
From the 1Department of Rehabilitation, Neurorehabilitation Unit, HABILITA Care and Research Rehabilitation Hospitals, Zingonia di Ciserano, Bergamo, 2Department of Rehabilitation Medicine, Severe Acquired Brain and Spinal Cord Injuries Rehabilitation Unit, Ulss 9 Ca’ Foncello Hospital,Treviso, 3Unit of Anesthesia and Intensive Care B-DEA, S. G. Bosco Hospital, Turin, 4Physical Medicine and Rehabilitation, Neurorehabilitation Unit, IRCCS Casa Sollievo della Sofferenza, San Giovanni Rotondo (FG), 5Unit of Biostatistics IRCCS Casa Sollievo della Sofferenza, San Giovanni Rotondo (FG), 6SSD Severe Acquired Brain Injury Unit – S. Giovanni Battista Hospital, Foligno (PG), 7Department of Rehabilitation Medicine, S. Gerardo Hospital, Monza, Italy and Intensive Care and Neurorehabilitation Italian Study Group authors (see Appendix SI)
Objective: To determine whether early mobilization of patients with severe acquired brain injury, performed in the intensive/neurointensive care unit, influences functional outcome.
Design: Prospective observational study.
Setting: Fourteen centres in Italy.
Subjects: A total of 103 consecutive patients with acquired brain injury.
Methods: Clinical, neurological and functional data, including the Glasgow Coma Scale (GCS), Disability Rating Scale (DRS), the Rancho Los Amigos Levels of Cognitive Functioning (LCF), Early Rehabilitation Barthel Index (ERBI), Glasgow Outcome Scale (GOS), and Functional Independence Measure (FIM) were collected at admission and every 3–5 days until discharge from the intensive/neurointensive care unit. Patients were divided into mobilization and no mobilization groups, depending on whether they received mobilization. Data were analysed by intragroup and intergroup analysis using a multilevel regression model.
Results: Sixty-eight patients were included in the mobilization group. At discharge, both groups showed significant improvements in GCS, DRS, LCF and ERBI scores. The mobilization group showed significantly better improvements in FIM cognitive, GOS and ERBI. The patients in the mobilization group stayed longer in the intensive care unit (p = 0.01) and were more likely to be discharged to intensive rehabilitation at a significantly higher rate (p = 0.002) than patients in the no mobilization group. No adverse events were reported in either group.
Conclusion: Early mobilization appears to favour the clinical and functional recovery of patients with severe acquired brain injury in the intensive care unit.
Key words: intensive care; mobilization; neurorehabilitation; rehabilitation; acquired brain injury.
Accepted Jul 4, 2017; Epub ahead of print Oct 5, 2017
J Rehabil Med 2017; 49: 00–00
Correspondence address: Michelangelo Bartolo, Department of Rehabilitation, Neurorehabilitation Unit, HABILITA Care and Research Rehabilitation Hospitals, Zingonia di Ciserano, Bergamo, Italy. E-mail: michelangelobartolo@habilita.it
Intensive care unit (ICU) patients may develop complications due to prolonged immobilization, such as cardiovascular system damage and critical illness neuromuscular syndromes (1), which are associated with poor short-term outcomes, including a delay in ventilator weaning and ICU/hospital discharge (2, 3).
Early mobilization might counterbalance these effects, by maintaining muscle strength, improving functional outcome, sedation levels and patients’ quality of life in the ICU and beyond (4–6). Although early physical rehabilitation, including mobilization of critically ill patients, was considered unsafe a few years ago, in the last decade a growing body of literature has shown the safety and feasibility of mobilizing ICU patients to prevent impairments and functional limitations (5, 7, 8). A number of studies have shown that early rehabilitation is effective, especially if mobilization is implemented within a structured protocol (9) and is based on procedures with proven feasibility and safety. Therefore, early mobilization has been included as a component of the ABCDE bundle (Awaken from sedation, Breathe independently of the ventilator, Choice of sedation, Delirium management, Early mobilization) (8, 10) and recent studies have confirmed its important role/effect (11).
However, evidence supporting early mobilization is based mainly on trials performed in general medical and surgical ICUs, while studies conducted in neurological ICU (NICU) settings are sparse and show conflicting results. Indeed, a bidirectional case-control study showed that early mobilization and sitting upright could be favourable for patients admitted to NICUs (12), whereas a prospective intervention trial and a comparative study revealed that early rehabilitation in patients with severe acquired brain injury (sABI) might lead to a shorter length of hospital stay (LOS), fewer restraint days, and fewer hospital-acquired infections (13, 14). On the other hand, a recent retrospective chart review conducted during a 6-month pre-mobilization and 6-month post-mobilization period concluded that, despite an increase in the amount of physical therapy and occupational therapy, no change in hospital and ICU LOS or duration of mechanical ventilation was observed (15).
Overall, the lack of available evidence underlines that there is still much research to be done into early rehabilitation for sABI patients in the ICU and there are specific questions to be answered regarding the timing of intervention, the intensity and type of exercises, and which professionals should be involved (e.g. physiotherapist, occupational therapist, nurse) (16).
The aim of the current study was to evaluate whether early mobilization influences the functional outcome of patients with sABI, through further analysis of data collected during a previous multicentre observational study (17).
Fourteen centres in Italy with neurorehabilitation units and an ICU/NICU participated in the study (7 in the north of Italy, 3 in the south, 2 in the centre, and 2 in the islands).
Patients admitted to the ICU from 1 January to 31 December 2014, with a diagnosis of sABI were enrolled in the study. Each participating centre was asked to enrol at least 10 patients.
sABI was defined as central nervous system (CNS) damage due to acute traumatic or non-traumatic (vascular, anoxic, neoplastic or infectious) causes that led to a variably prolonged state of coma (Glasgow Coma Scale ≤8), producing a potentially wide range of impairments affecting physical, cognitive and/or psychological functioning (18–22).
Subjects with premorbid CNS-related disability, neurological diseases, or neoplastic disease with metastatic involvement of the CNS were excluded.
Immediate relatives or legal guardians of the patients provided informed consent to participate in the study. The study was conducted in accordance with the revised version of the Declaration of Helsinki and was approved by the local ethics committee of the coordinator centre and approval was extended to all centres taking part in the study.
Data in the present study were collected as part of routine care during a previous prospective, observational, multicentre study by our working group (17). As the study was observational, no criteria to decide readiness to mobilize were provided: it was only recorded when mobilization was performed. At the end of the study, the baseline clinical features and the outcomes of the patients who received mobilization (MOB) and who were not mobilized (NoMOB) were compared in order to understand which criteria are used by clinicians to mobilize (or not mobilize) the patients. The methodology has been described previously in detail (17).
On admission all the enrolled patients underwent a complete clinical, neurological and functional examination. All patients were re-evaluated every 3–5 days (at least twice per week) until discharge from the ICU. Clinical and rehabilitative data were collected.
The following rehabilitative data were collected: duration, type and timing of rehabilitative sessions, postural changes (performed at least 6–8 times/day), early passive/active-assisted mobilization, respiratory rehabilitation, bronchial drainage, removal of tracheostomy tube, sitting posture and orthostatic reconditioning, gait rehabilitation, swallowing evaluation, speech therapy, responsiveness, multisensory stimulation, caregiver education and psychological support, and team meetings with caregivers. The researcher who collected the data specified whether each procedure was performed.
For the aims of this work, early passive/active-assisted mobilization was defined as movement against gravity involving axial loading of the spine and/or long bones, also including the following activities: (i) sitting over the edge of the bed, (ii) sitting on a chair, (iii) use of a tilt bed/table to ≥40°. Physical and/or mechanical assistance was permitted in order to complete these activities. A session of mobilization was defined as a single continuous period of mobilization with a period of bed-rest either side of that session.
In order to provide a multidimensional assessment of the patients’ clinical and functional status the following measures were used: Glasgow Coma Scale (GCS), Disability Rating Scale (DRS), the Rancho Los Amigos Levels of Cognitive Functioning Scale (LCF), Early Rehabilitation Barthel Index (ERBI), Glasgow Outcome scale (GOS) and Functional Independence Measure (FIM).
All measurements were administered at each visit, except for ERBI, which was administered at admission and at discharge, and GOS and FIM, which were administered only at discharge. All adverse events were recorded.
Patient characteristics were reported as means ± standard deviations (SD) and medians (together with first and third quartiles) or frequencies and percentages, for continuous and categorical variables, respectively. For each continuous variable, the assumption of normal distribution was checked by means of the Shapiro-Wilk test along with quantile-quantile (Q-Q) plots. Comparisons between the MOB and NoMOB groups were assessed using the Mann–Whitney U test (because of deviation from normal distribution) or the Fisher’s exact test, as appropriate for continuous and categorical variables, respectively.
To test changes in GCS, DRS and LCF scores at different (and unequally spaced) follow-up times from the first evaluation to discharge, hierarchical generalized linear models (HGLMs) for longitudinal data were fitted for each outcome. Within this framework, the Poisson distribution for the error term was assumed to model each functional score. A random intercept was included in each model to account for clustering due to centres (i.e. multicentre design effect). As measurements were collected at different times, a spatial-power covariance structure (which handles individuals’ unequally spaced follow-up times), was assumed within each longitudinal model (23). To test changes in ERBI measurements at the first and last evaluations, a HGLM was performed on ERBI rank values, assuming normal distribution for the error term. Such models included an indicator variable, which specifies whether patients received mobilization (i.e. MOB group), a time variable, which specifies each measurement (within each patient), and a group-by-time interaction variable. Specifically, to test whether the outcome means were different (during the follow-up) in all patients, we examined the statistical significance of the time variable, whereas to test whether such means were different within each group, we examined the statistical significance of suitable statistical contrasts defined within the models. Moreover, pairwise comparisons between means were also estimated and p-values were adjusted for multiple comparisons following the Benjamini–Hochberg procedure. Another statistical contrast was properly assessed to evaluate whether there was a difference between group means at first evaluation (i.e. baseline) only. The significance of the group-by-time interaction variable suggested whether the outcome mean profiles (i.e. means collected over time) were different between the 2 MOB groups. The time variable was included into HGLMs, both as categorical and continuous. In the first case, a test for overall difference between means over time was assessed by examining the significance of the Type III test, whereas in the second case, a test for linear trend was assessed by examining the significance of the slope of the time variable. To make valid inference for each statistical test derived from HGLMs, degrees of freedom were corrected following Kenward-Roger approximation. Estimated means were carried out from HGLMs and were reported along with their 95% confidence interval (95% CI). For the ERBI outcome only, observed medians along with first-third quartiles) were reported instead. Furthermore, longitudinal plots of the estimated functional outcomes over time were separately reported for each MOB group at issue, along with error bars, which represented 95% CI. Two-sided p-values < 0.05 were considered for statistical significance. All analyses were performed using SAS Software, Release 9.4 (SAS Institute, Cary, NC, USA) and R (package: ggplot2).
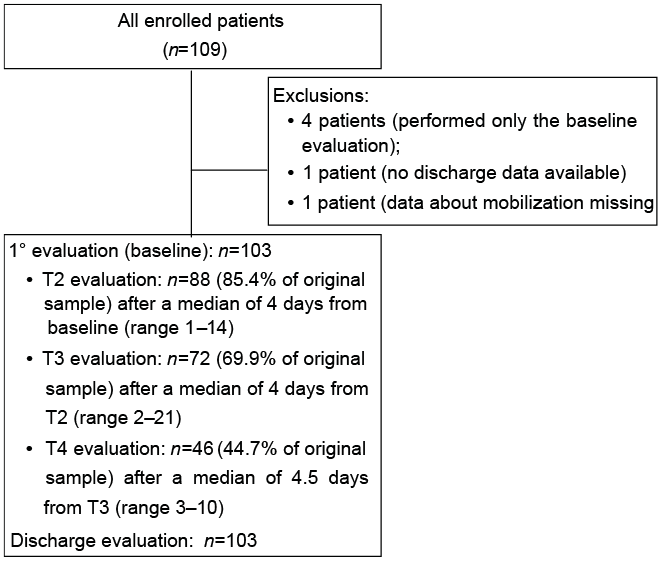
The study enrolled 109 consecutive patients diagnosed with sABI. Six patients were excluded due to missing data; therefore the study sample comprised 103 subjects. Participant enrolment and flow through the study are summarized in Fig. 1.
Fig. 1. Flow diagram of the study.
Among the total sample, 68 patients (66%) received the intervention (MOB group). Baseline demographic and clinical characteristics, aetiology, side and extension of cerebral lesions and comorbidities of the total sample, as well as of the MOB and NoMOB groups, are summarized in Table I.
Table I. Demographic and clinical characteristics of patients with severe acquired brain injury (sABI) at hospital admission (overall and by mobilization status)
For most patients mobilization was performed by a physiotherapist (98%), while in one case a nurse performed the mobilization.
The mean LOS in the ICU was 24 days (standard deviation (SD) 14.1 days) for the total sample, with a significant difference (p = 0.01) between the MOB group (26.2 (SD) 13.7 days) and NoMOB group (19.5 (SD) 14.2 days).
Data for patients’ functional status at admission and discharge are shown in Table II.
Table II. Functional measures at admission and discharge in patients with severe acquired brain injury (sABI) (overall and by mobilization status)
At admission the between-group analysis showed that the NoMOB group had a significantly more severe clinical and functional profile than the MOB group with regard to all measurements, except for the ERBI scale. Longitudinal analysis revealed a statistically significant improvement in patients’ clinical and functional conditions in both groups, when comparing admission-discharge values of GCS and LCF scores. Moreover, comparison within the group revealed that the MOB group showed significant improvement in DRS and ERBI scores, while the NoMOB group showed a trend towards improvement for these measures without reaching statistical significance (Table II).
Comparison between groups at discharge showed statistical significance only for the ERBI, in favour of the MOB group (Table II). At discharge, the comparison of FIM scores between the MOB and NoMOB groups revealed a statistically significant difference only for the sub-score of FIM cognitive: 7 (95% CI 5; 14) vs 5 (95% CI 5; 8.75) (p = 0.04); however, the difference was not statistically significant for the total score: 21 (95% CI 18; 27) vs 18 (95% CI 18; 21.75) and for the motor subscores 13 (95% CI 13; 15.25) vs 13 (95% CI 13; 13).
With regard to the GOS score, the difference between the MOB group (3 (95% CI 3; 3)) and the NoMOB group (2 (95% CI 2; 3)) was statistically significant (p = 0.009).
Patients’ clinical characteristics, including limitations and need for supportive devices at discharge, were not statistically different between the 2 groups, except for the presence of pressure sores, which were significantly more frequent in the NoMOB group (Table III).
Table III. Clinical characteristics of patients with severe acquired brain injury (sABI) at hospital discharge (overall and by mobilization status)
For both groups, patients were discharged mainly to sABI rehabilitation units (30.9% and 48.6% of patients in the MOB and NoMOB groups, respectively), which, in Italy, define care settings for patients with disability due to neurological disease. At least 180 min of treatment per day is provided and patients receive care from an interdisciplinary team, often in technologically supported contexts. The percentage of subjects who were discharged to rehabilitation units was significantly higher for the MOB group (27.9%) than the NoMOB group (0%); p < 0.001. Rehabilitation units in Italy are devoted not only to neurological patients, but must ensure at least 120 min of rehabilitation treatment. Treatment by some professionals in the multidisciplinary team (e.g. psychologist, occupational therapist) is recommended but not mandatory. The other patients were discharged to acute wards, particularly to neurosurgery units (17.6% for the MOB group and 22.9% for the NoMOB group), without significant differences. All the discharge destinations are shown in Table IV.
Table IV. Discharge destinations
No adverse events were reported in either group.
The first rehabilitative clinical evaluation was performed after a mean of 7.7 (SD 6.9) days for patients in the MOB group, while patients in the NoMOB group underwent the first rehabilitative evaluation after a mean of 15.5 (SD 21.3) days from ICU admission. No statistical differences were found. Data on the rehabilitative treatments performed in both groups are summarized in Table V. At discharge, the mean number of sessions of mobilization, speech therapy and psychology was 10 (SD 7.7), 0.8 (SD 2.5) and 0.4 (SD 1.3), respectively, for the MOB group. The mean number of missed sessions did not reach 1%, considering both clinical and organizational causes. No sessions were recorded for the NoMOB group.
Table V. Rehabilitation treatments: intergroup comparison
Data from this study show that early mobilization seems to favour clinical and functional recovery in ICU patients with sABI; however, only two-thirds of patients received mobilization and this started one week after ICU admission. These results are consistent with data from non-neurological populations, revealing that early mobilization of patients receiving mechanical ventilation is still uncommon, despite the recent publication of consensus recommendations regarding safety criteria for mobilization of adult, mechanically ventilated ICU patients (24).
Baseline comparison between MOB and NoMOB groups in our sample provided guidance regarding the criteria commonly used by clinicians to decide patients’ readiness to be mobilized. Approximately one-third of patients were considered unsuitable to start mobilization, perhaps because they were deemed clinically “too serious” by physicians. This raises the question of whether this attitude is supported by evidence or driven by fear among healthcare providers. The literature indicates that the main obstacles in early rehabilitation are: (i) the clinical severity of patients, considered “too sick” to engage in physical activities; (ii) the presence of indwelling lines and tubes (endotracheal tubes, central venous catheters, arterial lines, bladder catheters) that restricted movement; (iii) sedation that made patients too sleepy to be involved in treatment (25); and (iv) the presence of femoral vascular access and mechanical ventilation (26, 27). Moreover, although less represented, the lack of professional resources and poor experience in delivering rehabilitative care to ICU patients have also been described (27, 28). On this issue, it has been shown recently that staff education alone was ineffective at improving mobility outcomes for ICU patients, suggesting that educative approaches should be integrated with other factors, such as a change in sedation practice and increase in staffing (28). In our sample, the main factors associated with early mobilization were: (i) patients’ level of consciousness and cognitive functioning; and (ii) comorbidities. In fact, only patients who exhibited at least minimal reactions to the environment and presented with fewer comorbidities underwent mobilization. In our opinion, the reasons to perform early mobilization are not clear to all operators: in general medical and surgical ICU it is easier to understand that mobilization can favour a faster motor recovery that can be observed during the ICU stay, while for patients with sABI, who are often unconscious or sedated, the benefits of the intervention may be less evident. However, the prejudicial exclusion of comatose patients could not be justified. Indeed, comatose subjects might also benefit from rehabilitation and obtain functional improvement. The achievement of this objective is essential, since ICU patients who improve their functional status during the ICU stay have a reduced risk of 90-day mortality following hospital discharge (29).
When considering neurological patients, most clinicians have concerns in relation to the early mobilization of severe stroke patients, especially after a haemorrhagic event (30). With regard to aneurysmal subarachnoid haemorrhage (SAH), some observational studies have found the highest risk period for re-bleeding is between 2 and 4 weeks after the initial aneurysmal SAH. Consequently, in order to avoid re-bleeding, especially for patients who have not had, or could not have, surgical or endovascular treatment for the aneurysm, bed-rest for 4–6 weeks is often included as a component of the treatment strategy (31, 32). Conversely, in patients with SAH, the feasibility and safety of arterial and intracranial pressure of an early rehabilitation programme was focused on functional training and therapeutic exercise in more progressively upright positions (33, 34). How
ever, a recent Cochrane systematic review concluded that no randomized controlled trails or controlled trials were available to provide evidence for or against staying in bed for at least 4 weeks after symptom onset, and suggested further research to clarify optimal periods of bed-rest for these patients (32). A recent retrospective study that analysed the outcome of 143 ICU-dependent, tracheotomized, and mechanically ventilated patients with both ischaemic and haemorrhagic cerebrovascular disease (CVD), concluded that, as mortality rates of early rehabilitation in CVD are low, in-patient rehabilitation should be undertaken even in severe CVD patients to improve outcome and to prevent accommodation in long-term care facilities (35). Our findings showed that even if more than half of our patients were affected by sABI due to a haemorrhagic stroke, mobilization was probably a safe procedure; no adverse events were recorded in the MOB group and the rates of the deaths were comparable between the 2 groups. However, these data need to be confirmed in larger samples.
Our results highlight the problem of lack of homogeneity of the contents of rehabilitation in the ICU at this time. The literature suggests that rehabilitation in the ICU for sABI patients is primarily focused on respiratory therapy, passive-assistive movement for contracture prophylaxis, stimulation therapy, low-dose strength, and endurance training and stretching (36). The therapeutic goal is usually focused on the prevention of secondary damage (i.e. pneumonia or contractures), promotion of consciousness and sensory perception, and strengthening of muscles (36). Recently, an Italian Consensus Conference recommended that rehabilitation for patients with sABI in the intensive hospital phase should be more comprehensive and encompass management of respiratory problems, dysphagia, tracheostomy tube removal, cognitive disorders and language (37). However, most centres in Italy limit their rehabilitative approach to the physiotherapists’ intervention. Our data partially confirm this observation: even when patients in the MOB group also performed significantly more respiratory rehabilitation and multisensory stimulation than patients in the NoMOB group, the interventions were always performed by physiotherapists. The presence of the speech therapist was minimal and psychologists’ intervention, besides being limited in time, was devoted mainly to providing educational support to the caregivers.
Regarding the effectiveness of early mobilization, our data showed that the improvement in clinical and functional conditions in the MOB group was slightly higher than for the NoMOB group, reaching statistical significance only for ERBI values. Similar to what has been observed in medical and surgical ICUs (38), our findings suggest a methodological reflection on the available validated scales evaluating functional outcome in patients with ABI. It is likely that the measures commonly used in rehabilitation are not sensitive enough to capture the mild improvement occurring in the early phase of ICU stay. The ERBI, not commonly used in Italy, could be a reliable and valid scale to assess early neurological rehabilitation patients, as it contains highly relevant items for this population, such as mechanical ventilation, tracheostomy or dysphagia, compared with other validated clinical scales most widely used in rehabilitation. Our data showed a longer LOS in ICU for patients in the MOB group, contrary to data in the literature suggesting a shorter ICU stay for mobilized patients (13, 14). In our opinion, these results should be considered in relation to the setting where patients were sent after ICU discharge. In fact, patients with a better prognosis who received early mobilization in the ICU were discharged in a significantly higher percentage to rehabilitation units, skipping admission to sABI units where more intensive treatments based on a multidisciplinary approach are guaranteed. Unfortunately, the lack of dedicated pathways for sABI patients may induce delay in discharge from the ICU. In fact, even if clinical factors should affect rehabilitation use, several non-clinical variables play a major role in rehabilitation provision and use. In particular, the availability of rehabilitation services seems to be the major determinant of whether patients use such care and which type of rehabilitation facility they use. Moreover, across Italian regions, the criteria used to rule out access to rehabilitation units are different and often unclear, lacking clinical criteria that would identify the best setting for maximizing outcomes.
This study has some limitations. The MOB and NoMOB groups were not homogeneous, since patients were not randomly allocated to the 2 groups. On the other hand, the aim of the study was to provide a description of the procedures that were spontaneously adopted across different centres in Italy. Subsequent studies, performed as randomized trials, will provide more rigorous and controlled data to analyse the effects of mobilization in the ICU, identifying patients who would benefit more. Two additional limitations can be reported: the narrow time window (ICU LOS was a mean of 24 days (SD 14.1) and the lack of follow-up data. Evidence showed that most of the functional recovery after TBI occurs in the first 6 months after the injury, a period too long to verify the decisive results of a rehabilitation intervention occurring in the first weeks of hospitalization (39). Studies on patients with cerebral haemorrhage have shown that significant improvements (measured by means of FIM and CRS) could be detected, on average, after 11 and 9 weeks from admission to neurorehabilitation, for patients diagnosed with a vegetative state or minimally conscious states, respectively (40). This suggests that neurological outcomes should be measure over a longer time-frame than our study, and may explain why the studies on patients with sABI are performed mainly in a subsequent phase after the ICU stay, during patients’ admission to rehabilitation. Therefore, it is necessary to plan further studies including follow-up evaluations, in order to track the recovery pathway of patients with ABI from the acute phase to hospital discharge.
In conclusion, although technical difficulties and questions remain, this study provides further support to the early and progressive implementation of mobilization in the ICU for patients with sABI, and suggests that, in order to achieve widespread implementation of early rehabilitation, a shift in focus is necessary from survival to functional outcome among ICU clinicians. Finally, the study highlights several areas for future research: studies are needed addressing the timing and dosage of mobilization, as well as the association between early mobilization and patient-centred outcomes.
This project was originated within the inter-societies working group of SIRN (Italian Society of Neurological Rehabilitation), SIAARTI (Italian Society of Anesthesia, Analgesia, Resuscitation Intensive Care), and SIMFER (Italian Society of Physical Medicine and Rehabilitation), which aims at improving and promoting the culture of early rehabilitation in the ICU.


 Click to show fullsize
Click to show fullsize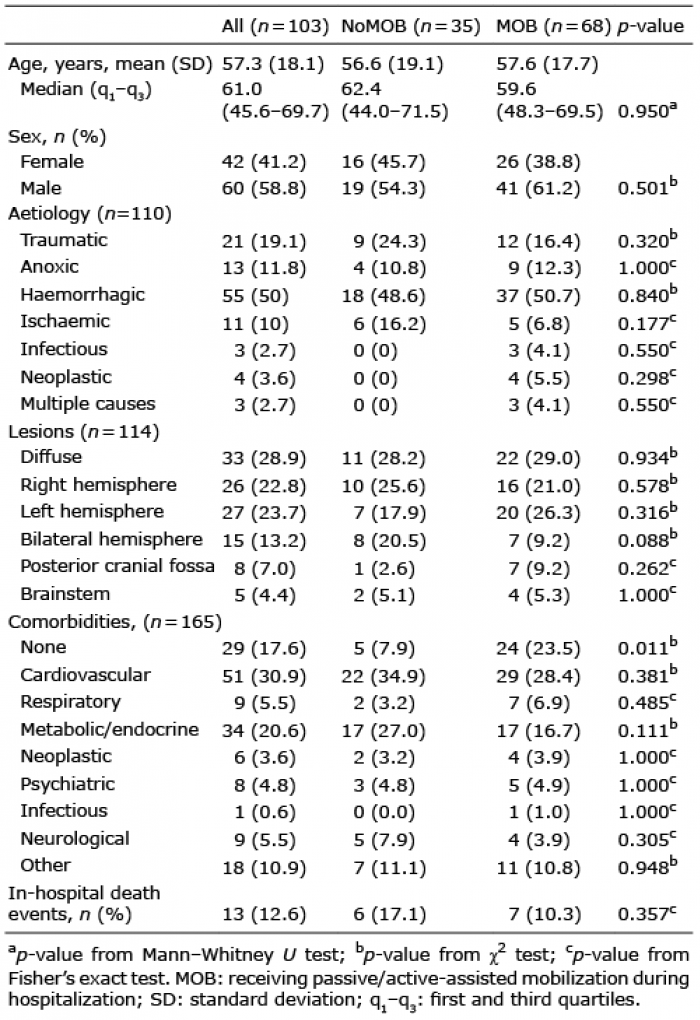 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize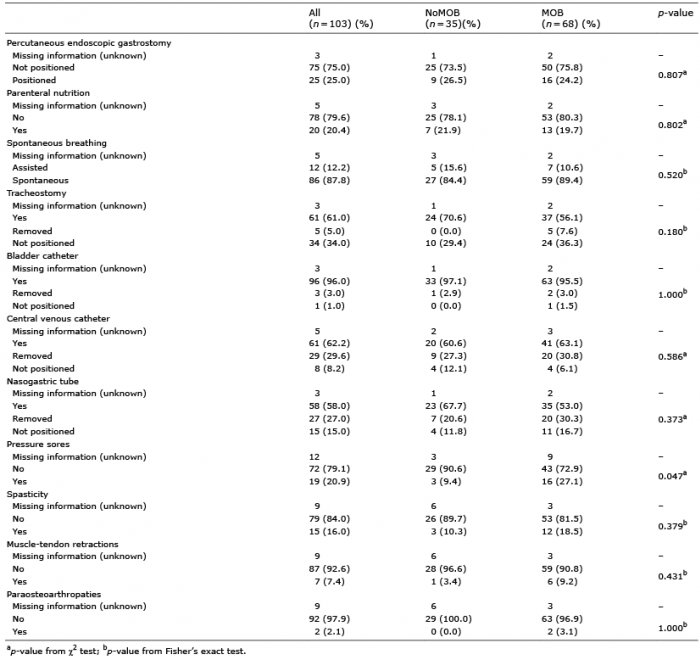 Click to show fullsize
Click to show fullsize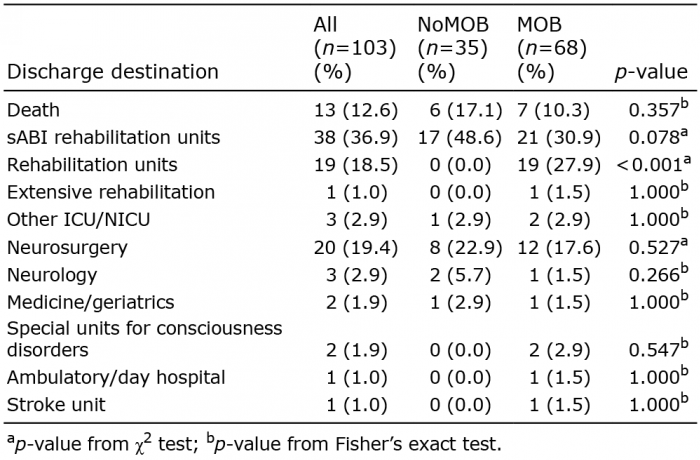 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize