
From the 1Department of Physical Therapy, Faculty of Health and Welfare, Tokushima Bunri University, Tokushima, 2Department of Rehabilitation, Kasei Tamura Hospital, Wakayama and 3Life and Medical Sciences Area, Health Sciences Discipline, Kobe University, Kobe, Japan
Objective: To determine the cut-off values for knee extensor strength on the paretic and non-paretic sides and both sides combined for identifying independence in gait in chronic stroke survivors.
Design: Cross-sectional study.
Patients: Sixty chronic stroke survivors.
Methods: Functional Independence Measure (FIM) gait scores were measured, and the participants were allocated to the independent group (FIM gait score 6 or 7) or the dependent group (FIM gait score 1–5). Knee extensor strength on the paretic and non-paretic sides was measured using a handheld dynamometer.
Results: Eighteen stroke survivors were allocated to the independent group and 42 to the dependent group. The receiver operating characteristic curve analyses revealed that the cut-off values for knee extensor strength were 0.46 Nm/kg (sensitivity 83% and specificity 67%; area under the curve (AUC) 0.816) on the paretic side, 0.65 Nm/kg (sensitivity 89% and specificity 55%; AUC 0.738) on the non-paretic side and 1.31 Nm/kg (sensitivity 83% and specificity 74%; AUC 0.811) for both sides combined.
Conclusion: These cut-off values could help to identify stroke survivors who are no longer independent in gait because of decreasing knee extensor strength on the paretic and non-paretic sides.
Key words: cut-off value; independence in gait; knee extensor strength; chronic stroke survivors.
Accepted Aug 29, 2017; Epub ahead of print Sep 26, 2017
J Rehabil Med 2017; 49: 00–00
Correspondence address: Naoki Akazawa, Department of Physical Therapy, Faculty of Health and Welfare, Tokushima Bunri University, Boji 180, Nishihama, Yamashiro-cho, Tokushima-city, Tokushima 770-8514, Japan. E-mail: akazawa@tks.bunri-u.ac.jp
Regaining independence in gait is the main goal of stroke rehabilitation and is closely related to increased muscle strength in the paretic and non-paretic lower extremities (1, 2). In particular, knee extensor strength is closely related to gait ability in stroke survivors (3, 4). A previous study (5) reported that independence in sit-to-stand was predicted not only by the knee extensor strength on the paretic and non-paretic sides, but also by the knee extensor strength of both sides combined. Therefore, measuring knee extensor strength on the paretic and non-paretic sides is common clinical practice (6−8).
Identifying independence in gait is important to prevent the decreased muscle strength (9) and inactivity (10) that often occur after stroke. However, cut-off values have not yet been determined for knee extensor strength on the paretic and non-paretic sides individually or combined. We believe that determining such cut-off values could help to identify stroke survivors whose dependence in gait might be caused by decreasing knee extensor strength. The aim of this study was therefore to determine the cut-off values for knee extensor strength on the paretic and non-paretic sides individually and combined, which can be used to identify independence in gait in chronic stroke survivors.
Sixty stroke survivors who lived in the community participated in this study. Participants were recruited using advertisements and enrolled from October 2014 to September 2016. The inclusion criterion was first-ever chronic stroke survivor (> 6 months latency/time since stroke). Participants with a history of dementia or aphasia were excluded. Each participant provided written informed consent prior to participation, and the study protocol was approved by the ethics committee of our institution.
Knee extensor strength on the paretic and non-paretic sides was measured. Age, sex, body mass index, type of stroke, time since stroke, Functional Independence Measure (FIM) gait score (11) and use of cane and lower extremity orthosis were also measured.
Knee extensor strength was measured using a handheld dynamometer (micro FET2, Hoggan Health Industries, Salt Lake, USA). A handheld dynamometer was placed just proximal to the ankle on the anterior surface of the leg while the participant was seated with knees and hip flexed to 90° (12). We asked participants to produce the maximum knee extensor strength contraction for 3–4 s. Two measurements were performed by the same physical therapist. The maximum value was used to calculate torque by multiplying strength (N) by the length of the lever arm (m). Knee extensor strength on the paretic and non-paretic sides was estimated as torque on each side divided by body weight (Nm/kg). Knee extensor strength on the paretic and non-paretic sides combined was estimated as the sum of the torque on the two sides divided by body weight. A previous study (12) reported that measurement of isometric knee extensor strength using a handheld dynamometer in neurological disease had high test-retest reliability (r = 0.98).
Sixty stroke survivors were allocated to the independent group (defined as a FIM gait score of 6 or 7) and dependent group (defined as a FIM gait score of 1–5) (13). The characteristics of the independent and dependent groups were compared using the Mann–Whitney U test, χ2 test and Fisher’s exact test.
Multiple logistic regression analyses were used to identify the relationship between independence in gait and knee extensor strength on the paretic side, non-paretic side and both sides combined. Any factors that showed a significant difference in the univariate analysis were treated as covariates. The areas under the curves (AUC) were calculated using the receiver operating characteristic (ROC) curves for knee extensor strength on the paretic and non-paretic sides and both sides combined. The cut-off values were determined based on the Youden index and p-values <0.05 were defined as significant. Statistical analyses were conducted using SPSS version 24 (IBM SPSS Japan, Tokyo, Japan).
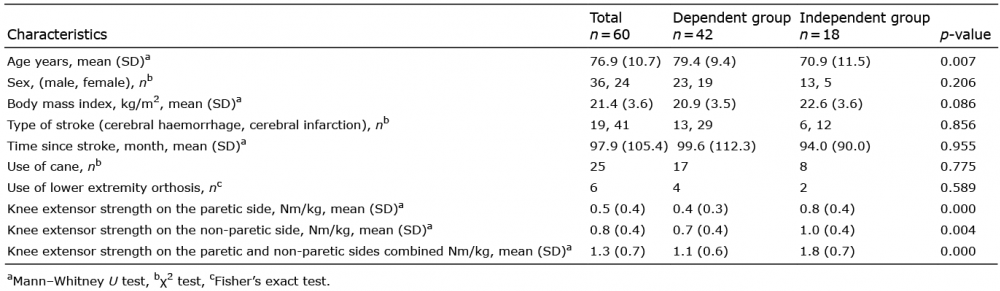
Table I shows the characteristics of all participants (n = 60, FIM gait score: median [interquartile] = 4.0 [2.0–6.0]) and the dependent (n = 42, FIM gait score: median [interquartile] = 3.0 [2.0–4.3]) and independent (n = 18, FIM gait score: median [interquartile] = 7.0 [6.0–7.0]) groups. The mean age was significantly lower in the independent group than in the dependent group (Table I). The knee extensor strength for all three measures was significantly greater in the independent group than in the dependent group (Table I).
Table I. Characteristics of all participants and comparisons of characteristics between groups
Multiple logistic regression analyses adjusted for age showed that knee extensor strength on the paretic (odds ratio 42.86; 95% confidence intervals (CI) 4.04–454.57; p < 0.01) and non-paretic sides (odds ratio 5.93; 95% CI 1.11–31.62; p < 0.05) and both sides combined (odds ratio 5.33; 95% CI 1.73–16.47; p < 0.01) were significant variables. ROC analyses revealed that the AUC for knee extensor strength was 0.816 (p < 0.01) on the paretic side, 0.738 (p < 0.01) on the non-paretic side and 0.811 (p < 0.01) for the two sides combined (Fig. 1). The cut-off value for knee extensor strength was 0.46 Nm/kg (sensitivity 83% and specificity 67%) on the paretic side, 0.65 Nm/kg (sensitivity 89% and specificity 55%) on the non-paretic side and 1.31 Nm/kg (sensitivity 83% and specificity 74%) for both sides combined (Fig. 1).
Fig. 1. Receiver operating characteristic curves for knee extensor strength on the paretic and non-paretic sides and both sides combined for identifying independence in gait. Circle=cut-off value for knee extensor strength on the paretic side (0.46 Nm/kg); triangle=cut-off value for knee extensor strength on the non-paretic side (0.65 Nm/kg); square=cut-off value for combined knee extensor strength on the paretic and non-paretic sides (1.31 Nm/kg).
The cut-off values for knee extensor strength for identifying independence in gait in chronic stroke survivors were 0.46, 0.65 and 1.31 Nm/kg on the paretic and non-paretic sides and both sides combined. In addition, the AUC values for the knee extensor strength on the paretic and non-paretic sides and the two sides combined were 0.816, 0.738 and 0.811. AUC values of 0.7–0.9 can be interpreted as moderately accurate (14). Thus, the AUC values in this study indicate moderate accuracy for identifying independence in gait.
These results show that knee extensor strength is closely related to independence in gait. Independence in sit-to-stand is predicted not only by knee extensor strength on the paretic and non-paretic sides, but also by the combined strength of the two sides (5). In addition, improvement in gait independence is related to increased lower extremity extensor strength on the paretic and non-paretic lower extremities (2). Our results are consistent with these findings.
Resistance training is effective for increasing the knee extensor strength on the paretic and non-paretic sides in chronic stroke survivors (15). When a chronic stroke survivor is not independent in gait, we recommend measuring the knee extensor strength on the paretic and non-paretic sides and estimating the combined knee extensor strength. If these measurements are below the cut-off values reported here, the patient may benefit from resistance training.
The study limitations include the small sample size and limited statistical power, which preclude us from ruling out chance findings. In addition, this study recruited chronic stroke survivors who lived in the community. Therefore, whether the cut-off values revealed in this study can be generalized to acute stroke survivors who are hospitalized is unclear. Further studies are needed to determine the cut-off values in acute settings.
In conclusion, the cut-off values for knee extensor strength on the paretic and non-paretic sides and combined were 0.46, 0.65 and 1.31 Nm/kg, respectively. These cut-off values could help to identify stroke survivors whose dependence in gait might be caused by decreased knee extensor strength on the paretic and non-paretic sides.
The authors thank the participants and staff members who helped with this study.
The authors declare no conflicts of interest.


 Click to show fullsize
Click to show fullsize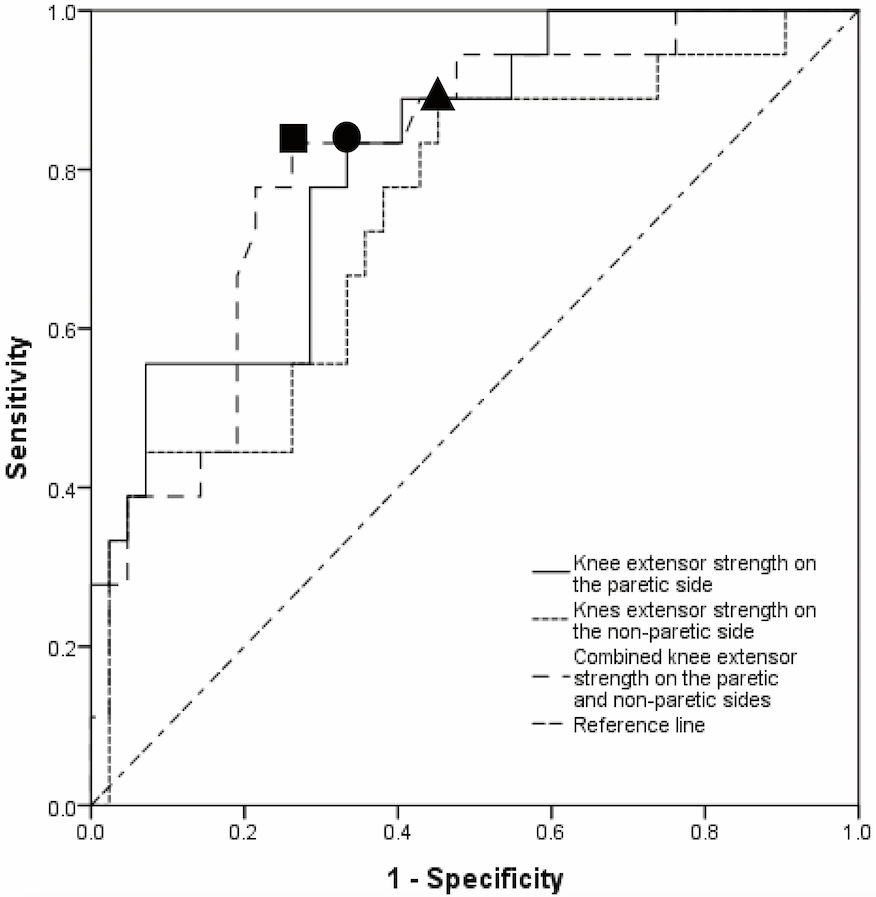 Click to show fullsize
Click to show fullsize