
From the 1Graduate Program in Rehabilitation Sciences, University of British Columbia, 2Rehabilitation Research Program, Vancouver Coastal Health Research Institute and 3Department of Physical Therapy, University of British Columbia, Canada
Objective: This retrospective cohort study identified inpatient rehabilitation admission variables that predict walking ability at discharge and established Berg Balance Scale cut-off scores to predict the extent of improvement in walking.
Methods: Participants (n = 123) were assessed for various cognitive and physical outcomes at admission to inpatient stroke rehabilitation. Multivariate logistic regression identified admission predictors of regaining community ambulation (gait speed ≥ 0.8 m/s) or unassisted ambulation (no physical assistance) after 4 weeks. Receiver operating characteristic curve analysis identified cut-off admission Berg Balance Scale scores.
Results: Mini-Mental State Examination (odds ratio (OR) 1.60, 95% confidence interval (95% CI) 1.19–2.14) was a significant predictor when coupled with admission walking speed for regaining community ambulation speed; stroke type (haemorrhagic/ischaemic) was a significant predictor (OR = 0.19, 95% CI 0.05–0.77) when coupled with Berg Balance Scale (OR 1.14, 95% CI 1.09–1.20). Only Berg Balance Scale was a significant predictor of regaining unassisted ambulation (OR 1.11, 95% CI 1.05–1.17). A cut-off Berg Balance Scale score of 29 on admission predicts that an individual will go on to achieve community walking speed (n = 123, area under the curve (AUC) = 0.88, 95% CI 0.81–0.95); a cut-off score of 12 predicts a non-ambulator to regain unassisted ambulation (n = 84, AUC 0.73, 95% CI 0.62–0.84).
Conclusion: The Berg Balance Scale can be used at rehabilitation admission to predict the degree of improvement in walking for patients with stroke.
Key words: walking; postural balance; stroke rehabilitation; gait; early ambulation.
Accepted Aug 29, 2017; Epub ahead of print Oct 25, 2017
J Rehabil Med 2018; 1: 00–00
Correspondence address: Janice Eng, Department of Physical Therapy, University of British Columbia, Vancouver, Canada, V6T 1Z3. E-mail: janice.eng@ubc.ca
After stroke, regaining mobility is a determining factor in discharge destination (1, 2); unsurprisingly, independent walking ranks among the top rehabilitation goals set by patients with stroke (3, 4). However, only 53% of patients with stroke regain independent walking ability after 4 weeks of rehabilitation (5) and only some of these will achieve a speed that allows safe navigation outdoors. Determining walking improvement over an inpatient stay in the early months post-stroke is important, as it coincides with the window of greatest neurological recovery (6), and will be less confounded by sedentary activity once the patient is at home or in more chronic stages. Neurological recovery is defined as the recovery of impairment and is often the result of brain recovery and reorganization; it has been increasingly recognized as being influenced by rehabilitation (7). Being able to predict a patient’s expected improvement upon admission to inpatient stroke rehabilitation may better streamline their treatment, goal-setting, and preparations for discharge.
Current research has identified several predictors of long-term mobility skills (6–12 months post-stroke), including cognitive impairment and recovery, initial walking speed and distance, balance, age, and presence of depressive symptoms (8–11). Research focused on discharge destination has found age, social support, sitting balance, cognition, and stroke severity to be significant predictors (12–16). However, despite the knowledge that most walking recovery will occur in the first 11 weeks after stroke (6), few studies have focused on predictors of walking improvement during this early time-period.
Balance is one of the few constructs that may have predictive value for early walking recovery (17). The Berg Balance Scale (BBS) is one of the most widely used and recognized balance measures (18, 19). The BBS has been validated in several populations, including stroke, and cut-off scores have been determined to identify those at risk of falls and those who need a gait aid for ambulation (19, 20). The BBS is commonly applied during inpatient rehabilitation, and has been shown to predict length of stay and discharge destination (19). It would be further useful for clinicians if specific values of the BBS were identified that predict whether patients will go on to walk without needing physical assistance or at speeds suitable for the community. The BBS is an ideal measure for this purpose, as it can be administered to patients who have very low function as well as those with preliminary ambulatory abilities.
The primary aims of this study were: (i) to identify the measures at admission to inpatient rehabilitation that predict discharge walking ability, and (ii) to establish BBS cut-off scores to predict improvements in walking. We hypothesized that cognitive function, in addition to admission physical function, is an important predictor of early walking recovery given that brain structures, such as the prefrontal cortex, show substantial activation during gait tasks in stroke (21).
This retrospective cohort study utilized data from a randomized controlled trial (ClinicalTrials.gov NCT00908479; full protocol available from authors) investigating the impact of a supplementary self-directed exercise programme in addition to inpatient stroke rehabilitation care, compared with standard stroke rehabilitation care alone on lower limb function. In that trial, participants in the intervention group received an exercise programme suitable to their functional level and were asked to complete 60 min of exercise in their own time, 6 days a week for 4 weeks. The self-directed exercise programme addressed range of motion and muscle stretching, muscle strengthening, weight-bearing, balance, and walking. Participants in the control group received an education book regarding stroke recovery and general health. Participants were assessed by a blinded evaluator at admission to rehabilitation, post-intervention at 4 weeks, as well as at 6 and 12 months post-stroke. Ethical approval for this randomized controlled trial was provided by the Human Research Ethics Board of the University of British Columbia and resource approval by the associated health authorities involved; written informed consent was obtained from all participants. As there were no significant differences between the supplementary programme group and control group at admission and at 4 weeks, the data from both groups were pooled for this cohort study. No adverse events associated with the intervention were observed throughout the randomized controlled trial. STROBE (STrengthening the Reporting of OBservational studies in Epidemiology) guidelines were followed to standardize the reporting of this analysis.
Participants were recruited from 5 participating inpatient rehabilitation hospitals in British Columbia, Canada, where patients are typically admitted 2–3 weeks post-stroke and spend 4 weeks in the inpatient stroke rehabilitation unit. Participants were recruited consecutively on admission and screened for eligibility within 72 h from November 2009 to December 2011; 12-month follow-up was completed by November 2012. Participants were included if: (i) lower extremity treatment had been identified as a goal by the patient and the rehabilitation team; their stroke occurred (ii) less than 4 weeks previously and (iii) was confirmed by a neurologist as an infarct or haemorrhage using either magnetic resonance imaging or computed axial tomography. Participants were excluded if they had unstable cardiovascular status, significant musculoskeletal or neurological conditions other than stroke, receptive aphasia or a Mini-Mental State Examination (MMSE) score below 20. Demographic characteristics (age, sex, stroke history) were collected in addition to the variables listed below. Participants were considered ambulatory if they were able to complete a 5-Meter Walk Test (5MWT) at any speed at the time of assessment without any hands-on physical assistance from a therapist.
The primary outcome for all study participants was walking ability at follow-up (after 4 weeks of inpatient rehabilitation) and whether they achieved a speed suitable for community ambulation. Individuals able to ambulate at 0.80 m/s or faster on their 5MWT were classified as community ambulators (22); participants who did not reach this speed were classified as non-community ambulators. Community ambulation is the ability to move about independently and safely outside of the home; a threshold speed to classify community ambulation is important as it facilitates discharge planning for the home and family (22). The 5MWT is a reliable, valid, and responsive measure of walking ability for sub-acute stroke and requires the individual to walk 9 m (23, 24), over which they are timed for the middle 5 to calculate comfortable walking speed. Unassisted ambulation was considered as a secondary outcome for the subset of individuals who were non-ambulatory at admission. Unassisted ambulation was defined as the ability to complete the 5MWT without physical assistance. This classification was selected because it removes the subjective clinician evaluation supervision or manual contact and focuses instead on the physical ability of the stroke survivor to walk over-ground, a factor that has strong implications for discharge planning and destination (25).
In order to identify factors associated with improvement in walking during inpatient stroke rehabilitation, we considered several independent variables representing the domains of stroke severity, cognition, mood, and balance. These domains were chosen as they have been shown to be associated with discharge destination and functional improvement during rehabilitation (10, 14, 16). Type of stroke (ischaemic/haemorrhagic) was also included, as there is evidence that survivors of haemorrhagic strokes have better functional prognosis after inpatient rehabilitation compared with those with ischaemic stroke (26). Treatment group from the original randomized controlled trial was also included as an independent variable to reduce bias, as this could be a confounding factor, despite the finding of no significant difference in walking speed between groups in the original study.
The Stroke Levity Scale (SLS) is a simple and quickly administered test of stroke severity (27). It is a 4-item measure that considers strength of the dominant upper extremity, strength in the hemiparetic lower extremity, general mobility, and presence of aphasia. The scale is scored out of 15, with higher scores indicating less severity. The SLS has been shown to be a valid and reliable measure of impairment in patients with stroke (27).
The MMSE is a 10-item screening tool for cognitive impairment (28). It is scored out of 30, with scores ranging from 18 to 24 indicating mild cognitive impairment in neurological patients, and scores below 18 indicating severe impairment. It tests the domains of orientation, memory, attention, calculation, and language, and is a valid screening tool of cognitive impairment for patients with stroke (29).
The Center of Epidemiological Studies-Depression Scale (CESD-10) (30) is a 10-question screening tool for depression and has been shown to have good sensitivity and specificity in patients with stroke (31). Each item is scored from 0 to 3 for a total of 30, with greater scores indicating more depressive symptoms; a subject scoring 10 or higher is considered depressed.
The BBS is a 14-item test of functional balance (18), with each item rated out of 4 for a total score of 56. It assesses static balance in sitting and standing, as well as dynamic balance during transitions and while in standing. Individuals who are able to maintain their balance for each task score higher on this outcome. The BBS is a valid measure of balance in stroke and has high intra- and inter-rater reliability, as well as excellent sensitivity to change (19).
Data were analysed using IBM SPSS Statistics (Mac version 22.0, IBM Corp, Armonk, New York, USA). Only participants with 4-week follow-up walking data were included in the analysis. Descriptive statistics were reported for demographic information and assessed variables for all subjects on admission, partitioned by those who achieved community ambulation (5MWT ≥ 0.8m/s) at 4 weeks and those who did not. Mean and standard deviation (SD) were reported when data were normally distributed; when not normally distributed, median and interquartile range (IQR) were reported. Demographic information and assessed variables were similarly reported for the subset of individuals who were non-ambulatory at admission, partitioned by whether unassisted ambulation was achieved by 4 weeks.
Multivariate logistic regression was used to identify the strongest predictors (independent variables) of achieving community ambulation speed at 4 weeks (dependent outcome). Spearman’s rank-order correlation (rho) was used to check for multicollinearity between independent variables; variables with a strong correlation (rho ≥ 0.7) were not used in the same logistic regression analysis and instead parallel models were generated. The following steps were taken to build the final models. Variables were entered into the initial multivariate analysis if they showed at least a moderate association with community ambulation (univariate logistic regression relationship of significance p < 0.25). From the initial multivariate model, variables were removed that were non-significant (p > 0.25), iteratively until a final model with only significant variables at level p < 0.05 was obtained. Predictors in the final model were controlled for an interaction effect, and were included in the model if the interaction contributed significantly (p < 0.05). All previously ruled out variables were re-inserted individually to check for significant contribution (p < 0.05). Time since stroke onset and treatment group from the overall randomized controlled trial were considered as potential confounders and were thus included in all models. Nagelkerke R square values were obtained, and the goodness of fit of each model was tested using receiver operating characteristic (ROC) curves. Each model is presented with p-values, unstandardized coefficients, and odds ratios (OR) with a 95% confidence interval (95% CI).
A similar multivariate logistic regression analysis was undertaken to identify the strongest admission predictors of unassisted ambulation (“ambulatory” or “non-ambulatory” at 4 weeks as dependent outcome) using similar methods.
ROC curve analysis was also performed to identify a BBS admission score that would predict walking ability at follow-up after 4 weeks of stroke rehabilitation. A cut-off BBS score was identified for the entire sample by selecting the coordinates on the ROC curve that maximized the sensitivity and specificity for distinguishing those who achieved a walking speed suitable for community ambulation from those who did not at 4-week follow-up. The same criteria were used to select the cut-off BBS score for non-ambulators on admission to distinguish those who regained unassisted walking ability after rehabilitation. Area under the curve (AUC) and accuracy statistics were calculated for each ROC curve and cut-off score, which reflect the discriminative value of the BBS in predicting walking ability after 4 weeks of inpatient rehabilitation.
Of 142 participants recruited at admission to inpatient rehabilitation, 123 remained in the study at the 4-week follow-up assessment. There were no significant differences between the 19 participants who dropped out (13.4%) and those who remained in the study. Demographic details and admission measures are shown in Table I for all 123 participants.
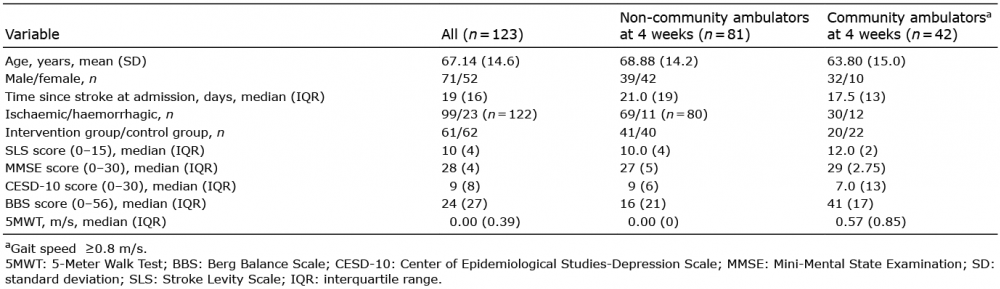
Table I. Participant characteristics at admission to inpatient stroke rehabilitation, grouped by community ambulatorsa and non-community ambulators at 4 weeks
The median time since stroke on admission was 19 days for the whole sample and therefore 47 days at the follow-up assessment, indicating that the majority of participants underwent inpatient rehabilitation within 6–7 weeks post-stroke, the optimal window for neurological recovery. As can be seen in Table I, there was a greater proportion of men in the group that achieved community ambulation (76.2%) than the group that did not (48.1%); similarly, a greater proportion of subjects experienced a haemorrhagic stroke in the community ambulation group (28.6%) than the non-community ambulation group (13.8%). The median admission BBS score of 41 for the group that achieved community ambulation by 4 weeks was more than twice the median score of 16 for the group that did not achieve community ambulation.
Demographic details and admission scores for the subgroup of individuals who were not ambulatory on admission are shown in Table II. Of note, the median admission BBS score for those who became ambulatory at discharge was more than 3 times greater than the median of those who remained non-ambulatory.
Table II. Characteristics of non-ambulators on admission, grouped by ambulatory status after 4 weeks of rehabilitation
The achievement of a speed suitable for community ambulation after rehabilitation was moderately associated (p < 0.25) with sex, age, stroke type, admission SLS, MMSE, BBS and 5MWT using univariate analysis with the whole sample (n = 123). There was a strong correlation (Spearman’s rho = 0.72) between BBS and 5MWT, and so 2 parallel multivariate analyses were performed. In the final model including BBS (Model A, Table III), stroke type and BBS were identified as significant predictors (p < 0.05). In the final model including 5MWT (Model B, Table III), MMSE and 5MWT were identified as significant predictors (p < 0.05). No significant interaction effects were included in either model; both models had similar Nagelkerke R square and AUC values. Interestingly, while time since stroke was included as a confounding variable in each model, it was shown to be significant in both models predicting community ambulation.
Table III. Parallel multivariate logistic regression models to predict community ambulation speed walking improvement after 4 weeks of rehabilitation
Of the 84 participants who were non-ambulatory on admission, 53 participants were able to walk without physical assistance by 6–7 weeks post-stroke at follow-up. On univariate logistic regression, time since stroke, stroke type, SLS, MMSE and BBS were found to have significant (p < 0.25) associations with walking outcome. However, when entered together into a multivariate logistic regression model (Table IV), only BBS remained a significant predictor (p < 0.05) of change in ambulatory status (OR = 1.11, 95% CI 1.0–1.17). Time since stroke was again a significant variable in predicting ambulation improvement. The final multivariate model had lower Nagelkerke R square and AUC values than those predicting community ambulation.
Table IV. Multivariate logistic regression model to predict unassisted ambulation after 4 weeks of rehabilitation
Investigation of the predictive value of the BBS score in identifying community ambulators using ROC curve analysis (n = 123) yielded an AUC of 0.88 (95% CI 0.81–0.95). The point on the curve that maximized both sensitivity (0.86) and specificity (0.84) corresponded with a cut-off score of 29 on admission to predict community ambulation at follow-up. For non-ambulators on admission (n = 84), a similar analysis yielded an AUC of 0.73 (95% CI 0.62–0.84) in identifying those who become ambulatory after 4 weeks of rehabilitation. The optimal cut-off score maximizing sensitivity (0.74) and specificity (0.68) on the curve was a BBS score of 12. Both curves are shown in Fig. 1. The likelihood ratios and predictive values for both BBS cut-off scores are reported in Table V.
Fig. 1. Receiver operating characteristic curves for predicting community ambulation ability (walking speed ≥ 0.8 m/s) or unassisted ambulation after inpatient rehabilitation using admission Berg Balance Scale (BBS) score.
Table V. Optimal Berg Balance Scale cut-off scores at admission to predict walking improvement after rehabilitation and receiver operating characteristic curve analysis statistics
This retrospective cohort analysis identified several clinical factors that, when measured at admission to inpatient rehabilitation, are able to predict walking ability at discharge. Better cognitive status, greater initial walking speed or balance ability, and haemorrhagic stroke were identified in parallel multivariate analyses to be predictors of achieving community walking speed (n = 123); only balance ability was a predictor for regaining unassisted walking (n = 84). Time since stroke was a significant covariate in all multivariate models, as was expected given that progress of time has been shown to be an important factor for recovery in the first 6–10 weeks after stroke (32). ROC curve analysis of the BBS scores found that a cut-off score of 29 is predictive of regaining community ambulation speed by discharge, and a cut-off score of 12 is predictive of regaining unassisted ambulation.
The establishment of BBS cut-off scores to predict unassisted ambulation or community ambulation has several implications for clinical practice. As the BBS is already a widely-used measure for rehabilitation, this interpretation of admission values may help to guide clinicians in their treatment focus. For example, clinicians may decide to spend more time practicing safe transfers or wheelchair skills for individuals with BBS scores less than 12. On the other hand, clinicians may wish to increase the intensity and duration of gait training for individuals who score 29 or higher on the BBS on admission, since the individual is likely to progress to walking speeds suitable for the community setting. Similarly, these cut-off scores may help guide other team members in planning for discharge based on the patient’s expected walking ability. It may also help to determine candidacy for rehabilitation (short-term vs. long-term, low intensity vs. high intensity) as well as length of stay.
A previous study by Bland et al. (17) identified a cut-off admission score of 20 on the BBS, in combination with a Functional Independence Measure walk item score of 1 or 2 (maximum to total assistance to walk), which distinguishes household ambulators from community ambulators at discharge. Our finding of a cut-off score of 29 for a community ambulator is a full 9 points higher; however, Bland et al. used a much lower speed (> 0.40 m/s) to classify community ambulators. In their study, 2 samples of participants were admitted to rehabilitation a median of 4 and 5 days post-stroke, and discharged after a median of 14 and 17 days of rehabilitation, respectively (a total timeline of 3 weeks post-stroke). In contrast, maximum walking improvement after a stroke is achieved at between 3 and 11 weeks, depending on the degree of lower extremity impairment (6). It is possible that more of their participants would go on to become independent or community ambulators simply with more time as neurological recovery is still ongoing. Another previous study, by Makizako et al. (33), determined a cut-off BBS score of 13 on admission to inpatient rehabilitation that predicts independent walking at 12 weeks post-stroke. Our similar finding of a cut-off score of 12 for non-ambulators who no longer need physical assistance by 7 weeks post-stroke, rather than 12 weeks post-stroke, may suggest that much of the recovery for walking has already plateaued by the 7-week time-point for those with low balance ability.
It is important to note that the likelihood ratios and predictive values listed in Table IV indicate that the cut-off score of 29 for community ambulation has better predictive accuracy than the cut-off score of 12 for unassisted ambulation. This may, in part, reflect the smaller sample size for the unassisted walking analysis (n = 84) compared with the community ambulation analysis (n = 123). This may also reflect the subjectivity as to whether the clinician feels that a patient is safe to walk without hands-on supervision, which can be influenced by factors such as patient vs. therapist size, patient predictability, and therapist confidence. Another reason for the lower diagnostic accuracy for predicting unassisted ambulators may relate to confounding non-physical factors that might affect early performance in walking or on the BBS, such as cognition and mental status, motivation, pain, behaviour, and depression.
This study also found that individuals with higher cognitive scores have greater odds of achieving a gait speed suitable for community mobility. A previous cross-sectional study one year after stroke has shown that executive function and cognition are associated with balance and mobility in the community (34). Our current study advances these findings with a retrospective cohort design, which demonstrated that achieving community walking speed could be predicted over time by initial cognitive status during inpatient rehabilitation. It is not surprising that cognition is associated with improvements in ambulation during rehabilitation; various brain imaging studies have shown that activation and functional connectivity of the prefrontal and premotor cortices are necessary to perform simple and complex walking tasks (21). A meta-analysis of neuroimaging studies has suggested that the premotor cortex serves as a gateway between cognitive and motor networks (35); as such, greater premotor activation is associated with greater walking outcomes in patients with stroke (36).
It was also shown in this study that those with a haemorrhagic stroke have greater odds of regaining community walking, compared with ischaemic stroke. This is in line with previous findings that functional outcomes after haemorrhagic stroke tend to be greater than after ischaemic stroke, if all other variables (initial severity, age, mortality) are controlled (26). It is posited that the difference in recovery after ischaemic or haemorrhagic stroke are due to the neurological processes occurring with each stroke; neurological functions recover as a haematoma and brain compression resolves, compared with axonal sprouting and cortical re-organization after ischaemic cell death (26, 37).
The results are contingent on how unassisted and community ambulation were defined in this study, which was based on aspects of a self-paced walking measure. Such measures do not directly account for the safety, endurance, or tolerance of the participant, nor do they measure whether an individual actually participates in walking activities in their home or community. However, self-paced walking speed is one of the most common measures evaluated after a stroke and has been shown to predict community ambulation (38, 39). Various speed thresholds have been proposed to distinguish home and community ambulators, ranging from 0.4–0.93 m/s (22, 38); our selection of a 0.8 m/s threshold is on the higher end of this range. It is important to note that measures of physical function, including gait speed, explain only a fraction of the variation in community and home participation after stroke (40). Various other factors not considered in this study, such as self-efficacy, motivation, and socioeconomic status, are probably associated with community participation.
This study has several limitations. The generalizability of the study findings is limited to those that meet the inclusion and exclusion criteria for the randomized controlled trial in which the participants were enrolled. These included a minimum score of 20 on the MMSE and admission to rehabilitation within 4 weeks of stroke. However, the majority of patients admitted to inpatient rehabilitation would meet this cognition threshold, as they are required to participate actively in a full-day programme. Another limitation of the study is that other measures that may impact improvement during rehabilitation and overall walking function were not included. For example, lower extremity impairment (somatosensation, spasticity) was not specifically measured yet may impact balance and walking ability. Finally, as mentioned previously, community ambulation was classified according to walking speed in a controlled laboratory setting, which may not necessarily reflect whether an individual is truly comfortable walking in the community.
In conclusion, this study identified balance ability at admission to rehabilitation as a significant predictor of walking improvements during the first 6–7 weeks after stroke when the most recovery is expected to occur. Having an understanding of prognosis at the time of admission will assist clinicians in making decisions for specific interventions and discharge planning. Our results indicate that an individual with a BBS score of 29 or greater upon admission to rehabilitation is highly likely to achieve walking speeds suitable for community ambulation by 6–7 weeks post-stroke, and that those who score 12 or higher are likely to regain independence in walking. Cognitive status at admission was also found to predict walking ability, and should be considered by clinicians in therapeutic and prognostic decision-making.
This work was supported by the Canadian Institutes of Health Research, Heart and Stroke Foundation of BC and Yukon, and Canadian Partnership for Stroke Recovery.
The authors declare no conflicts of interest.


 Click to show fullsize
Click to show fullsize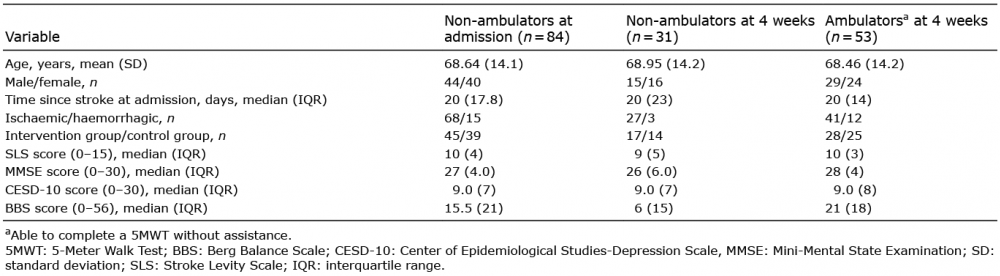 Click to show fullsize
Click to show fullsize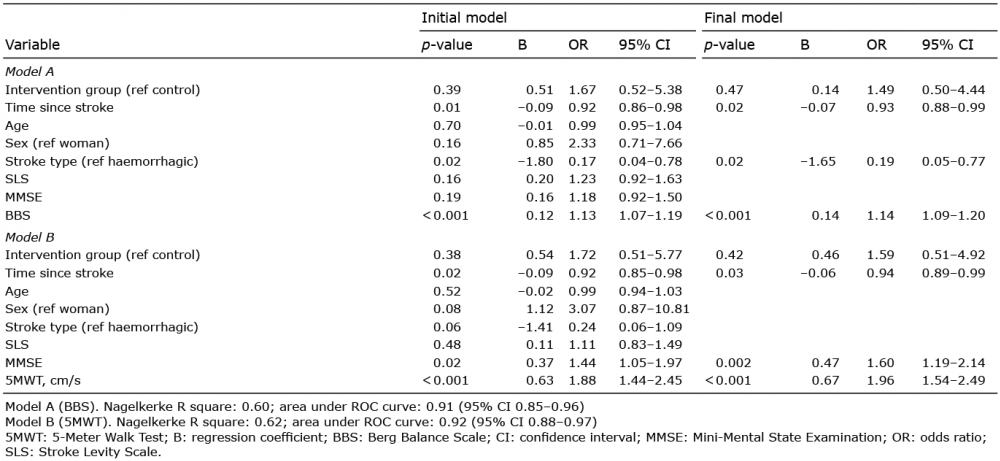 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize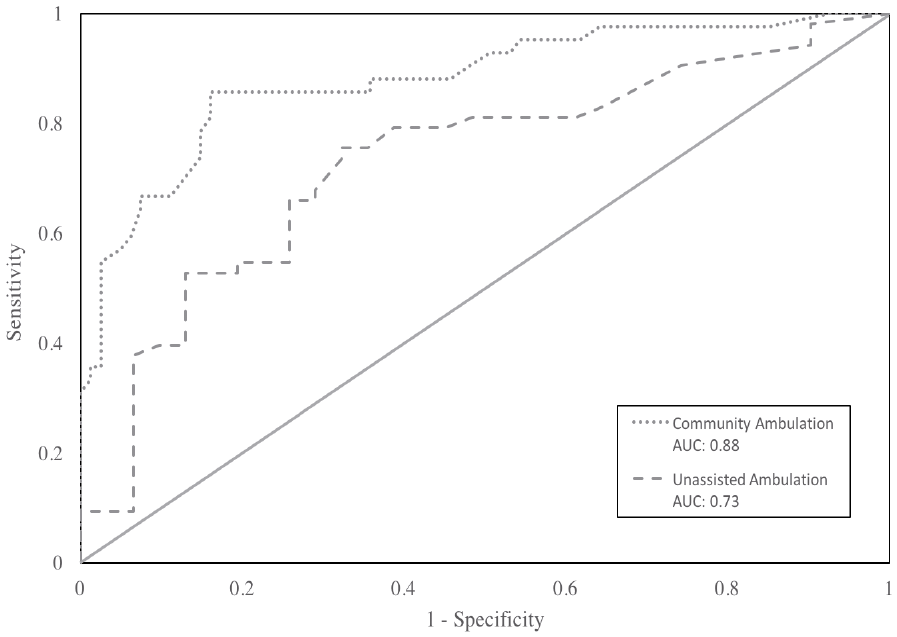 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize