
From the Swiss Paraplegic Centre Nottwil, Nottwil, Switzerland
Study design: Prospective cohort study.
Objective: To investigate the changes in resting energy expenditure and body composition over time in a cohort of patients with spinal cord injury during acute treatment, rehabilitation, and 2 years after the end of rehabilitation.
Methods: Adult patients admitted for acute treatment and rehabilitation after traumatic spinal cord injury were recruited. Measurements of resting energy expenditure and body composition were scheduled at 2, 6, 10 and 14 weeks after spinal cord injury, at the end of rehabilitation, and 2 years later.
Results: Patients’ mean age was 38.8 years (standard deviation 14.0). Resting energy expenditure began to decrease up to the 10-week measurement (p = 0.02) and further decreased after the 130-week measurement (p < 0.001). Body weight was already decreased after the 6-week measurement (p < 0.01) and increased after the end of rehabilitation (p = 0.009). Percentage body fat mass showed similar changes.
Conclusion: After an initial decrease in resting energy expenditure, body weight and percentage of body fat, these values levelled off during the rehabilitation period. After the end of the rehabilitation period, body weight and body fat mass increased again to the baseline levels, whereas resting energy expenditure decreased further. These results suggest that rehabilitation programmes should focus on adapting to these foreseeable changes.
Key words: spinal cord injury; paraplegia; tetraplegia; energy expenditure; body composition; obesity.
Accepted May 3, 2017; Epub ahead of print Jun 28, 2017
J Rehabil Med 2017; 49: 579–584
Correspondence address: Peter Felleiter, Swiss Paraplegic Centre Nottwil, Guido A. Zaech Str. 1, CH-6207 Nottwil, Switzerland. E-mail: peter.felleiter@paraplegie.ch
Severe trauma induces massive metabolic changes that are part of the adaptive survival response to critical illness. These acute changes are characterized by hypermetabolism, with increased energy expenditure and protein catabolism (1). Early enteral feeding and, if necessary, parenteral feeding, are therefore a major focal point of modern intensive care medicine (2). Whereas other survivors of severe trauma typically regain muscle mass during rehabilitation, patients with acute spinal cord injury (SCI) continue to lose muscle mass over time, which leads to changes in body composition and a significant decrease in basal metabolic rate (3).
Several cross-sectional studies have shown that most patients with SCI typically gain weight after surviving the acute phase, even though their muscle mass decreases due to inactivity (4, 5). Patients with SCI are also prone to accumulate fat mass due to specific hormonal and metabolic changes (6). Another explanation for the weight gain in non-ambulatory individuals with SCI is that their food intake may remain unchanged from before the injury, whereas their energy expenditure decreases (7–9). This results in a significantly higher body fat percentage in individuals with SCI compared with those without SCI (3, 10, 11).
An unchanged diet for patients with SCI, which does not take into account their reduced energy expenditure, leads to weight gain and obesity. This exposes many patients with chronic SCI to the unfavourable health-related consequences that follow a traumatic SCI event. Obesity increases the risk of cardiovascular disease, as well as many other metabolic, sleep, and orthopaedic disorders, e. g. osteoarthritis (12, 13). A previous cross-sectional study suggests that changes in body composition occur over time in individuals after SCI (3). However, the timeline of changes in energy expenditure and body composition between the acute and chronic phase of SCI has not been analysed (14). This information would help provide adequate caloric intake and improve nutritional counselling for patients with SCI. The aim of this study was therefore to investigate the timeline of changes in energy expenditure and body composition in patients with SCI following injury. Our primary hypothesis was that significant changes in energy expenditure and body composition arise in patients with SCI during the period of acute treatment, rehabilitation and the 2 years following the end of rehabilitation. Our secondary aim was to analyse whether these changes differ between individuals with paraplegia and tetraplegia.
The investigation was performed at a 140-bed SCI rehabilitation centre in Switzerland. The study was approved by a research ethics committee (Northwestern and Central Switzerland) and is registered at ClinicalTrials.gov (no. NCT01980784).
Inclusion criteria. All patients admitted for acute treatment and rehabilitation after traumatic SCI were screened within the first 2 weeks following the traumatic event. The following inclusion criteria were used: age 18–70 years, body mass index (BMI) 18–30 kg/m2, neurological level of injury C4 to T12, American Spinal Injury Association Impairment Scale (AIS) A, B or C, and written informed consent (15).
Exclusion criteria. The following exclusion criteria were used: complications during acute treatment that may interfere with study participation or skew study results, pre-existing type 1 or type 2 diabetes mellitus, pre-existing hypercholesterolaemia, untreated hypothyroidism or hyperthyroidism, invasive mechanical ventilation, and presence of a cardiac pacemaker.
Personal demographics and results from the neurological level of injury assessment were collected. The severity of SCI was classified using the AIS. Routine blood tests were used to verify continual absence of all exclusion criteria throughout the study.
Measurements of resting energy expenditure (REE) and body composition were scheduled at 2, 6, 10 and 14 weeks after SCI, at the end of rehabilitation (at the latest after 26 weeks) and at 2.5 years (130 weeks) after SCI. Body composition was evaluated by bioelectric impedance analysis (BIA), using the Bodystat 1500 (Bodystat Ltd, Douglas, Isle of Man, UK). REE was measured at the bedside, using the indirect calorimeter MedGem (Microlife Inc., Golden, CO, USA), and calculated from measured oxygen uptake. The tests were performed according to the manufacturer’s recommendations.
All tests were performed at 08.00 h after a fasting period of at least 8 h. Patients received no food for 8 h prior to the measurements, only water or unsweetened tea, and no caffeine or alcohol for 12 h prior to data collection. Strenuous physical activity and smoking were not allowed for 12 h prior to the measurements. The patients’ bladders were emptied prior to collecting the measurements. Patients rested for 15 min in a supine position before the BIA measurement, and indirect calorimetry was subsequently carried out.
The sample size was calculated using nQuery Advisor 2.0 (Statistical Solutions Ltd, Cork, Ireland). Due to lack of data on the development of energy expenditure in individuals during the first year after SCI, we used data from a study by Baumann et al. This study measured energy expenditure in pairs of monozygotic twins discordant for SCI (7). A sample size of 22 was calculated to detect a significant difference (effect size = 1.019) in REE between baseline and follow-up values, with an α-error of 0.05 and a power of 90%. To adjust for an assumed dropout rate of 10–20%, the sample size was set to 25.
Data are presented as the mean and standard deviation (SD). The data were tested for a normal distribution using QQ-plots, the Kolmogorov-Smirnov test and the Shapiro-Wilk test. A 2-way repeated measures analysis of variance (ANOVA) was used to test for significant differences in various timed measurements between the 2 patient groups (paraplegia and tetra-plegia). Post-hoc analyses were performed with the Bonferroni correction. All statistical analyses were performed using SPSS software (version 18.0.3, IBM, Somers, NY, USA). A p-value ≤ 0.05 was considered significant.
A total of 30 patients were screened for study participation. Three patients declined to participate and 2 were excluded after their blood analyses showed either hypercholesterolaemia or untreated hypothyroidism. One further patient was excluded during the course of the study because a protocol review showed a violation that had gone unnoticed (BMI >30 kg/m2).
Thus, a total of 22 men and 2 women were analysed in this study. Their neurological levels of injury ranged from C4 to T12. Of the participants, 16 were paraplegic and 8 were tetraplegic. All remained wheelchair users during the course of the study. There were 16 patients with an AIS assessment score of A, 5 with a score of B and 3 with a score of C. The patients’ ages ranged from 18 to 60 years, with a mean age of 38.8 (SD 14.0) years. The patients’ BMI ranged from 19.3 to 29.9 kg/m2 (mean 24.3, SD 2.8 kg/m2).
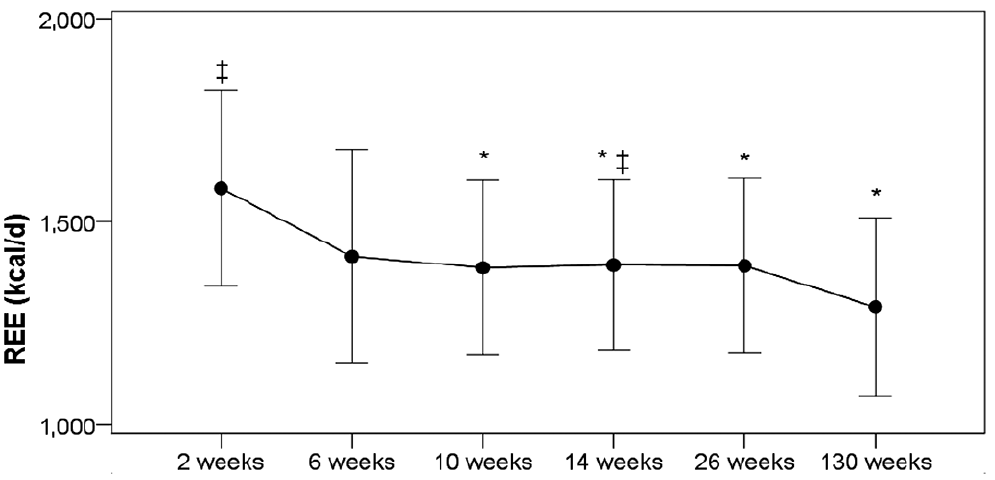
Measurements of REE, body weight and percentage of body fat mass over time are shown in Figs 1–3. Additional information about these parameters is provided in Table I. REE began decreasing after the 10-week measurement (p = 0.02), levelled off during the remainder of the rehabilitation period, and finally decreased further after the 130-week measurement (p < 0.001) (Fig. 1). Body weight was already decreased at the 6-week measurement (p < 0.01), remained unchanged until week 26 and started to increase again after discharge from rehabilitation (p = 0.009) (Fig. 2). The percentage of body fat mass showed similar changes, decreasing at the 10-week measurement (p = 0.024) and returning to the baseline value at the 130-week measurement (p = 0.039) (Fig. 3).
Fig. 1. Resting energy expenditure (REE) during the study interval. *Significantly different from 2-week value. ‡Significantly different from 130-week value.
Fig. 2. Body weight during the study interval. *Significantly different from 2-week value. ‡Significantly different from 130-week value.
Fig. 3. Percentage of body fat during the study interval. *Significantly different from 2-week value. ‡Significantly different from 130-week value.
Table I. Resting energy expenditure and body composition of the evaluated individuals
Analysis of REE, body weight, and percentage of body fat mass measurements between the 2 patient groups (paraplegia and tetraplegia) showed no significant differences (Figs 4–6). Demographic data describing the 2 groups are provided in Table II.
Fig. 4. Resting energy expenditure (REE) of patients with paraplegia and tetraplegia during the study interval. No significant differences between the groups.
Fig. 5. Body weight of patients with paraplegia and tetraplegia during the study interval. No significant differences between the groups.
Fig. 6. Percentage of body fat of patients with paraplegia and tetraplegia during the study interval. No significant differences between the groups.
Table II. Baseline characteristics of the 2 evaluated groups (n=24)
Although several studies have been published on post-traumatic changes in energy expenditure and body composition in individuals with SCI, none have analysed these changes over the acute post-traumatic phase (0–4 weeks) and only a limited number have analysed these changes over the subacute (4–26 weeks) and chronic phase (14, 16, 17). Therefore, we present here the first continuous data-set containing measurements of post-traumatic changes in energy expenditure and body composition in patients with SCI from 2 weeks post-injury (acute phase) to 2.5 years post-injury
(chronic phase).
During the acute phase, REE decreases significantly, and remains at this level during rehabilitation in the subacute phase. After the patients returned home and at 2.5 years after injury, we were surprised to find that REE decreased further. The percentage of body fat was lower after 10 and 14 weeks, but then began increasing again to the level at admission. Likewise, the body weight of the patients decreased significantly during the acute phase, levelled off during the subacute phase, and increased after 2.5 years post-injury.
Until now, no continuous data have been available on the changes in REE during the acute phase following SCI. During the subacute phase (65.5 days post-injury), Cox et al. (5) reported a mean REE of 1,556 kcal/day in a 22-patient study. A portion of these patients had Brown-Sequard syndrome, so information regarding AIS assessment and ability to ambulate is not available. This may explain the higher caloric needs reported in that study. Two studies on patients with chronic SCI, one by Bauman et al. (7) and the other by Mollinger et al. (8), reported a mean REE of 1,387 kcal/day and 1,376 kcal/day, respectively. These results are congruent with the mean caloric need of 1,397 kcal/day measured in our patients between 6 and 26 weeks post-injury. Gorgey et al. (18) reported a basal metabolic rate of 1,494 kcal/day in patients > 1 year after SCI, which is higher than we measured. When comparing these data it should be taken into account that obese patients were excluded from participation in our study, but were not excluded in the other studies.
Longitudinal data-sets on the changes in body composition during the acute and subacute phases after SCI are not available. An increased body fat percentage of 30% and more in patients with chronic SCI has been described in various papers (3, 10, 18). This increase is less dramatic in younger patients and tetraplegic patients, compared with paraplegic patients (3, 10). In all these studies dual-energy X-ray absorptiometry (DEXA) was used for the measurement of body composition. Whereas DEXA both requires expensive technical equipment and exposes patients to radiation, BIA is a bedside method and requires only minimal technical expertise. BIA and DEXA are considered equally valuable for analysis of body composition in patients with SCI (19). Probably due to the limited number of individuals we were unable to detect any differences in body composition or REE between patients with paraplegia and tetraplegia.
Our study excluded obese patients and enrolled a younger study participant population than other similar studies. In addition, only one-third of our study participants were tetraplegic. This may, in part, explain why the percentage of body fat is considerably lower in our patients than in patients with SCI from other studies. However, how much the body fat will continue to increase following our observation period of 2.5 years is unknown.
The limitations of the current study include using a single centre specializing in the treatment of patients with SCI for over 25 years, since it offers an elaborate system of counselling that may influence patients’ behaviours. In addition, obese patients were excluded from participation in our study, making it difficult to apply our results to this growing population group. Finally, there were a limited number of patients in our study who we collected measurements from, similar to most long-term studies beginning in the acute phase.
The acute post-traumatic phase is characterized by spinal shock, resulting in hypotension and often requiring therapy with high fluid volumes and vasopressors. The mechanical trauma is often aggravated by additional trauma caused by surgical interventions targeted at enabling early mobilization. Similar to the changes in critical illness patients during this catabolic phase, a variety of clinical changes were identified from our study population, including increased energy expenditure and decreased muscle mass. Early enteral and parenteral nutrition are necessary for adapting to the various energy, protein, and micronutrient requirements during the different phases of recovery. Early onset of a reduction in body mass is typically observed in patients with SCI. The atrophy of muscle tissue during the acute phase is a clinically visible phenomenon and decreases lean body mass. Body water is another component included in lean body mass and may influence these results. Changes in body fluid may also influence BIA measurements, as total body fat is underestimated in persons with generalized oedema (20). The decrease in body fat mass observed early in the rehabilitation period may reflect an imbalance in nutritional state and physical activity. The REE is dependent on body and muscle mass, and therefore reflects these changes.
The subacute phase is characterized by a controlled environment in a rehabilitation unit, which provides optimally balanced nutrition and focused physical activities for patients as a training of basic functions, skills, and muscular and cardiovascular endurance. The controlled nutritional supply and continuous encouragement of physical activity provided to patients by the rehabilitation centre supports patients in building muscle mass in the innervated areas of their bodies. This should increase the lean body mass, although there is, in parallel, an ongoing reduction in muscular mass in the paralysed areas of the patients’ bodies.
In most cases, the patients experience new challenges after returning to their homes following the rehabilitation period. These challenges include maintaining a structured day, continuing physical activities, and avoiding quantitative and qualitative malnutrition (8, 11, 21, 22). Surprisingly, 2.5 years after the trauma, body weight and body fat mass had increased back to baseline levels, whereas REE had further decreased. These findings may reflect the challenges of returning to a normal lifestyle after having strict regulations concerning nutrition and physical activity during rehabilitation. Patients may also be less physically active after rehabilitation. The further decrease in REE reported may reflect the inactivity of muscles in innervated areas that had been activated during rehabilitation. If patients return to their pre-traumatic nutritional habits, they will probably overeat and this will result in increased fat tissue and body mass. Unfortunately, overweight and obesity increases the risk of diabetes and cardiovascular disease in these patients.
High-quality medical rehabilitation programmes and the therapists that they employ should therefore focus on adapting to these foreseeable changes. It is not only necessary to provide a balanced nutrition and physical activity regimen to patients with SCI during the rehabilitation period, but it is also important to incorporate these topics into patient education programmes. Furthermore, patients’ relatives should also receive this education. Measurements of body mass are simple and inexpensive. These should be scheduled on a regular basis and the results communicated and discussed with the rehabilitation therapists. Nutritional counselling should be a mandatory element of a rehabilitation programme, since it informs patients of the dietary measures necessary for preventing an overweight body composition and the successive complications that result.
This study was sponsored by the Swiss Paraplegic Foundation.
The authors declare no conflicts of interest.


 Click to show fullsize
Click to show fullsize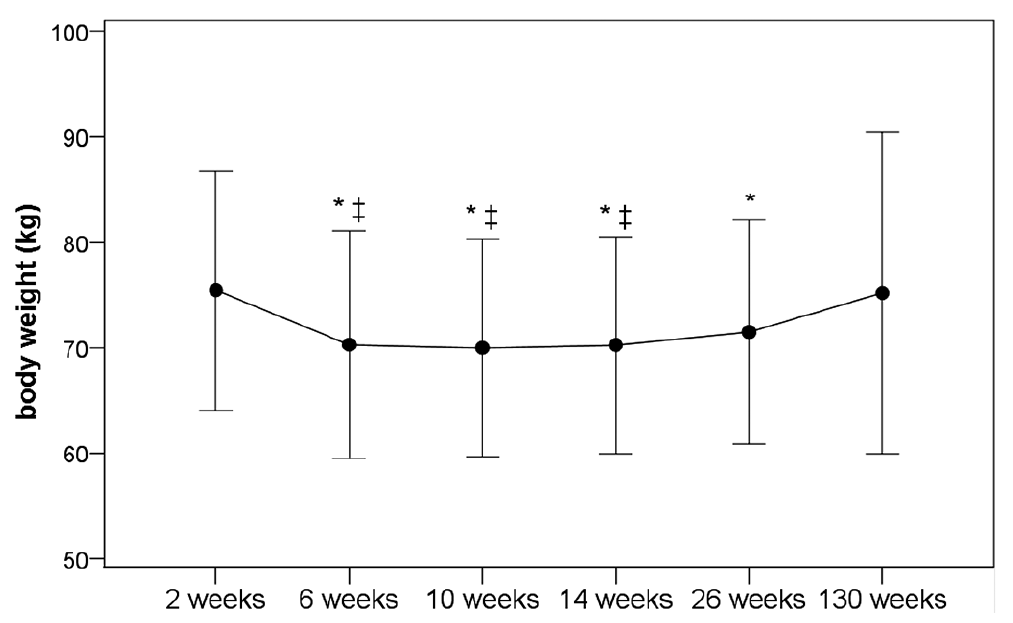 Click to show fullsize
Click to show fullsize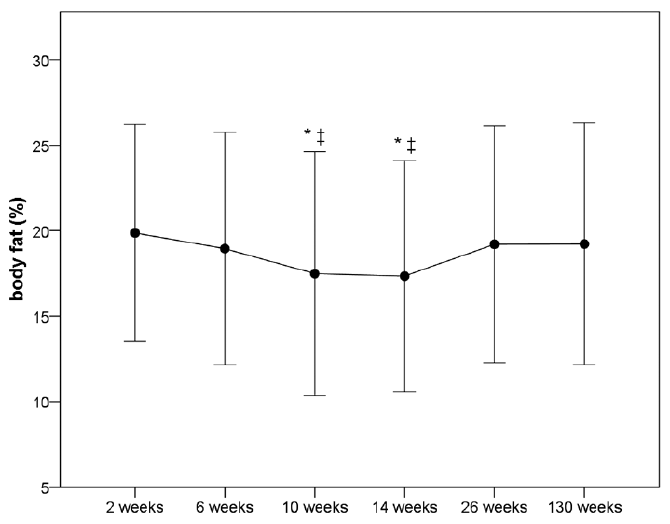 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize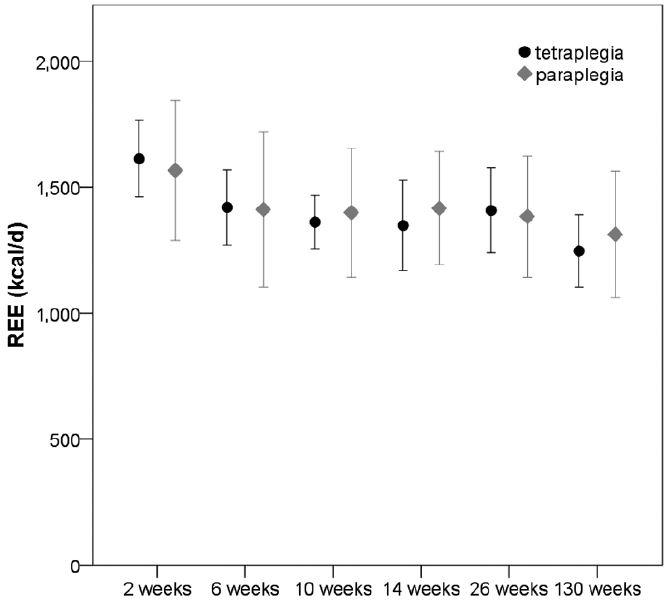 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize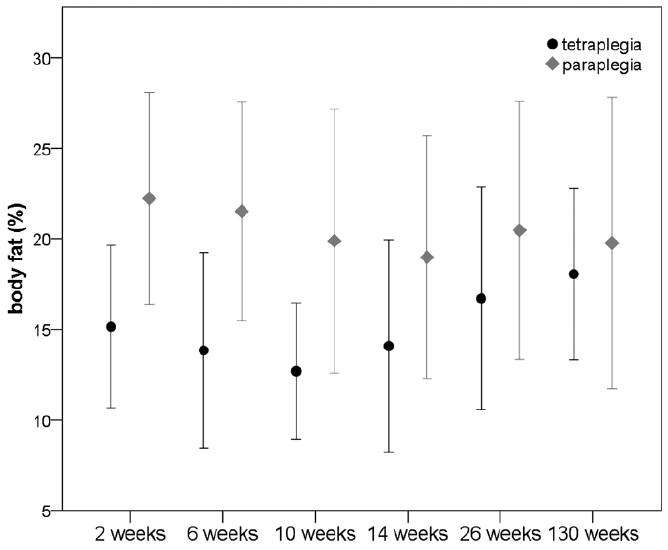 Click to show fullsize
Click to show fullsize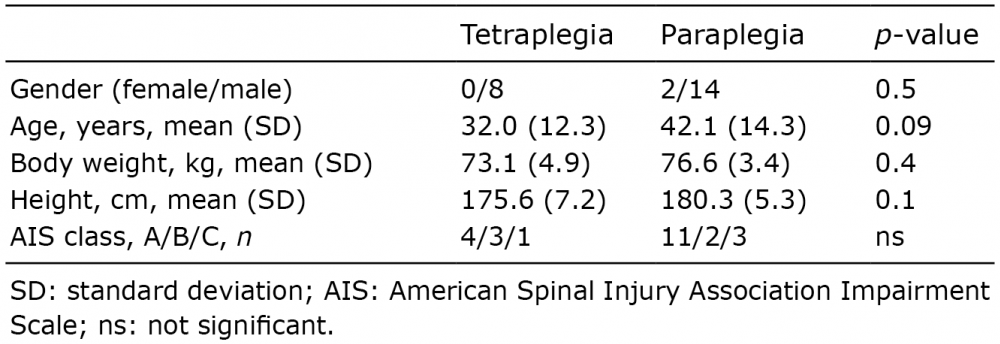 Click to show fullsize
Click to show fullsize