
From the 1Department of Health Sciences and Health Policy, Faculty of Humanities and Social Sciences, University of Lucerne, Lucerne, and 2Swiss Paraplegic Research (SPF), Nottwil, Switzerland
Disability has a profound impact, both on those who live with it and on society that responds to the needs of people experiencing disability. Society has a primary obligation to respond to the impact of disability. Rehabilitation has an essential role to play here; but its relationship to disability embodies a broader social ambiguity about what it means to experience disability. On the one hand, disability is a mark of a minority group persons with disabilities, which has, historically, been socially disadvantaged. On the other, disability is a matter of how health conditions and associated impairments interact with the physical and social world to create limits on what people can do or become. However, just as health problems are universal over the life course, so too is disability. Everyone experiences disability. This paper explores the historical underpinnings of these two perspectives on disability, in particular how they impact on rehabilitation practice and policy. After surveying the social consequences of these perspectives, the paper attempts to reconcile them in order to enhance the overall effectiveness and relevance of the social response to disability.
Key words: disability; rehabilitation; functioning; minority model; disability advocacy.
Accepted May 11, 2017; Epub ahead of print Jun 29, 2017
J Rehabil Med 2017; 49: 543–549
Correspondence address: Gerold Stucki, Swiss Paraplegic Research (SPF), Guido A. Zäch Strasse 4, 6207, Nottwil, Switzerland. E-mail: gerold.stucki@paraplegie.ch
Disability has a profound impact, both on people who live with disability and for society that responds to their needs. For the individual with a health condition, the impairments of body function and structure they experience, in interaction with their environment, can lead to restrictions in performance of actions, tasks and social roles, both simple and complex. The person may be in pain, discomfort or experience bodily limitations in their day-to-day environment, and these may then become restrictions on what he or she can do, which may then lead to social exclusion. For society, the impact involves not only the direct social costs in terms of health and social services, but, more importantly, the opportunity costs of underutilized human resources, creativity and productivity.
It is generally agreed that a primary obligation of any society is to respond to the impact of disability. The ethical obligation to do so has perhaps been best formulated by philosopher Norman Daniels, who argued that the state, as a matter of justice, is obliged to provide its citizens with the resources they need to secure opportunities to do and become what they wish in their lives (1). States also have an obligation to remove obstacles that hinder these opportunities. Since poor health limits opportunities, an effective societal response to population health needs is required as a matter of justice. A similar argument can be made in the language of human rights: each individual is endowed with basic human rights to access essential social resources and opportunities on an equal basis (2, 3). Since 2007, these human rights have been reaffirmed specifically for persons with disabilities in the United Nations’ (UN’s) Convention on the Rights of Persons with Disabilities (CRPD) (4).
The case for society’s obligation to respond to the impact of disability can also be made in purely economic terms. Successfully addressing disability needs entails enhancing the capacity of individuals to participate fully in all domains of social life, and that invariably means contributing to the economic health of society. The social response to disability is thus an investment and not merely a cost. The potential for “returns on investment” will only increase in the future because of demographic ageing and an increased prevalence of non-communicable diseases (5).
There are a wide range of social supports and services that address disability and contribute to enhancing full participation, inclusion and fair opportunities, and, at the societal level, social and economic benefits. The range of rights in the CRPD shows that all of the agencies and institutions of the modern social state (health, social service, labour, education, transportation, communication, and others) will need to be fully engaged in order to fulfil the societal obligation to address disability.
That being said, health services will always constitute a core social response. Of all these services, those provided by the rehabilitation health strategy most directly address the two aspects of the experience of disability: problems in biological health and the intrinsic capacity to perform actions, simple to complex, and lived health, the experience of performing actions in one’s actual environment (5). Together, biological health and lived health constitute the complete lived experience of a health condition, operationalized in the World Health Organization (WHO)’s International Classification of Functioning, Disability and Health (ICF) (6) by the notion of “functioning” (7). As a health strategy, the objective of rehabilitation can therefore be understood as that of improving functioning at the body level, thereby optimizing the individual’s intrinsic capacity to perform actions and then to enhance the individual’s ability to interact with the environment through the provision of assistive technology and modifications to the immediate environment. These interventions improve the individual’s actual performance of actions, and thus his or her actual lived experience of health (8–10).
Yet rehabilitation, from its beginnings (11) has always embodied an ambiguity in how disability is understood as an experience: does disability define a class of persons, persons with disabilities, or is it a universal experience that can, and typically does, affect everyone over the course of their lives? The impact of this ambiguity on the social response to disability could be found in almost any facet of modern social services and supports designed as a response to disability. This is evident in the political advocacy of disability persons’ organizations, in debates about how best society can enhance opportunities for persons with disabilities, and even in scientific arguments over the actual prevalence of disability globally. Yet, recent developments at the WHO involving that agency’s perception of the relationship between disability and rehabilitation, will be the focus of this paper as they are emblematic of the underlying ambiguity in how we understand disability.
In 2011, the WHO published a highly influential and agenda-setting World Report on Disability, in which the focus was on the lived experience of a discrete social minority of persons; namely, persons with disabilities (12). There it is argued that persons with disabilities can be defined, not in terms of health conditions, but rather in terms of historic social disadvantage caused by attitudes and practices, ranging from fear and hostility to benign neglect. These social disadvantages are now addressed by the CRPD, which although it includes rights to health and rehabilitation services, extends far beyond this to include all social opportunities, and further still to basic values of dignity, respect, autonomy and equality. Because only a minority of individuals has been subjected to the social disadvantages associated with disability, disability identifies a specific minority group.
The World Report on Disability assembled the evidence of this social neglect, and provided recommendations that set the stage for a substantial WHO commitment to disability, in the WHO Global Disability Action Plan 2014–2021: Better health for all people with disability (13). The Action Plan explicitly identified persons with disabilities as its target group, characterized as a subpopulation of people (15% of the global population according the World Report on Disability) who “face widespread barriers to accessing services, and experience poorer health outcomes, lower education achievement, less economic participation and higher rates of poverty than people without disabilities.”
More recently, the WHO has launched another agenda-setting initiative directed specifically to rehabilitation, and the urgent worldwide need to scale up rehabilitation to address the population ageing and epidemiological trends toward increased prevalence of non-communicable diseases that will increase disability prevalence in the future. Rehabilitation 2030: A Call for Action (14) highlights the substantial and ever-increasing unmet need for rehabilitation worldwide to address this increase prevalence of disability. As the objective of rehabilitation is to optimizing functioning and minimize disability for independence, full participation, economic productivity, and meaningful life roles, rehabilitation should be at the centre of society’s response to disability. Unlike the World Report on Disability, however, this call for action points to the global need for rehabilitation services, not for some minority group, but for everyone who has rehabilitation needs. Here the focus is not a on a minority group, but on Experiencing Disability itself. Since over the life course everyone experiences some level of health decline, and since everyone ages, this experience of disability is not merely conceptually, but epidemiologically universal.
What we see in these WHO initiatives is a tension between two understandings of the experience of disability: one restricted to a minority group (persons with disabilities) and the other a universal feature of humanity (experiencing disability). The objective of this paper is to clarify these perspectives on disability, to express carefully how they differ and the tensions that result, and to explore the possibility of reconciling these perspectives for a more powerful and clarified social response to disability. To do so, we rely on the contrast between the defining objective of rehabilitation as a health strategy, namely to optimize functioning, and the broader social objective of inclusion that is at the heart of the current disability human rights movement and the long history of political activism by persons with disabilities. We argue that these objectives are not themselves in conflict, but are complementary.
This paper sets the stage of the second debate of the European Academy of Rehabilitation Medicine (EARM) in the “Debates in Rehabilitation Medicine” series published in collaboration with this journal (15). Readers of the journal are invited to join the debate by submitting letters to the editor.
There is broad consensus about the conceptualization of disability. For nearly 50 years, and across disciplines from the health sciences, sociology, politics and law, disability has been generally understood to be rooted in physiological and psychological functioning (that is, health states), but experienced in terms of activities, relationships and roles that are created, or strongly shaped, by the physical, human-built, attitudinal and social environment. Political debates about “models of disability” that occupied past decades have more or less resolved into this broad consensus, although there remain different versions of this “interactional model” of disability. Most prominent is the so-called “biopsychosocial” model found in WHO’s ICF, but it is also reflected in the characterization of disability in the CRPD: “…disability results from the interaction between persons with impairments and attitudinal and environmental barriers that hinders their full and effective participation in society on an equal basis with others.”
Although the interactional approach is the modern consensus, there nonetheless remains a deeper ambiguity about the experience of disability and who experiences it.
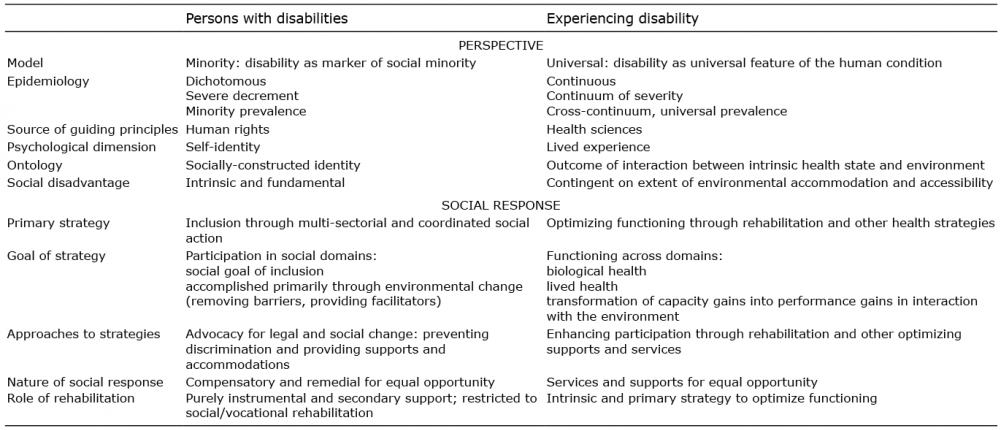
The difference between being a person with disabilities and experiencing disability might at first appear to be a linguistic variation, but it is deeply theoretical, has historical roots and far-reaching social consequences. The two perspectives effectively generate different connotations of the word “disability”, one linking it to a socially-constructed disadvantage or devalued social status, the other to the outcome of sub-optimal health states interacting with the physical and social environment. For a variety of reasons that will be described below, the nature of rehabilitation as a health strategy is at the heart of the tension. Specifics of the differences in perspective and the social consequences discussed in this paper are set out in Table I. First, this paper briefly explores the historical roots of both perspectives.
Table I. The two perspectives compared: persons with disabilities and experiencing disability
What is often termed “minority group analysis” of disability was an outgrowth of the scholarship and political activism in the 1960s and 1970s in North America and Europe, and eventually came to be called the “social model of disability”. Advocates in the USA used the civil rights movement as their model (16, 17), while in the UK the basis was the Marxist analysis of social oppression (18, 19). Both groups relied on earlier medical sociological accounts of the “sick role” in the context of rehabilitation (20–22) as well as deviance theory and the dynamics of social marginalization (23, 24). Some theorists directly blamed health and human service professionals, especially rehabilitation therapists, for devaluing people with disabilities and, in effect, creating the disvalued social role of “the disabled” (25–27).
Although this analysis of disability was closely linked to “identity politics” (28), which emphasized the rigid social dichotomy between those with and those without disability, it was political scientist Harlan Hahn, in a series of influential articles in the 1980s, who had firmly aligned disability with the social dynamics of racial activism (29, 30), underscoring the crucial role of political advocacy to secure equal rights. The analysis in the US paved the way to the passage of The Americans with Disabilities Act, 1991 (ADA), the preamble of which directly borrows from The Civil Rights Act, 1960: “Individuals with disabilities are a discrete and insular minority who have been faced with restrictions and limitations, subjected to a history of purposeful unequal treatment and relegated to a position of political powerlessness in our society….’’ (31).
Like all rights-based political movements, the minority group or social identity analysis of persons with disabilities put full participation and social inclusion at the top of its advocacy agenda. As a political strategy and social movement calling for rights and remedies against discrimination, it was highly successful, if measured by the political attention the movement drew to the situation of persons with disabilities (32). Indeed, this perspective of disability can be credited with nearly every change in attitude and treatment of people with disabilities in the past 40 years, leading to the passage of the UN’s Convention on the Rights of Persons with Disabilities. Along the way, scholars such as Tom Shakespeare began to overlay the psychological dimension of disability self-identity (33) that addressed the stigma of biological inferiority by valorizing the identity, and further underscoring the separateness of persons with disabilities.
Given its very self-conscious, academic and political-activist provenance, the persons with disabilities perspective has clearly articulated features. Being modelled on the American civil rights experience, it was essential that people with disabilities be a “discrete and insular minority”, which in effect meant that, epidemiologically, disability needed to be a dichotomous notion: one is either a person with disabilities or not. To make sense of this, only those with long-term, serious and severe impairments (people who are blind or severely visually impaired, deaf or substantially hearing impaired, etc.) could be thought to be “disabled”. As the lives of people with severe impairments were more profoundly changed by the experience, the plausibility of being socially disadvantaged and adopting a self-identity of person with disabilities was plausible. Indeed, some disability advocates strongly objected to people with temporary health problems, however incapacitated (or discriminated against), or those whose impairments were seen as self-created (obese people or substance abusers) to be viewed as persons with disabilities (17).
The minority status of persons with disabilities was consequence of the fact that this status was “socially constructed” by social and economic forces that undervalued the persons with disabilities identity. This was manifested in discrimination, prejudice, lack of equal opportunity and other social disadvantages. These disadvantages, moreover, were neither accidental nor contingent, but intrinsic to the very ontological status of being (viewed as) persons with disabilities. Since these social disadvantages were based on persistent attitudes and misperceptions, the only effective remedy was to address the social structures that reinforced attitudes and misperceptions. The most effective political and legal basis for the social remedies needed was legally enforced human rights, a strategy which, by the late 1990s, was inextricably incorporated into the persons with disabilities perspective.
The other perspective on the experience of disability follows from the fact that people are biological entities that experience diseases and injuries that affect their biological functioning. These assaults on health, in turn, impact on the things people can do in their lives, from reading a book, to going to school, doing a job, and being a parent, neighbour, community member or citizen. Human beings break down, fall apart and eventually die. This is not social construction; impairments are universal facts. Importantly, impairments are also variable in severity; the basic body function of visual acuity ranges from some statistically determined level of normality to a mild and moderate impairment, to a serious degree of limitation to, finally, blindness or a total loss of visual acuity. All body functions (and structures) follow this pattern; they are experienced, and assessed, on a continuum. We can prevent some health problems that lead to impairments, and slow the progress of decline, but in the end, impairments of some level of severity, like death itself, are simply unavoidable.
It is fair to say that this perspective on disability has always been (and associated with) the medical understanding of disability (historically replacing the more ancient and moralistic view of inferiority, immorality or a pitiable existence) (34). Yet this basic view is not monopolized by health professionals. For example, American sociologist Irving Zola in his paper “Toward the necessary universalizing of a disability policy” (35), argued that the minority approach to disability, although a productive short-term political strategy, simply could not be sustainable for the long term. It is a mistake, he argued, to think that disability is a dichotomous notion, applicable only to those with permanent and severe impairments. Disability is a near universal phenomenon, part of the human condition. Optimally, therefore, social policy should also be universal, applicable to everyone experiencing or at risk of experiencing disability of any level of severity. A universal policy would match the level of resource, service, or support to the level of need, recognizing that impairments, though dynamic over the life course tend, given ageing, to be increasing in both number and severity.
Zola’s views might have been radical to sociologists and disability advocates, but it was the unspoken consensus amongst rehabilitation professionals, especially occupational therapists (36), for whom disability was an infinitely various, yet universal feature of humanity. Since no one could claim to possess a complete repertoire of capacities, suitable for all permutations of the physical and social environment, both epidemiologically and clinically people exhibit a spectrum of abilities, changeable over time. As Zola himself later stated, “having a disability was not a fixed status, but rather a continually changing, evolving and interactive process’’ (37).
Recent work by rehabilitation professionals, particularly under the auspices of the International Society for Physical Medicine and Rehabilitation (ISPRM) have used the ICF, and specifically the key notion of functioning, as the basis for conceptually characterizing rehabilitation and its objectives (38). As a health strategy, rehabilitation aims to optimize a person’s functioning by improving both his or her biological health and lived health in concert, and achieves this through the provision of treatment for health conditions to optimize intrinsic health capacity, by strengthening a person’s psychological resources and assets and facilitating the person’s immediate environment, so that this is translated into enhanced performance and improved lived health (5, 7).
Activities and interventions towards optimizing functioning and reducing disability constitute the social response to disability. But here the underlying tension between the two perspectives on disability has taken its toll. One of the persistent themes of the persons with disabilities perspective has been the distrust of professionals, especially health professionals and, within this group, most particularly rehabilitation professionals. Few health professions have experienced the kind of criticism and depth of animosity directed to them by disability advocates, who, firmly wedded to the persons with disabilities perspective, have claimed that rehabilitation professionals have essentially colonized persons with disabilities forcing them into a dependent social role that undermines their independence (27, 39, 40). This view appears to be reinforced by frequent studies suggesting a “zero concordance” between disabled people and rehabilitation professions about unmet rehabilitation needs (41). The unstated assumption seems to be that rehabilitation professionals seek to mould the person to an environment that is a given and cannot be changed, and, when this is impossible, to relegate the individual to the social sidelines. Although frequently hinted at in the disability studies literature (42), this assumption profoundly misunderstands the objective of rehabilitation and the self-perception of rehabilitation professionals themselves.
It may be that part of this distrust of rehabilitation professionals is the result of the belief that, given their objective of optimizing functioning, they are somehow at odds with the broader political objective of disability advocates, namely full participation and social inclusion. We will return to this issue below, but first it is important briefly to describe how these perspectives create strategies of policy development that often reflect an ambiguity of purpose (once again, summarized in Table I).
Strategically, the persons with disabilities perspective argues that the social disadvantage of disability are caused by society; either through ignorance, benign neglect or, more rarely, by design and overt discrimination. Because of this, the appropriate social response must be to ensure social inclusion at the individual level by means of political advocacy towards legal and policy change. The focus of this legal and policy change must be both negative (to prevent and compensate for discrimination and prejudice) and positive (to provide the accommodations and supports needed for enhanced participation).
The experiencing disability perspective argues that the social disadvantages the individual experiences are jointly determined by underlying health conditions, and resulting impairments, as well as by environmental barriers (or the absence of environmental facilitators). Thus, the social response must be more nuanced. As the underlying health condition creates functioning problems that cause disadvantage, some form of health intervention must be provided to improve and optimize a person’s capacity. Improving capacity, however, may not be enough (or may not be possible), in which case some form of environmental adjustment or modification will be required. This can take the form of the provision of appropriate assistive devices (eye glasses, hearing aids, wheelchairs, and communication devices), personal assistance, or the removal of unnecessary environmental obstacles (providing ramps or widening doors for persons in wheelchairs) or both. As these services and supports are socially-provided, it is inevitable that facilitating laws and policies will also be required.
The differences are subtle, but have an impact on how policy is designed. The persons with disabilities perspective insists that the appropriate social response to the injustice experienced by persons with disabilities is essentially compensatory or remedial, given that most environmental barriers (or failures to provide facilitators) are a feature of social design and thus are changeable. To make this case, however, advocates tend to downplay the essential need for health interventions to enhance intrinsic capacity (medical, pharmaceutical and rehabilitative), turning their attention to the goal of inclusion and emphasizing the unfairness of forcing people with “physical differences” to make their way in a human-built environment designed for people without impairments.
The experiencing disability perspective tends to focus on interventions that directly address health status and changes to the immediate environment. Supports and services are provided, not as compensation for past discrimination, but as part of a general social obligation to ensure equal opportunity for all citizens by optimizing functioning, through the provision of rehabilitation and other health services. For their part, health professionals may inadvertently downplay the importance of broader social change for inclusion, completely outside of the health sector, especially if social resources are drawn away from the health sector to address social change.
The two perspectives on disability have different lineages and strategically impact social policy in different ways. Each has strengths and weaknesses: although, epidemiologically, limitations in functioning are a universal human experience, it is obvious that more severe impairments impact individuals more profoundly than milder ones and those impairments have very different impacts on the lived experience in different social environments. These realities could justify highlighting, however artificially, the needs of a minority group of persons with disabilities for advocacy purposes. At the same time, given the ageing population and increasing prevalence of chronic, non-communicable diseases, it is essential that society prepares itself to respond, not only to the obvious needs created by severe impairments, but also to the needs created by mild and moderately severe impairments. For these impairments are experienced by a much larger population for whom prevention and rehabilitation efforts can have the greatest benefit (43).
Disability advocates are undoubtedly correct that persons with disabilities have historically been, and continue to be, denied basic human rights, which limits their opportunities to participate fully in society. Nonetheless, the long-term social goal of inclusion is simply unachievable without access to health and rehabilitation services to optimize functioning. This said, although optimizing functioning is a necessary condition for social inclusion, it is not sufficient. Health professionals need to appreciate that, though theirs is a necessary contribution to that broader social goal, much more needs to be done, and many more social agents need to be involved.
This suggests a potential resolution to the tension of the two “disabilities”: the strength of the persons with disabilities perspective is its capacity for political advocacy, and this, in part, is a function of artificially restricting its constituency to a minority of people with severe impairments. However, this is also its fundamental weakness. In order to meet the challenges of demographic and epidemiological trends, the growing population of persons experiencing mild or moderate levels of impairment must also have a call on our social resources, since interventions will be needed to prevent these impairments from producing, in interaction with the environment, more disability in the world. The interests of this much larger group (i.e. in effect, everyone over the life course) should not be ignored. The strength of the experiencing disability perspective is that it emphasizes the universality, and therefore the normality, of disability and the need to effectively address it through basic health and rehabilitation services. At the same time, the political goal of inclusion is unachievable without a coordinated effort by many agents of the state across many, perhaps all, areas of state action.
Perhaps then, the tensions between the perspectives can be addressed by a clearer division of labour. The objective of health professionals in general, and rehabilitation professionals in particular, is to effectively and efficiently optimize functioning and minimize the impact of disability, or its risk. This should be viewed as an essential component of the broader social goal of inclusion. At the same time, this contribution of rehabilitation to inclusion should be appreciated as such by those who have chosen to represent a subset of the population who, perhaps, has been the most highly impacted by disability in their lives. For their part, health professionals should also appreciate their role in the context of, and answerable to, the broader social goal of inclusion, which requires cooperation across social agents. In other words, when the WHO produced the World Report on Disability they were contributing to the wider social agenda, doing their part as the UN agency for health to give a full, 360° picture, of disability in terms of the lived experience of health. The World Report on Disability made it clear that there are many social agents that need to join forces to bring about inclusion, agents that include, but go far beyond, the sphere of health. The Rehabilitation 2030: A Call for Action, on the other hand, is WHO’s more focused contribution to social inclusion: turning back to the area it knows best, health, and showing how rehabilitation is a necessary condition for inclusion for those experiencing disability.
The authors would like to thank Professors Christoph Gutenbrunner, Alessandro Giustini and Mr Jan Monsbakken for fruitful discussions that led to the evolution of the two perspectives on disability discussed here. The authors would also like to extend their appreciation to Cristiana Baffone and Susanne Stucki for their support during the preparation of the manuscript.
The authors declare no conflicts of interest.


 Click to show fullsize
Click to show fullsize