
From the 1Department of Palliative Rehabilitation and Integrative Medicine, University of Texas MD Anderson Cancer Center, 2Department of Cancer Rehabilitation, Allina Health Services, Courage Kenny Rehabilitation Institute, 3Section of Benign Hematology, 4Department of Gynecological Oncology and Reproductive Medicine, 5Department of Biostatistics, University of Texas MD Anderson Cancer Center and 6University of North Texas Health Science Center, Texas College of Osteopathic Medicine, Fort Worth, TX, USA
Objective: To determine the frequency of venous thromboembolism, possible predictors, and the association between venous thromboembolism and Functional Independence Measure (FIM) scores and length of stay among cancer patients admitted to the inpatient rehabilitation unit at a cancer centre.
Design: Retrospective analysis of patients admitted to acute inpatient rehabilitation from September 2011 to June 2013.
Subject/patients: Cancer patients in the acute inpatient rehabilitation unit within a tertiary cancer centre.
Methods: International Classification of Diseases (ICD-9) codes identified deep vein thrombosis, pulmonary embolism, and inferior vena cava filter.
Results: Venous thromboembolism occurred in 32/611 patients (5.2%): 23/611 (3.8%) during the course of hospitalization before admission to rehabilitation, and 9/611 patients (1.5%) during rehabilitation. Patients with lower extremity oedema at admission (p = 0.0218) had a higher chance of subsequently developing venous thromboembolism. Patients with venous thromboembolism during rehabilitation had a significantly lower FIM transfer score at admission to rehabilitation (p = 0.0247), a longer length of stay in rehabilitation (p = 0.0013) and overall hospitalization (p = 0.0580).
Conclusion: Cancer patients with low FIM transfer scores and lower extremity oedema are at higher risk of venous thromboembolism. Patients with these clinical findings at admission may require measures for more aggressive surveillance for the presence of venous thromboembolism. Patients with venous thromboembolism had an increased length of stay in rehabilitation, but ultimately did not have significant differences in FIM score changes.
Key words: venous thromboembolism; inpatient rehabilitation; cancer; complications; treatment.
Accepted Aug 8, 2017; Epub ahead of print Sep 20, 2017
J Rehabil Med 2017; 49: 00–00
Correspondence address: Amy Ng, Department of Palliative Care and Rehabilitation Medicine, Unit 1414, University of Texas, MD Anderson Cancer Center, 1515 Holcombe Boulevard, Houston, TX 77030, USA. E-mail: ang@mdanderson.org
Venous thromboembolism (VTE) prophylaxis and treatment in cancer patients presents a major challenge in daily practice. Cancer patients have a wide array of comorbidities, and several national and international guidelines have been published for the treatment and prophylaxis of VTE in these patients (1). Cancer-associated VTE is prevalent, with the rate increasing by 28% from 1995 to 2003, with an overall VTE incident rate of 4.1%, with 3.4% deep vein thrombosis (DVT) and 1.1% pulmonary embolism (PE), in a recent analysis of 1,000,000 hospitalized cancer patients (2). Patients with cancer-associated VTE worldwide have significantly worse survival (3, 4) and experience more complications of bleeding rate and recurrent VTE (4, 5). In cancer patients, there is a 4–7-fold increase in the frequency of VTE during treatment compared with patients without cancer (6).
Current guidelines from the American Society of Clinical Oncology, the National Comprehensive Cancer Network, the American College of Chest Physicians, and the European Society of Medical Oncology all recommend the use of usual prophylactic doses of low molecular weight heparins for patients with cancer who require hospitalization for acute medical illness in the absence of bleeding or other contraindications to anticoagulation (7–9). The high incidence of VTE and associated complications among cancer patients highlights the need to establish a systematic approach to prevention and treatment. Until very recently, there has been no analysis of risk-benefit ratio for prophylaxis in hospitalized cancer patients (10). This is a particularly difficult population to treat, as these patients often have other medical comorbidities and have contraindications to anticoagulation treatment, such as thrombocytopaenia, coagulopathy and metastatic disease with high risk of bleeding. Currently there are no well-established guidelines in place for prophylactic anticoagulation recommendations for cancer patients undergoing inpatient acute rehabilitation.
There has been a considerable amount of research in a variety of inpatient rehabilitation populations, including general rehabilitation (11–13), post-orthopaedic surgery (14, 15), spinal cord injury (16–18), general neurology (19, 20), traumatic brain injury (21, 22), stroke (23), and cardiac (24–26) rehabilitation inpatients. To our knowledge, there are no studies of VTE in cancer rehabilitation inpatients.
Cancer rehabilitation inpatients have a number of risk factors that could make them particularly at risk of VTE, including reduced mobility and malignancy-related hypercoagulability. The aim of this study was to determine the frequency of VTE in cancer patients seen in the inpatient rehabilitation unit at a tertiary referral based cancer centre, and to determine if any patient characteristics or predictors exist in patients who develop VTE. This study also sought to determine if there is any impact on Functional Independence Measure (FIM) scores, FIM efficiency, and length of stay (LOS) for those rehabilitation inpatients developing VTE.
After obtaining institutional review board approval, a retrospective chart review was conducted of patients admitted to the
acute inpatient rehabilitation unit from September 2011 to June 2013.
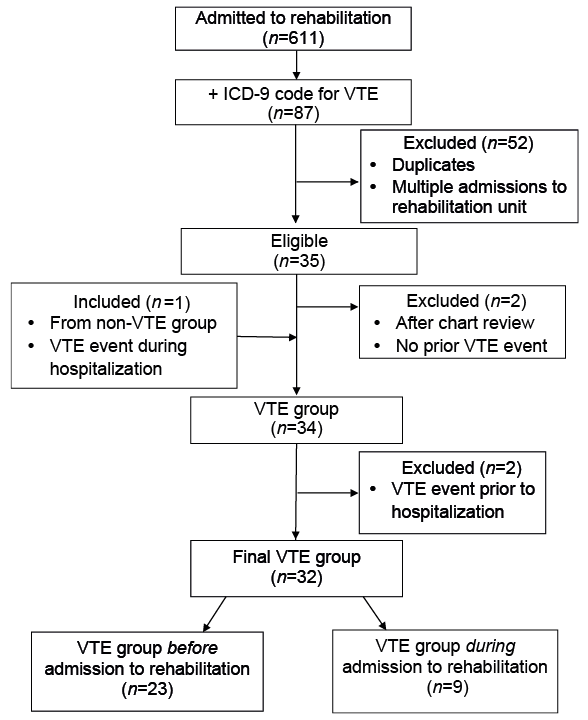
Fig. 1 summarizes the derivation of the VTE group using International Classification of Diseases (ICD)-9 codes: 38.7 inferior vena cava (IVC), plication of vena cava; 415.1 (PE); and 453.6, 453.4, 453.41 (DVT) were searched amongst the billing database used by the physiatrists and haematologists at our institution during admission to rehabilitation. Duplicate medical records were found when a patient returned to the primary oncology service due to acute complications before completion of acute rehabilitation and was later readmitted to rehabilitation to re-start and complete their rehabilitation. In these cases, both admission and discharge FIM scores of the second and complete admission to rehabilitation were used. A total of 32 patients had a VTE event, 9 patients had the VTE event during inpatient rehabilitation admission and 23 patients with VTE during the hospitalization course but before admission to rehabilitation (Fig. 1). A control group with no VTE (non-VTE) events was included in this study for comparison.
Fig. 1. Derivation of study sample: venous thromboembolism (VTE) group. ICD: International Classification of Diseases.
Fig. 2 illustrates the derivation of the non-VTE group. The non-VTE group was chosen randomly from the same set of admitted patients (n = 611) in the inpatient unit during the same time frame, who did not develop VTE during their hospital stay (n = 577). The non-VTE group was chosen to have twice the number of VTE patients identified. The decision to select twice the number of VTE patients was made based both on the practical (workload) consideration of an abundance of non-VTE patients and the desire for a reasonable precision of estimation.
Fig. 2. Derivation of study sample: non-venous thromboembolism (VTE) group. ICD: International Classification of Diseases.
This method provides a fair non-VTE group sample without making it impossible to complete the study. Further chart review of the 68 patients in the non-VTE group found that 8 patients had a VTE event that occurred prior to hospitalization with admission to rehabilitation. These patients were already under treatment or prophylaxis and, as such, could not be considered as part of the true control or the VTE group. One additional person was found to have a VTE during the hospitalization period and was moved into the VTE group before admission to rehabilitation, as the event occurred during hospitalization, but was not identified using the ICD-9 codes. The final non-VTE group consisted of 59 patients who did not have a VTE event.
Data were collected and analysed for any association between VTE frequency and possible predictors, including demogra-phic information, rehabilitation stay characteristics, functional information (FIM scores at admission and discharge), symptom information (pain, fatigue, lower extremity oedema, dyspnoea), and presence of anticoagulation.
Demographic information included age, sex, race, and cancer diagnosis. Rehabilitation stay characteristics included LOS in the rehabilitation unit, presence of Foley catheter at time of admission to rehabilitation, and disposition after rehabilitation to a Skilled Nursing Facility (SNF) or home. The total LOS in the hospital (including acute medical days prior to admission to rehabilitation unit and rehabilitation days) were also collected. Rehabilitation factors for patients who had a Foley catheter, disposition to SNF instead of home and increased LOS were hypothesized to be associated with more debility and therefore analysed in this study.
Functional and symptom information included FIM scores, pain and fatigue scores (rated by the patient as score 0–10, with zero being no pain and 10 being the most pain), and presence of lower extremity oedema as documented in clinical examination by a physiatrist. The FIM instrument provides a uniform system of measurement for disability based on the International Classification of Impairment, Disabilities and Handicaps. The FIM instrument uses an ordinal scale to rate the level of assistance required in the performance of activities of daily living (ADL) and mobility tasks, with a score of 1 for total assistance and 7 for complete independence. The 2 main dimensions in FIM include motor tasks and cognitive tasks. The motor tasks include: eating, dressing, bathing, dressing upper body, dressing lower body, toileting, bladder, bowel and 3 transfer functions (transfers into and out of bed/wheelchair, transfers onto and off toilet, transfers into and out of bathtub), and locomotion gait and stairs. The cognitive dimensions include 5 tasks: cognitive comprehension, expression, social interaction, problem-solving, and memory. We specifically aimed at determining the impact of FIM transfer scores as it may be of great value in determining burden on caregivers and even ability to receive further treatment.
Pain and fatigue scores were recorded based on subjective measurement of patients on admission and discharge, with the highest number rated recorded. If no scores were available on the day of admission or discharge, the previous day was used.
Data regarding the risk and treatment of VTE included anticoagulation treatment, anticoagulation prophylaxis (low molecular weight heparin, aspirin, warfarin, heparin), statin use, clinician-assessed lower extremity oedema at the time of admission to rehabilitation, and clinician-assessed oxygen dependence as measured by oxygen (O2) use at admission (on the day before and day of admission to rehabilitation).
Patient demographic and clinical characteristics, and FIM efficiency score [(discharge FIM score – admission FIM score)/LOS in days] are summarized and compared between patients who developed VTE after being hospitalized but before admission to rehabilitation, those who developed VTE after admission to rehabilitation and who did not develop VTE during hospitalization. Comparisons of continuous variables between the 2 groups were performed using a Wilcoxon rank sum test. The differences in categorical variables between the 2 groups were determine with Fisher’s exact test or χ2 test. All computations were carried out in SAS 9.3 (SAS Institute Inc., Cary, NC, USA).
Demographic variables for 91 patients (VTE before rehabilitation (n = 23), VTE during admission to rehabilitation (n = 9) and 59 controls) are summarized in Table I using descriptive statistics. No statistical significance was found between each of the VTE groups and non-VTE group in terms of sex, race, tumour type, and risk groups. No statistical significance was found between VTE frequency and possible predictors, such as fatigue, pain, oxygen use or statin use.
Table I. Demographic variables
Table II shows that patients who developed VTE while in rehabilitation were slightly younger than those who did not develop VTE (50 vs 61 years old, p = 0.04) and had a longer LOS in acute inpatient rehabilitation (20.3 vs 11.2 days, p < 0.001). The total LOS in hospital (acute medical and inpatient rehabilitation stay) for those who developed VTE during rehabilitation was 30.8 vs 24.2 days, but this was not statistically significant (p = 0.06).
Table II. Main findings: venous thromboembolism groups vs non-VTE group
Patients who developed VTE during admission to rehabilitation were younger and had longer LOS for rehabilitation as well as overall LOS while hospitalized compared with those who did not develop VTE.
Of patients who developed VTE during rehabilitation, 50% had oedema at admission, whereas only 12.1% of patients who did not develop VTE during rehabilitation had oedema at admission (p = 0.02, Table III).
Table III. Presence of prophylaxis and lower extremity oedema at admission
All FIM scores at admission and discharge were analysed. The FIM transfer score at admission to rehabilitation was found to be significantly lower in the group that developed VTE vs non-VTE (mean ± standard deviation: 3.7 ± 0.9 vs 4.4 ± 0.7, p = 0.02; Table IV). FIM transfer efficiency (discharge FIM transfer score – admission FIM transfer score/LOS in days) was also found to be significantly lower in those who developed VTE compared with the non-VTE group (0.04 + 0.04 vs 0.1 ± 0.1, p < 0.05). The FIM transfer score at admission is an important factor to consider when physiatrists are determining the level of debility, and these results showed that the non-VTE group needed less help (higher FIM transfer and higher FIM transfer efficiency score) compared with the group with VTE during rehabilitation.
Table IV. Functional Independence Measure (FIM) transfer scores
The VTE before admission to rehabilitation group comprised 23 patients who were found to have a VTE event during their hospitalization but before admission to rehabilitation. There were no statistically significant findings between the group who developed VTE before admission to rehabilitation vs the non-VTE group in terms of female sex (35% vs 39%, p = 0.72), race (p = 0.67), high risk cancers (p = 0.85), primary cancer type (p = 0.32), age (66 vs 61 years, p=0.82), LOS in rehabilitation (13.2 vs 11.2 days, p = 0.13), or LOS overall hospitalization (28.7 vs 24.2 days, p = 0.08) as seen in Tables I and II.
Among patients who experienced VTE before admission to rehabilitation, 3 out of 23 (13%) were on prophylaxis during their hospital stay, compared with the non-VTE group, in which 37 out of 56 (66%) were on prophylaxis (p < 0.001) (see Table III). Among patients in the the VTE group during admission to rehabilitation there was no difference seen in prophylaxis use between patients who developed and did not develop VTE (56% for the VTE group vs 66% for the non-VTE group, p = 0.71) (see Table III).
On admission to rehabilitation, of the 21 patients who developed VTE prior to admission, 11 (52%) had lower extremity oedema, compared with 7 patients (12%) in the non-VTE group (p = 0.0002).
This study found that 5.6% of inpatient cancer rehabilitation patients from September 2011 to June 2013 had a VTE event. Similar literature on cancer inpatients showed frequencies of 4.1–7.8% (6).
VTE is newly diagnosed in an estimated 300,000–600,000 people annually in the USA (27). Approximately one-third of hospitalized patients are at risk of VTE (28). A literature review using discharge data for Medicare claims from 1988 to 1990 found that the rate of VTE was 0.6%. More recent studies show a VTE incidence of 7.8% over 26 months (29, 30). The National Hospital Discharge Survey, conducted from 1979 to 2000, showed a rate of 2% for DVT and 1% for PE. Patients with additional risk factors, such as cancer, are at higher risk of development of DVT and its associated complications. The increased incidence is thought to be due to increased awareness and increased use of diagnostic procedures (11, 14).
In a study by Khorana et al. (2) of hospitalized cancer patients, other demographics, including age older than 65 years, female sex, black race, currently being on chemotherapy and having high-risk cancers were determined to have a higher correlation with VTE. These high-risk cancer sites were: brain, pancreas, kidney, ovarian, lung, stomach, and haematological/myeloma, non-Hodgkin’s lymphoma, and Hodgkin’s lymphoma (2, 31). Our study did not demonstrate an association between a VTE event and high-risk cancers (Table I), although our study had only a limited sample size of 32 and we studied only those patients referred to inpatient rehabilitation.
In a study of post-operative patients who had received prophylaxis with an antithrombotic agent, the risk of developing PE in association with DVT was 8%, compared with 42% who were not on prophylaxis (32). In high-risk patients, early identification of VTE and initiation of treatment could prevent further morbidity and mortality. The current study did not indicate embolization occurrence with anticoagulation treatment or IVC filter placement and VTE identification and treatment allowed for early mobility without further loss of rehabilitation days due to bed rest.
Patients with VTE in this study were found to have an increased rehabilitation LOS compared with those without a VTE event. This might be a result of diagnosis, consultations and management of the initial VTE, or VTE might simply be a marker for a patient with a more complex clinical course. The design of the current study does not allow us to determine the 2 explanations, therefore, further prospective studies are needed to better characterize the association between VTE and the increased LOS.
Patients who had lower extremity oedema at the time of admission to rehabilitation were found to have a higher chance of developing a VTE event during the course of rehabilitation, compared with patients who did not have oedema. In 9 patients who developed VTE, 50% had LE oedema at baseline, whereas in 59 patients who never had VTE, only 12% had LE oedema at baseline (p = 0.02, Table III). This finding emphasizes the importance of physical examination, as asymmetrical lower extremity oedema may be one of the earliest indicators of presence of a VTE event (33). The presence of asymmetrical lower extremity oedema at admission to inpatient rehabilitation or any hospital admission may warrant further work-up of the swollen extremity for the presence of VTE.
Mobility, as evidenced by higher FIM transfer scores at admission to the inpatient rehabilitation unit in our study, showed a decreased risk of VTE development during the course of hospitalization.
In the group of 68 controls, one patient was found to have developed a VTE event before admission to rehabilitation, and this patient was included as part of the VTE group before admission to rehabilitation. One limitation is due to the coding of VTE diagnosis; it is possible that more patients developed VTE, especially during the time period before admission to rehabilitation, as their diagnosis was coded prior to rehabilitation. However, it is reassuring that, although 68 cases in the non-VTE group were reviewed carefully, only one case was found to have VTE. Therefore, the frequency is likely to be close to what we observed in this study. Prospective studies are needed to better determine the frequency and clinical course of VTE.
Although we found that the presence of prophylactic anticoagulation in our study was also associated with a lower risk of VTE event throughout hospitalization, our analysis was limited as we evaluated only the use of pharmacological prophylaxis (heparin, warfarin, low molecular weight heparin, aspirin) at the time of admission. This study did not examine the use of sequential compression devices/thromboembolic disease hose or include IVC filter as a form of prophylaxis for VTE.
This was a retrospective study at a dedicated cancer hospital and, due to the parameters of systems practice, may have inherent bias regarding data compared with more general settings in which oncology care is delivered.
The presence of lower extremity oedema, absence of prophylactic anticoagulation, and lower FIM transfer score at admission were found to increase the odds of a VTE event. Patients with these clinical findings may require measures for more aggressive surveillance for presence of VTE. These results should be considered as a pilot study and, prospectively, large population groups should be used to confirm the results.
Due to increased awareness of VTE prevention and the debate regarding performing routine screening prior to admission to rehabilitation units across the USA, it has not been easy to identify a consensus approach to prevention, diagnosis and treatment of VTE events. This study highlights cancer patients at high risk of a VTE event. Those patients who were identified and mobilized did not undergo further embolization into pulmonary embolism or mortality. Due to the special nature of cancer patients undergoing acute inpatient rehabilitation, management of VTE events is often complex. Prevention and treatment need to be tailored to the individual.
This study is supported in part by the National Institutes of Health (NIH) M.D. Anderson Cancer Center Support Grant # CA 016672. Eduardo Bruera is supported in part by NIH grants RO1NR010162-01A1,RO1CA122292-01, and RO1CA124481-01.
The authors declare no conflicts of interest.


 Click to show fullsize
Click to show fullsize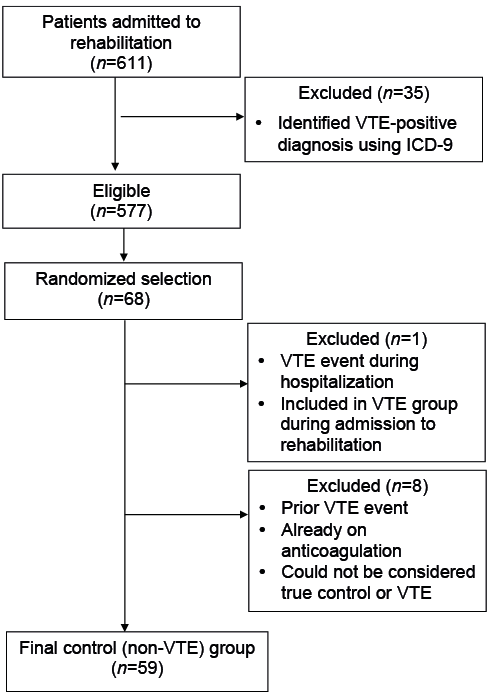 Click to show fullsize
Click to show fullsize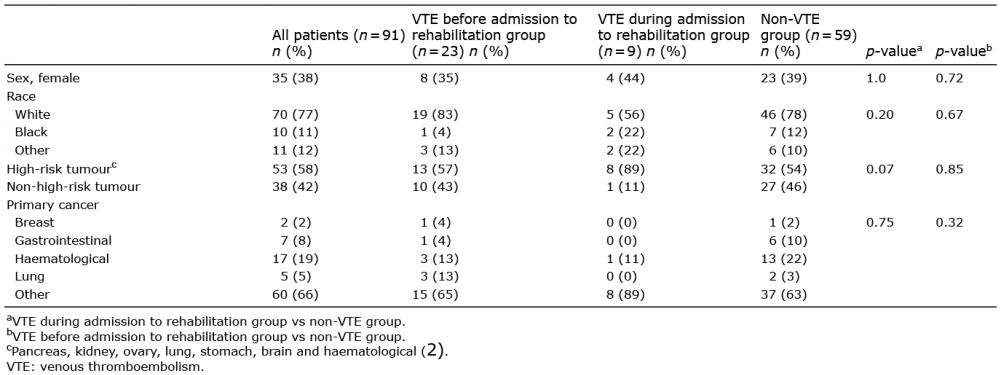 Click to show fullsize
Click to show fullsize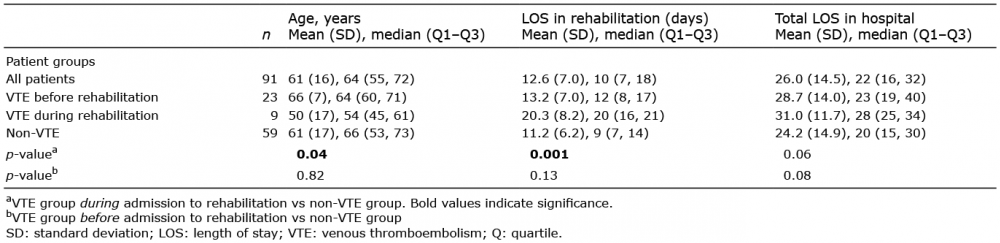 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize