
From the 1Department of Orthopaedics, The Ninth People’s Hospital of Chongqing, 2Department of Neurology, The Ninth People’s Hospital of Chongqing, 3Department of Orthopaedics, The People’s Hospital of Bishan District, Bishan, Chongqing, China
Introduction: Transcutaneous electrical nerve stimulation is a possible adjunctive therapy to pharmacological treatment for controlling pain after total knee arthroplasty. However, the results are controversial. A systematic review and meta-analysis was conducted to explore the effect of transcutaneous electrical nerve stimulation on patients with total knee arthroplasty.
Methods: PubMed, Embase, Web of Science, EBSCO, and Cochrane Library databases were searched systematically. Randomized controlled trials assessing the effect of transcutaneous electrical nerve stimulation on patients with total knee arthroplasty were included. Two investigators independently searched articles, extracted data, and assessed the quality of included studies. Primary outcome was visual analogue scale (VAS) score over a period of 24 h. Meta-analysis was performed using a random-effect model.
Results: Six randomized controlled trials involving 529 patients were included in the meta-analysis. Overall, compared with control intervention, transcutaneous electrical nerve stimulation supplementation intervention was found to significantly reduce VAS scores and total postoperative morphine dose over a period of 24 h, and to improve active range of knee motion (standard mean difference (SMD) = 0.37; 95% confidence interval (95% CI) = 0.06–0.68; p = 0.02), but had no effect on VAS scores at 2 weeks (SMD = 0.20; 95% CI = –0.07 to 0.48; p = 0.15).
Conclusion: Compared with control intervention, transcutaneous electrical nerve stimulation supplementation intervention was found to significantly reduce pain and morphine requirement over a period of 24 h and to promote functional recovery in patients who have undergone total knee arthroplasty.
Key words: transcutaneous electrical nerve stimulation; total knee arthroplasty; adjunctive therapy; pain control; meta-analysis.
Accepted Aug 11, 2017; Epub ahead of print Sep 21, 2017
J Rehabil Med 2017; 49: 00–00
Correspondence address: Lihua Peng, Department of Orthopaedics, The People’s Hospital of Bishan District, Bishan, Chongqing 402760, P.R. China. E-mail: 363670397@qq.com
Total knee arthroplasty (TKA) is widely accepted as the most common approach to improve function and control pain for patients with degenerative knee osteoarthritis (OA) (1, 2). However, rehabilitation exercises (e.g. flexion/extension of the knee) can be very painful and severe pain may lead to poor functional recovery (3–5). Pharmacological treatment is ineffective for controlling severe pain during rehabilitation (6, 7).
Transcutaneous electrical nerve stimulation (TENS) is reported to be efficacious for better pain management when used as a supplement to pharmacological analgesia during rehabilitation exercises. Both the peripheral and the central nervous systems are involved in the analgesic action of TENS through activating endogenous inhibitory mechanisms of opioid receptors in the central nervous system (8–11), and reducing central neurone sensitization and primary and secondary mechanical hyperalgesia (12, 13).
Previous studies have shown that TENS can reduce postoperative movement pain after various surgeries (8, 14). TENS has been reported to have important capability for pain relief and functional recovery after TKA (15, 16). In contrast to this promising finding, however, accumulating RCTs have shown that TENS has no influence on pain control and function improvement (17, 18). In order to elucidate these inconsistent results, a systematic review and meta-analysis of RCTs was conducted to investigate the influence of TENS on patients with TKA.
This systematic review and meta-analysis were conducted according to the guidelines of the Preferred Reporting Items for Systematic Reviews and Meta-analysis statement (19) and the Cochrane Handbook for Systematic Reviews of Interventions (20).
PubMed, Embase, Web of Science, EBSCO, and the Cochrane Library were systematically searched from inception to January 2017, with the following key words: transcutaneous electrical nerve stimulation or TENS, and total knee arthroplasty or TKA or total knee replacement or TKR. No limitations were set. To include additional eligible studies, the reference lists of retrieved studies and relevant reviews were also hand-searched and the process above was performed repeatedly until no further article was identified. Conference abstracts meeting the inclusion criteria were also included.
Inclusion criteria were: study population, patients with TKA; intervention, TENS; control, placebo; outcome measure, visual analogue scale (VAS) scores during 24 h; and study design, RCT.
The following information was extracted for the included RCTs: first author, publication year, sample size, baseline characteristics of patients, TENS intervention, control, study design, VAS scores during 24 h, total postoperative morphine dose over a period of 24 h, VAS scores and active range of knee motion (°) at 2 weeks. The author would be contacted to acquire the data when necessary.
The primary outcome was VAS scores during 24 h. Secondary outcomes included total postoperative morphine dose over a period of 24 h, VAS scores and active range of knee motion (°) at 2 weeks.
The Jadad scale was used to evaluate the methodological quality of each RCT included in this meta-analysis (21). This scale consisted of 3 evaluation elements: randomization (0–2 points), blinding (0–2 points), drop-outs and withdrawals (0–1 points). One point would be allocated to each element if they have been mentioned in article, and another point would be given if the methods of randomization and/or blinding had been detailed and appropriately described. If methods of randomization and/or blinding were inappropriate, or drop-outs and withdrawals had not been recorded, then 1 point was deducted. The score of Jadad scale varies from 0 to 5 points. An article with Jadad score ≤ 2 was considered to be of low quality. If the Jadad score was ≥ 3, the study was thought to be of high quality (22).
Standard mean differences (SMDs) with 95% confidence intervals (95% CIs) for continuous outcomes (VAS scores during 24 h, total postoperative morphine dose over a period of 24 h, VAS scores and active range of knee motion (°) at 2 weeks) were used to estimate the pooled effects. All meta-analyses were performed using random-effects models with DerSimonian and Laird weights. Heterogeneity was tested using the Cochran Q statistic (p < 0.1) and quantified with the I2 statistic, which described the variation of effect size that was attributable to heterogeneity across studies. An I2 value greater than 50% indicated significant heterogeneity. Sensitivity analysis was performed to detect the influence of a single study on the overall estimate via omitting one study in turn when necessary. Owing to the limited number (< 10) of included studies, publication bias was not assessed. p <0.05 in 2-tailed tests was considered statistically significant. All statistical analyses were performed with Review Manager Version 5.3 (The Cochrane Collaboration, Software Update, Oxford, UK) or Stata 12.0 software (StataCorp, College Station, TX, USA).
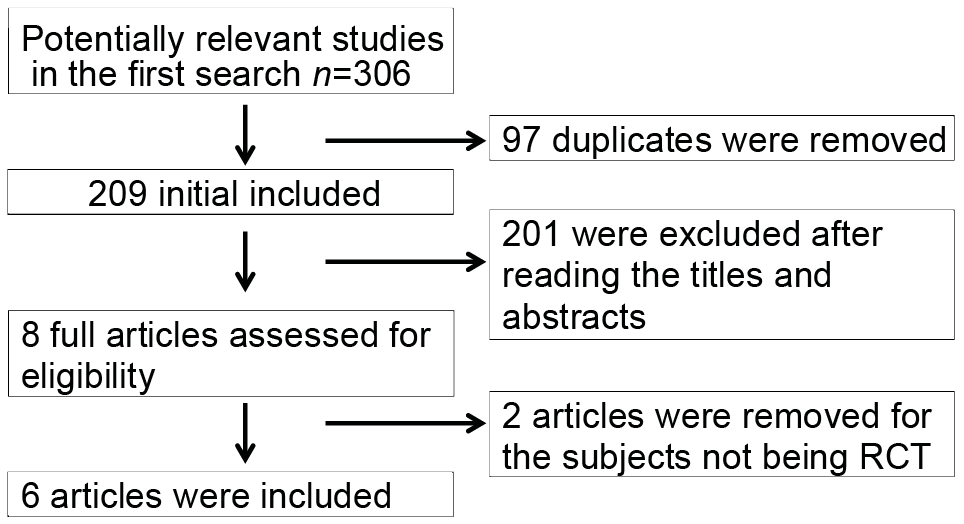
The flow chart for the selection process and detailed identification is shown in Fig. 1. A total of 306 publications were identified through the initial search of databases. Ultimately, 6 RCTs were included in the meta-analysis (4, 15–18, 23).
Fig. 1. Flow diagram of study searching and selection process. RCT: randomized controlled trial.
The baseline characteristics of the 6 eligible RCTs in the meta-analysis are summarized in Table I. The 4 studies were published between 2003 and 2014, and sample sizes ranged from 30 to 246, with a total of 529. The follow-up time varied from 24 h to 9.5 months.
Table I Characteristics of included studies
The follow-up time varied from 24 h to 9.5 months.
Among the 6 RCTs, 2 studies reported VAS scores during 24 h (15, 16), 2 studies reported total postoperative morphine dose over a period of 24 h (16, 18), 2 studies reported VAS scores and active range of knee motion (°) at 2 weeks (15, 17). Jadad scores of the 6 included studies varied from 3 to 4, all 6 studies were considered to be high-quality according to quality assessment.
These 2 outcome data were analysed with a random-effects model, the pooled estimate of the 2 included RCTs suggested that, compared with control group, TENS intervention was associated with a significantly decreased VAS scores over a period of 24 h (standard mean difference = –0.47; 95% CI = –0.87 to –0.08; p = 0.02), with no heterogeneity among the studies (I2 = 0%, heterogeneity p = 0.79) (Fig. 2).
Fig. 2. Forest plot for meta-analysis of visual analogue scale (VAS) scores during 24 h. SD: standard deviation; TENS: transcutaneous electrical nerve stimulation; 95% CI: 95% confidence interval.
No heterogeneity was observed among the included studies for VAS scores over a period of 24 h. Thus, we did not perform sensitivity analysis by omitting one study in each turn to detect the source of heterogeneity.
Total postoperative morphine dose in the TENS group was found to be significantly lower than in the control group (SMD = –0.81; 95% CI = –1.44 to –0.18; p = 0.012; Fig. 3).
Fig. 3. Forest plot for meta-analysis of total postoperative morphine dose over a period of 24 h. TENS: transcutaneous electrical nerve stimulation; 95% CI: 95% confidence interval.
Compared with control intervention, TENS supplementation showed no significant influence on VAS scores at 2 weeks (SMD = 0.20; 95% CI = –0.07 to 0.48; p =0.15; Fig. 4), but showed better active range of knee motion (SMD = 0.37; 95% CI = 0.06 to 0.68; p = 0.02; Fig. 5).
Fig. 4. Forest plot for the meta-analysis of visual analogue scale (VAS) scores at 2 weeks. TENS: transcutaneous electrical nerve stimulation; SD: standard deviation; 95% CI: 95% confidence interval.
Fig. 5. Forest plot for the meta-analysis of active range of knee motion (°) at 2 weeks. TENS: transcutaneous electrical nerve stimulation; SD: standard deviation; 95% CI: 95% confidence interval.
This meta-analysis shows that, compared with control intervention, TENS supplementation intervention was associated with a significantly reduced VAS scores and total postoperative morphine dose at 24 h, but had no influence on VAS scores at 2 weeks. This indicates that TENS supplementation could substantially promote immediate pain relief following TKA, but has no effect on pain control over a relatively long follow-up after TKA. This may be due to pain intensity remaining at a low level over the follow-up. Furthermore, this low-intensity pain may not affect the functional performance of knee movement exercise and the quality of life of patients.
In addition, TENS supplementation intervention was found to significantly improve function of knee movement, as shown by active range of knee motion. One included study reported that, approximately 9 months post-operation, TENS supplementation resulted in a significantly increased knee injury and osteoarthritis outcome score (KOOS), suggesting its ability to improve knee function over long-term follow-up (17). To the best of our knowledge, this is the first meta-analysis of the treatment efficacy of TENS supplementation for TKA.
Another included study reported that patients with low trait anxiety in a TENS group had a significant decrease in range-of-motion pain (4), which was consistent with 1 RCT (24). Our meta-analysis suggested that less morphine was required for patients receiving TENS than for those receiving placebo-TENS. These results indicate that psychological factors and TENS determine the intensity of pain after surgery and patients with low trait anxiety could benefit more from TENS treatment. In addition, high-frequency TENS with a strong amplitude (30–40 mA) was reported to significantly reduce pain after quadriceps femoris contraction and to promote muscle contraction (18, 25). However, TENS amplitude (or dose) may have no influence on outcome data (4).
There are several limitations to this systematic review and meta-analysis that should be taken into account. Firstly, the analysis was based on only 6 RCTs, 4 of which had a relatively small sample size (n < 100). Overestimation of the treatment effect is more likely in smaller trials compared with larger samples. The included studies had different intensities of TENS and follow-up times, which may have affected the pooled results. In addition, the influence of ethnic diversity on the treatment efficacy of TENS remains unknown. Finally, some unpublished and missing data may have biased the pooled effect.
In conclusion, TENS supplementation intervention showed an important ability to reduce immediate pain after TKA and facilitated the recovery of knee function. It is recommended that TENS supplementation is used for patients with TKA, although further studies are needed to determine the optimal duration time and intensity of TENS.
The authors declare no conflicts of interest.


 Click to show fullsize
Click to show fullsize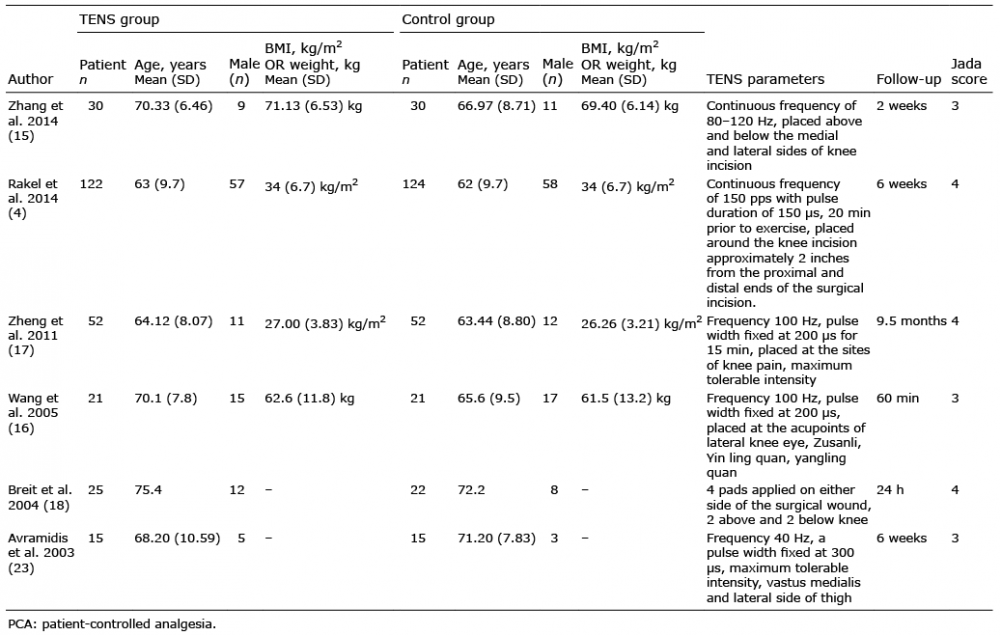 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize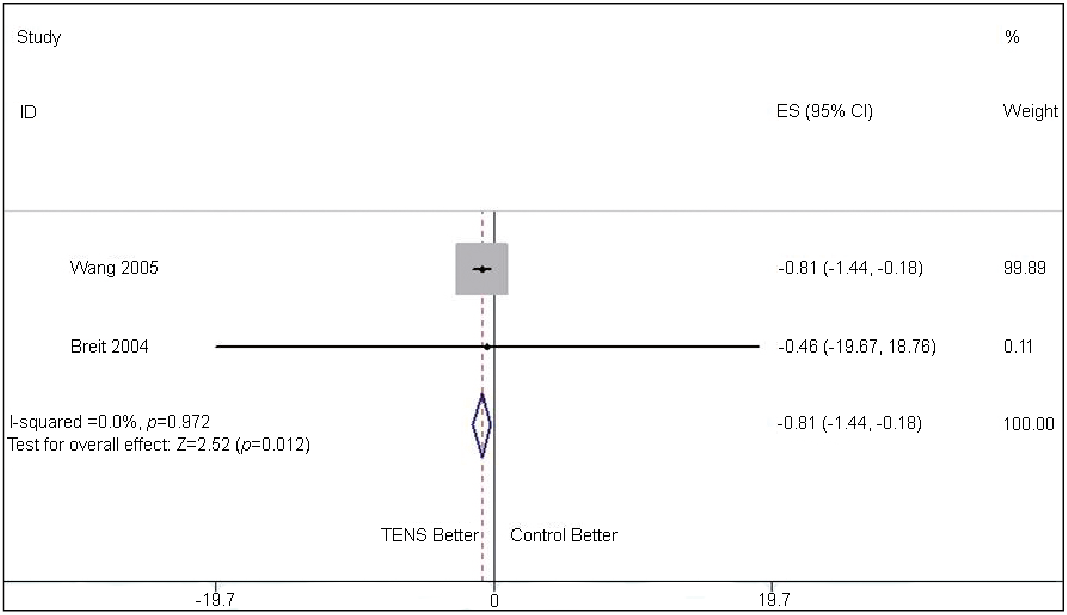 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize