subject 3, as indicated by low RPE scores (≤ 3). He would be expected to easily complete prolonged OBA session with the potential to burn 150–200 kcal/h, 40–50% of which would come from fat. However, the OBA elicited respiratory/metabolic response is probably too low (24–32% of VO2peak) to be considered sufficient stimulus to produce respective fitness gains (21).
Subject 4 differed most substantially from the other subjects, in that Maximal mode OBA elicited higher (4–20%) oxygen consumption, TEE and fat oxidation compared with the other 2 modes. This was in spite of the expected lower assistance levels at Adaptive and Fixed modes. Of note, oxygen consumption exceeded maximal values achieved during the GXT test for all OBA modes. Subject 4 had the highest level of injury with impairments of both triceps muscles, resulting in low VO2peak values compared with women with similar SCI and training status (22). She was also prone to spastic contractions in response to OBA (noted by subject report and observations from the experimenters). It is possible that Maximal mode elicited the most spasticity resulting in excessive contraction of the large leg musculature and subsequently increased metabolic demand. The notion that involuntary (spastic) contractions accounted for the large responses during Maximal mode OBA is further supported by the very low RPE, which indicates that Subject 4 contributed no voluntary effort. HR rate responses were also higher during Maximal mode OBA compared with Fixed and Adaptive, and were highest during standing rest. Given the high level of injury, injury severity and low muscle tone, substantial blood pooling in the lower extremities and subsequently diminished venous return are the likely factors underlying these responses. Contrary to what would be expected from the very high relative intensity of exercise, Subject 4 showed high proportions of fat oxidation for all modes of OBA (12, 23). Given that RPE never exceeded moderate levels it is likely that the arm ergometer GXT was simply not a suitable reference test for OBA in this Subject. OBA presents several advantages over upper arm ergometry training (e.g. it is weight-bearing, upright, challenges balance, etc.), and for Subject 4 larger cardiorespiratory responses are an additional benefit of OBA.
Participants did not undergo a full 45 min to 1 h OBA session for each bout, as would probably be done in clinical practice. However, the 6-min OBA walks were of sufficient length to reach steady state and allowed all measurements to be taken within the same session, therefore enhancing reliability compared with a longer, multi-day protocol.
Subjects were instructed to follow their regular habits, and the use of substances that might affect cardiometabolic responses (e.g. caffeine intake) was not restricted. However, given the design of the study, in which all measurements were taking within less than 1 h of each other in randomized order (for Fixed and Adaptive modes), we are confident that any effect on cardiometabolic outcomes would be largely consistent across trials and probably resulted in superior consistency to having withdrawal from habitually consumed substances if those had been restricted.
Cardiorespiratory and metabolic responses vary widely across people with different profiles of motor-incomplete spinal cord injury. Fixed mode generally elicited the highest responses or was at least only marginally lower (< 5%) than other OBA modes. This is in line with the actual mean assistance provided by the exoskeleton, which was lowest in Fixed mode for all subjects. Important considerations include whether the person has significant amounts of spasticity, how familiar they are with each mode, and how intense the OBA exercise stimulus is for each individual. Given these considerations, and depending on the rehabilitation/training goal, different levels of assistance during OBA may be utilized. Fixed mode is probably the optimal mode to produce cardiometabolic health benefits and cardiorespiratory fitness gains, albeit the latter may be limited for more highly functional individuals. Maximal or Adaptive mode are probably more suitable for maximizing step counts with less physiological and subjective exertion, and, for some subjects, Maximal assist mode is probably the only mode that can be sustained for prolonged periods.


 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize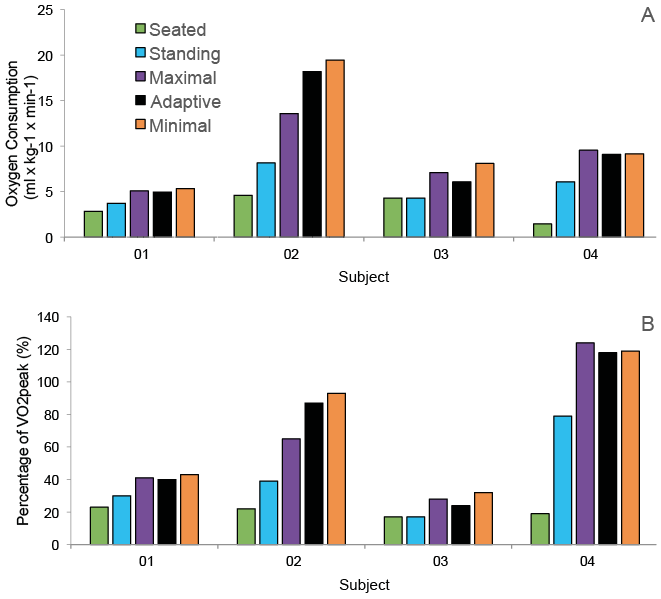 Click to show fullsize
Click to show fullsize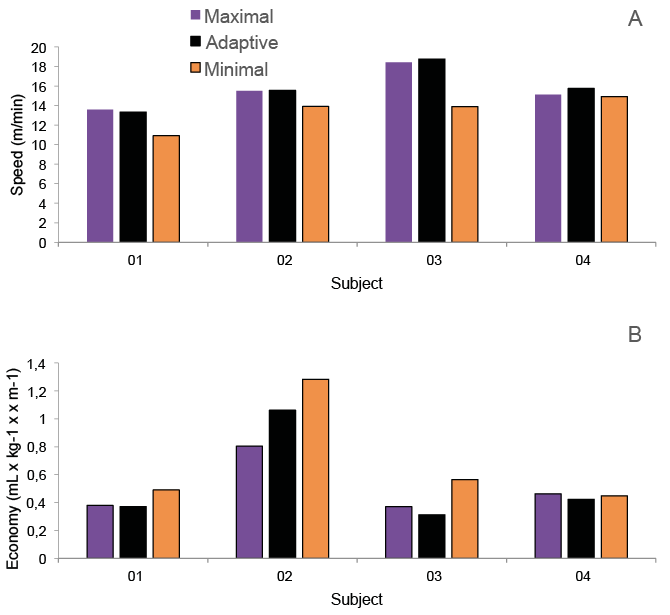 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize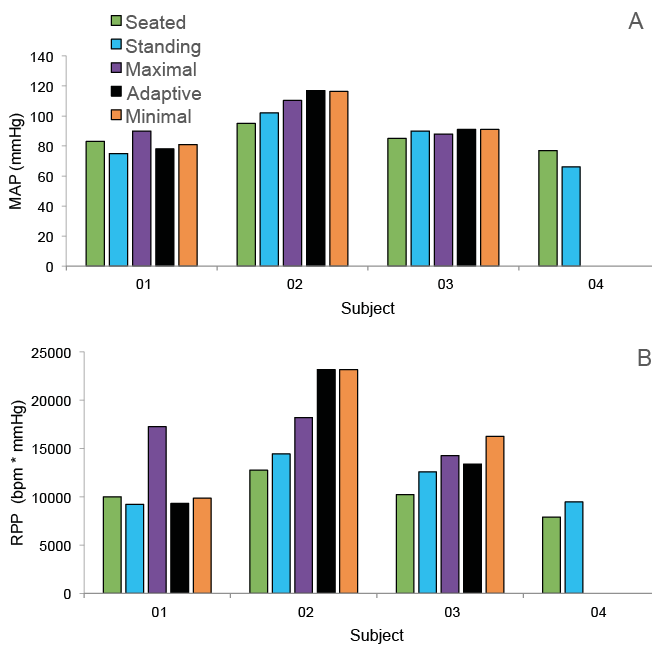 Click to show fullsize
Click to show fullsize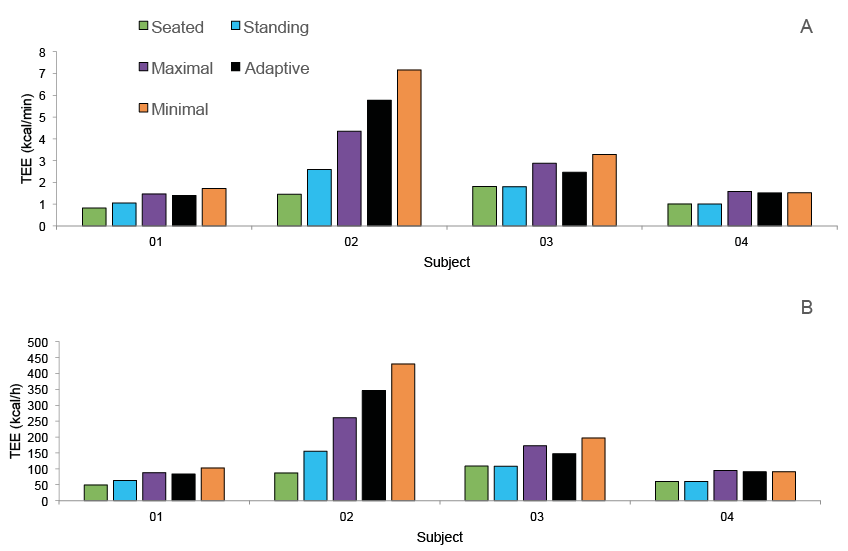 Click to show fullsize
Click to show fullsize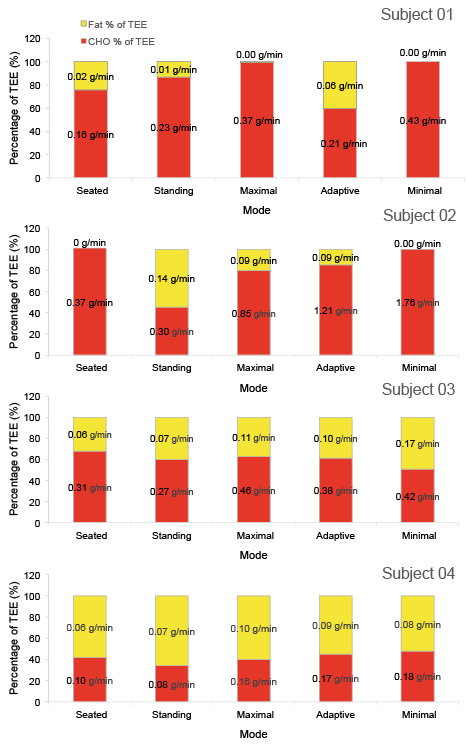 Click to show fullsize
Click to show fullsize