
From the 1Maisonneuve-Rosemont Hospital Research Center, University of Montreal Affiliated Research Center, Montreal, 2Department of Rehabilitation, Faculty of Medicine, Laval University, Quebec City, 3Center for Interdisciplinary Research in Rehabilitation and Social Integration, Quebec, 4Research Center of the Quebec University Hospital Center – Laval University, Quebec, Quebec, 5School of Rehabilitation Science, McMaster University, Hamilton, Ontario and 6School of Rehabilitation, Faculty of Medicine, University of Montreal, Montreal, Quebec, Canada
Objective: To perform a systematic review and meta-analysis of randomized controlled trials on the efficacy of workplace-based interventions to prevent or treat shoulder pain.
Data sources: A systematic review of 4 databases was performed up to January 2016.
Study selection: Randomized controlled trials were included if the intervention under study was a workplace-based intervention performed to prevent or reduce shoulder pain and disability in workers.
Data extraction: The methodological quality of the studies was evaluated and meta-analyses were conducted. Pooled mean differences and risk ratios were calculated.
Data synthesis: Data from 4 studies on strengthening exercises performed in the workplace for workers with shoulder pain (n = 368) were pooled. A statistically significant reduction in pain intensity was observed compared with different control interventions (mean differences (scale out of 10) 1.31 (95% confidence interval (95% CI) 0.86–1.76)). Pooled data from 5 studies on the efficacy of workstation modifications (n = 2,148) showed a statistically significant reduction in the prevalence of shoulder pain with a risk ratio of 1.88 (95% CI 1.20–2.96) compared with different control interventions.
Conclusion: Low-grade evidence exists that a workplace exercise programme may reduce the intensity of shoulder pain, and that workstation modifications may reduce the prevalence of shoulder pain.
Key words: exercise; ergonomics; intervention; shoulder pain; work.
Accepted Apr 7, 2017, Epub ahead of print XX, XXXX
J Rehabil Med 2017; 49: 529–542
Correspondence address: François Desmeules, Unité de recherche clinique en orthopédie/ Orthopaedic Clinical Research Unit, Centre de recherche de l’Hôpital Maisonneuve-Rosemont (CRHMR) 5415 Blvd L’Assomption, Pav. Rachel Tourigny, bureau/office 4163, Montréal, QC H1T 2M4, Canada. E-mail: f.desmeules@umontreal.ca
Work-related upper extremity disorders (WRUED) constitute a highly prevalent problem with a point prevalence of up to 53% in certain working populations (1). Shoulder pain represents an important subgroup of WRUED (2, 3) and incurs important health care costs as well as indirect costs from productivity loss and work absenteeism (4).
The incidence of shoulder disorders in workers is related both to individual and work characteristics as well as psychosocial factors (5). Repetitive movements, awkward postures, working with arms above shoulder level, vibration, older working age or work seniority have been identified in several studies as work-related risk factors for the development of shoulder problems (6). Psychosocial risk factors that have been associated with the incidence of shoulder pain or delayed return to work in workers in several studies include high psychological stress (high job demands combined with low control over work), low social support, and job dissatisfaction, but the strength of the associations observed varies from study to study (7).
Multiple interventions have been advocated to prevent WRUED and to promote return to work in workers with WRUED or with shoulder disorders. Strengthening and stretching exercises, workstation adaptation, schedule and task modifications or psychosocial interventions such as cognitive behavioural training and stress management programmes are some of the possible interventions aimed at reducing pain and disability and at promoting working ability in workers. Many experts advocate that tailored workplace interventions may be more efficacious than usual care in a clinical setting outside the workplace and, there is emerging evidence to support such claims (8). A recent systematic review on the efficacy of workplace-based exercise programmes for occupational non-specific neck and upper-extremity pain concluded that there was strong evidence that specific upper extremity resistance training in the workplace could reduce shoulder pain in the short term (9). Another recent systematic review by the Cochrane Collaboration concluded that supervised exercises with regular follow-up and reminders might be more effective to improve treatment adherence than home exercises for workers with chronic musculoskeletal disorders (10). Therefore, for workers, delivering exercises in the workplace might improve adherence to treatment and, in turn, treatment efficacy. Another Cochrane Collaboration systematic review evaluated the efficacy of ergonomic interventions in the workplace for neck or upper limb disorders (11). This time the authors concluded that there was low-grade evidence that ergonomic interventions are not effective for WRUED, with the exception of the use of an arm support in combination with the use of an alternative mouse to reduce upper extremity pain. None of these reviews, however, published results specific to workers with shoulder disorders. Since the prognoses for these disorders have been shown to differ (12) and as clinical practice guidelines recommend specific intervention strategies and therapeutic modalities for shoulder problems compared with neck or other upper extremity disorders (13), there is a need to specifically assess workplace interventions for workers with shoulder pain. Therefore, the aim of the current systematic review was to evaluate the available evidence with respect to the efficacy of workplace-based interventions to prevent or treat shoulder pain in workers.
This systematic review conforms to PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) methodological guidelines (14).
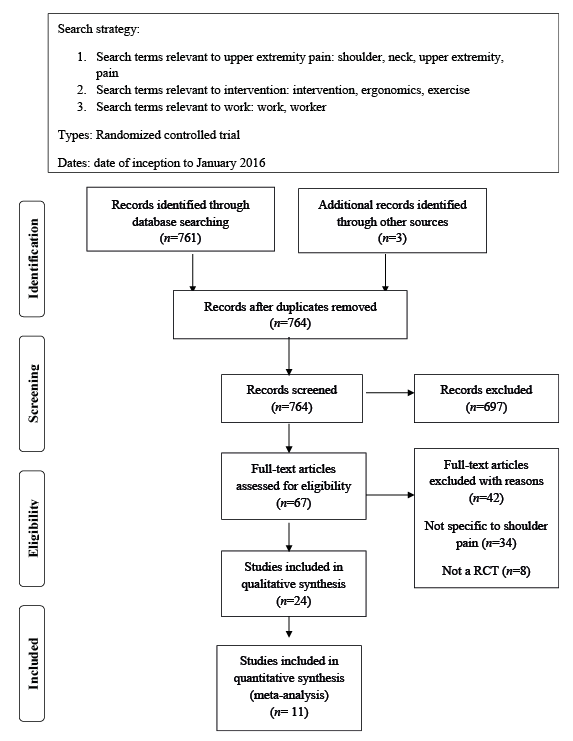
A literature search was conducted using a combination of keywords and MeSH (Medical Subject Headings) terms (Fig. 1). The search was performed in 4 databases (CINAHL, Embase, PubMed and PEDro) from their individual date of inception to January 2016. Hand searching of references from all retrieved articles was performed to identify additional relevant publications.
Fig. 1. Literature search results.
Study selection was based on the PICOS (patient, problem or population – intervention – comparison, control or comparator – outcome) framework (14). Titles and abstracts of all articles were reviewed to determine whether they met the following inclusion criteria: (i) included healthy adults (≥18 years) workers or adults workers with shoulder pain; (ii) the intervention under study was a workplace intervention or an on-site rehabilitation programme to prevent or to treat shoulder disorders compared with any other type of interventions; (iii) at least one of the reported outcomes was related to shoulder pain, either in terms of severity, prevalence or incidence; (iv) study design was a randomized controlled trial (RCT); (v) the language of articles was either English or French. The outcomes of interest included patient-reported outcomes specific to the shoulder, such as pain intensity and prevalence, functional limitations, as well as impairment-related outcomes, such as shoulder range of motion or muscle strength. Two evaluators (VL and ADC) participated in the screening and eligibility process and a third evaluator (FD) was consulted to resolve discrepancies.
Characteristics of the included studies were extracted by one evaluator using a standardized form and were all verified by a second evaluator. The following information was collected: study design, age, sex, types of rehabilitation and work-based interventions, occupation, outcome measures, duration of follow-up and results (Table I).
The risk of bias of the included studies was assessed with the Cochrane risk of bias tool (15). This instrument is a well-known and validated assessment tool used to assess the risk of bias in RCTs. This tool evaluates the risk of bias of a study in 6 methodological domains: sequence generation, allocation concealment, blinding (participants, provider and assessor), incomplete outcome data, selective outcome data reporting, and other sources of bias. Each item is appraised independently by 2 evaluators regarding its risk of potential bias: “unclear” indicates an unclear or unknown risk of bias based on the information presented in the study, “yes” indicates low risk of bias and “no” indicates high risk of bias. According to the Cochrane Collaboration, a study is reported as having a high risk of bias when one key domain is judged as having a high risk of bias (15). Based on the risk of bias within studies, the appraisal of the risk of bias across studies was used to grade the strength of the available evidence. Each methodological item was also attributed a numerical score; a score of 2 was given if a low risk of bias was present, a score of 1 if the risk of bias was unclear or unknown, and a score of 0 if a high risk of bias was present. Then, a total score (out of 16) was calculated to give an overview of the methodological quality and risk of bias of the included RCTs; where higher scores indicate a better methodological quality.
After the independent evaluation of each study, pair of raters met to compare ratings and resolve disparities. A structured consensus approach was used that involved: 1 – re-review of the manuscripts, 2 – discussion of the adherence to standards, and 3 – use of an independent third evaluator if consensus was not achieved.
Pre-consensus inter-rater reliability of the total methodological scores was assessed with an intra-class correlation coefficient (ICC). The studies that used the same interventions, outcome measures and follow-up period were identified, and results were pooled into meta-analyses. Analyses were performed using Review Manager (version 5.2) of the Cochrane Collaboration. Pooled mean differences (MD) and risk ratios (RR) were calculated with related 95% CIs (fixed effects models). The study weights were chosen using the usual method advocated by the Cochrane Collaboration in the Review Manager software. The statistical method combines results from multiple studies in the meta-analysis and weights studies by the amount of information they contribute (inverse variance of their effect estimate) and gives studies with narrower confidence interval more weight (16). To determine the degree of heterogeneity, testing was conducted using the I2 measure and an I2 < 60% was considered acceptable for pooling. Statistical significance was considered at p < 0.05. When included studies could not be pooled, a qualitative review of the evidence was performed by reporting main results of the study, evaluating the clinical and statistical significance of results and considering potential bias.
From the 67 potential articles identified after title and abstract review, 22 studies (24 published articles) met the eligibility criteria following full-text review (17–40) (Fig. 1). One study reported results from the same cohort of patients in 3 separate papers that were therefore analysed together (18, 22, 24).
Thirteen RCTs examined the effect of workplace exercise programmes (18, 19, 22, 24–27, 30–33, 35–37, 40). Exercises performed were very heterogeneous across studies. In 6 RCTs, the intervention was mainly strengthening exercises (18, 19, 22, 24, 26, 35, 36, 40), in 3 RCTs, it was stretching exercises (32, 33, 37) and, in one RCT, stabilization exercises for the trunk and shoulder were performed (27). Two RCTs reported results from a group of workers performing whole-body exercises, including aerobic, general strengthening and endurance, stretching and stabilization exercises not specific to the shoulder region or the upper extremity (25, 30). None of the exercise programmes were, however, specific to the worker’s tasks. Two of these RCTs also compared exercises with a psychosocial intervention (25, 27). One study compared a workplace-based exercise programme with an ergonomic intervention (31). Another RCT compared a workplace-based exercise programme with an ergonomic intervention to a clinic-based intervention (20).
Eight RCTs examined the effect of different ergonomic interventions (17, 21, 23, 28, 29, 34, 38, 39), 6 of which compared workstation modifications with a control intervention (17, 21, 28, 34, 38, 39). Two RCTs each compared different break schedules (23) or the use of a vibrating biofeedback computer mouse with a regular computer mouse (29).
The type of occupations of workers was also very heterogeneous across the included studies. One RCT did not mention the type of occupation of the participants (20). Nine RCTs included office workers (18, 19, 21–24, 28, 29, 31, 34, 37), 7 RCTs included factory employees (17, 30, 32, 33, 35, 36, 39) and 2 RCTs included laboratory technicians (26, 40). In the 3 remaining studies, the participants worked as hairdressers (38), healthcare workers (25) or cleaning workers (27).
Allocation concealment was unclear in all (17–25, 27–40) but one RCT, in which there was low risk of bias (26). There was a high risk of bias for blinding of personnel in all (17–39) but one study, in which the risk of bias was unclear (40), a methodological issue in rehabilitation studies, since treatment providers cannot be actually blinded, making all included studies at high risk of bias. The mean score of the methodological quality of the included studies was 55.1 ± 11.4% (range 37.5–75.0%) (Table II).
Table II. Risk of bias of included studies
The ICC for inter-rater agreement between reviewers on the evaluation of the risk of bias for the overall methodological score was 0.89 (95% CI 0.76–0.96). Pre-consensus inter-rater agreement for each items of the risk of bias tool ranged from high to perfect agreement (κ = 0.73 to 1.0).
Twelve RCTs with a high risk of bias compared an exercise programme delivered at work with a control group receiving education or with no intervention in groups of workers with or without shoulder pain.
Pooling of data for shoulder pain intensity was possible for 5 RCTs with a high risk of bias and a follow-up of 10 weeks to 10 months (n =765) (Table I) (30, 33, 35, 36, 40). These RCTs included patients with or without shoulder pain at baseline. The post-intervention scores were pooled and a statistically significant difference in favour of workplace exercises (general stabilisation, strength, coordination, endurance or flexibility exercises) was observed compared with the control group receiving simple advice to stay physically active or no intervention at all. The mean difference in pain intensity was (MD on 10-cm visual analogue scale (VAS)) of 0.46 (95% CI 0.24–0.69) (Fig. 2).
Fig. 2. Forest plot of pooled studies comparing an exercise programme with a control intervention for reduction in shoulder pain in symptomatic and asymptomatic workers. Post-intervention mean scores according to group allocation are presented for each study. Green squares represent between groups mean differences and the black diamond is the pooled mean differences with 95% confidence intervals.
Based on 4 studies that included only workers with shoulder pain at baseline, a secondary meta-analysis was performed. Data from these RCTs (n =368) of high risk of bias with a follow-up of 10 weeks to 10 months were pooled; a significant effect in favour of exercises in the workplace was observed for reduction in shoulder pain with a MD on a 10-cm VAS of 1.31 (95% CI 0.86–1.76) at a medium-to-long-term follow-up (26, 35, 36, 40) (Fig. 3).
Fig. 3. Forest plot of pooled studies comparing an exercise programme to a control intervention for reduction in shoulder pain in symptomatic workers. Mean pre-post intervention differences according to group allocation are presented for each study. Green squares represent between groups mean differences and the black diamond is the pooled mean differences with 95% confidence intervals.
Because of significant heterogeneity between studies (χ2= 10.1, p < 0.10 and I2 = 70%), pooling of data was not possible for 4 studies (n = 483) that assessed the efficacy of exercises in terms of reduction in prevalence of shoulder pain. Therefore, the 5 RCTs that included workers with or without shoulder pain at inclusion, were analysed qualitatively (27, 30, 32, 33, 37). No significant differences were observed between intervention groups performing stabilization, stretching or general exercises and control groups receiving no intervention for the prevalence of shoulder pain (27, 30, 32, 33). Only one RCT (n =178) of low methodological quality reported a statistically significant difference favouring the exercise group for the reduction in the prevalence of reported soreness in the shoulder in the past week (37).
Four RCTs (n = 1,474) evaluated the efficacy of workplace exercises on function using various functional outcome measures. In the study by Andersen et al. (18, 22, 24), the 3 exercise groups performing different regimens of upper extremity strengthening exercises showed a statistically significant difference of 4.0 points (0–100 scale) (95% CI 2.0–7.0) over the reference group receiving no intervention for the Disability of the Arm, Shoulder and Hand (DASH) questionnaire.
Three other studies (n = 901) of low methodological quality did not observe any significant treatment effect of workplace exercise compared with a control intervention in terms of function, work ability or duration of sick leave (19, 27, 30).
Two trials (n = 576) (25, 27) that compared a workplace-based exercise programme with a control intervention also compared therapeutic exercises with a psychosocial intervention consisting of stress management training (25) or cognitive behavioural training (27) on a population of symptomatic and asymptomatic workers. No statistically significant differences between groups were observed in terms of improvement of shoulder symptoms in the study by Horneij et al. (25) or in terms of reduction in prevalence of shoulder pain in the study by Jorgensen et al. (27). There were also no statistically significant differences between the psychosocial intervention group and the control group on all these outcomes (25, 27).
One RCT with a of high risk of bias (n = 164) compared, in office workers with and without shoulder pain, an ergonomic intervention consisting of an evaluation by an occupational medicine specialist followed by workstation modifications to a workplace-based exercise programme consisting of stretching exercises of the upper limb (31). Statistically significant reductions in the prevalence of shoulder complaints were observed in both groups following the interventions (p < 0.05; 20% reduction in the ergonomic group compared with a decrease of 30% in the exercise group). The between-group difference was, however, not statistically different (p = 0.24).
Six RCTs of low methodological quality compared an ergonomic intervention consisting of specific workstation modifications with a control group that received only general ergonomic education, a brochure or no intervention in a mixed cohort of workers with or without shoulder pain (17, 21, 28, 34, 38, 39).
Pooling of data was possible for 5 studies of low methodological quality (n = 2,148) (Fig. 4) (17, 21, 34, 38, 39). The follow-up ranged from 1 month to 1 year in these trials and the results presented a statistically significant difference favouring the ergonomic intervention over the control interventions for the reduction in the prevalence of shoulder pain with a pooled risk ratio of 1.88 (95% CI 1.20–2.96).
Fig. 4. Forest plot of pooled studies comparing an ergonomic intervention to a control intervention for reduction in prevalence of shoulder pain. Reduction in prevalence of shoulder pain according to group allocation is presented for each study. Blue squares represent risk ratios and the black diamond is the pooled risk ratio with 95% confidence intervals.
The study by Ketola et al. (28) that included only symptomatic workers could not be pooled with other studies and was therefore analysed qualitatively. At the 2-month follow-up, only the ergonomic intervention group showed a statistically significant improvement in shoulder pain intensity (p < 0.05) compared with the ergonomic education group and the control group receiving a pamphlet on musculoskeletal health. However, at the 10-month follow-up no significant between-group differences were observed (p ≥ 0.05).
The low methodological quality RCT by King et al. (29) compared the efficacy of a biofeedback vibrating computer mouse with a non-vibrating mouse (n = 23) for the reduction in shoulder pain in office workers with or without shoulder pain. The mean change in shoulder pain reached statistical significance for between-group comparisons (p < 0.05) in favour of the “vibrating mouse” group at week 25 with a difference of 1.52 ± 0.27 on 10-cm VAS.
The trial by Galinsky et al. (23) of low methodological quality compared 2 different schedules of rest breaks in workers working as data-entry operators (n = 42). One group had a regular rest break schedule with a 15-min break, twice per 8.5-h shift, whereas the other group had supplementary rest breaks of 5 min every hour in addition to the regular breaks. At 16 weeks, a significant difference in pain intensity was observed between groups in favour of the supplementary breaks group (p < 0.01).
A study of low methodological quality by Cheng et al. (20) (n = 94) compared a clinic-based intervention with a workplace-based intervention on workers with rotator cuff tendinopathy. The clinic-based group received work simulation exercises in a clinical setting while the workplace-based group received biomechanics and ergonomic education in their work environment. Both groups received a shoulder exercise programme. On the Shoulder Pain and Disability Index (SPADI; range 0–100), a significant between-group difference was observed with a mean improvement of 13.8 ± 2.9 in the clinic-based group compared with 20.6 ± 4.9 in the work-based group (p = 0.03). A significantly higher percentage of workers returned to work in the work-based group (71.7%) compared with the clinic-based group (37.5%) at the 4-week follow-up (p = 0.001).
Twenty-two RCTs were included in this systematic review and meta-analysis and the methodological quality varied from low to high with a mean quality score of 55.1 ± 11.4%.
Efficacy of workplace exercises
Based on a meta-analysis that included 5 RCTs in which symptomatic and asymptomatic workers were enrolled, there is low-grade evidence that an exercise programme performed in the workplace is more effective than a control intervention to decrease the intensity of shoulder pain (MD 0.46 (95% CI 0.24–0.69)); however, the treatment effect is small and not clinically important (30, 33, 35, 36, 40). Based on a secondary meta-analysis that included only workers with shoulder pain at baseline, we can conclude that there is low-grade evidence that an exercise programme is more effective than a control intervention to reduce shoulder pain (MD of 1.31 (95% CI 0.86–1.76)) (26, 35, 36, 40). This result may be considered clinically important since the confidence interval covers the reported minimal clinically important difference (MCID) of 1.4 cm for a 10-cm VAS specific to rotator cuff disorders (41). However, 5 RCTs of low to high methodological quality analysed qualitatively and not included in the pooled analysis suggest that a workplace-based exercise programme may not be effective to reduce the overall prevalence of shoulder pain in groups of symptomatic and asymptomatic workers. These results, taken together, suggest that workplace-based exercise programmes may be more effective to reduce the intensity of shoulder pain in symptomatic workers than to prevent it in healthy workers. More studies that isolate the preventive or therapeutic effects of exercise programmes are therefore needed before definitive conclusions may be drawn. The type of exercise prescribed may also play a role in the heterogeneous effects observed in the included studies; the majority of RCTs showing a positive effect in our review (6 out 8) included strengthening exercises for the shoulder and the upper limb, but we were unable to pool these studies into a meta-analysis to confirm that assumption.
Our results and conclusion are overall comparable to those of a systematic review by Lowe et al. on the efficacy of workplace-based exercise for the neck and shoulder region. The authors concluded that there was moderate evidence supporting specific workplace-based strengthening to treat work-related neck and upper extremity pain. Several other systematic reviews have reported the efficacy of exercises as a treatment for shoulder pain in adult populations (42–44). As stated by the authors, one possible advantage for delivering the intervention in the workplace is that it may increase adherence to treatment and, thereby, the efficacy of the exercise programmes. One trial of moderate methodological quality in our review supports that assumption (20). Another advantage of performing exercises in the workplace is the ability to tailor the exercise intervention specifically to the worker’s tasks. However, surprisingly, none of the studies included in our review specifically tailored exercises. Future RCTs evaluating the effect of exercise programmes in the workplace should therefore aim at evaluating the efficacy of exercises that are tailored to the worker’s needs.
In terms of function and work-related outcomes, 3 out of 4 RCTS of low methodological quality reported non-significant treatment effect for exercises. These results should be interpreted with caution as the outcome measures were heterogeneous and, here again, workers with and without shoulder pain at baseline were included in the same cohorts.
Two other included trials that compared exercise with a psychosocial intervention showed no statistically significant difference between groups for improvement in shoulder pain or for prevalence of shoulder pain (25, 27). Interestingly, the exercise group as well as the psychosocial intervention group were also not significantly different from the control group for these outcomes. These results could again be explained by the cohorts of mixed participants with or without shoulder pain. In this situation, any treatment effect may be more difficult to detect.
Based on our meta-analysis that included 5 RCTs, there is low-grade evidence that an ergonomic intervention is effective for the reduction in the prevalence of shoulder pain with a pooled risk ratio of 1.88 (95% CI 1.20–2.96) (17, 21, 34, 38, 39). However, it is unclear whether the intervention prevented shoulder pain in healthy workers or reduced shoulder pain in those already with shoulder pain, since, as previously mentioned, the authors from the included studies did not report the results separately for symptomatic and asymptomatic workers. Therefore, treatment effects remain unclear in terms of preventive effects and the effects observed could only be the results in the reduction in symptoms for symptomatic workers only. Again, studies focusing only on the preventive or the therapeutic effects of these workplace-based interventions are therefore needed.
Previous systematic reviews by Hoe et al. (11) and Verhagen et al. (45) concluded that there is low-grade evidence that ergonomic modifications does not reduce or prevent work-related upper extremity pain. However, the studies included in these systematic reviews were of poor methodological quality and did not specifically appraise the effects for shoulder pain, but assessed the effect for various upper extremity pain disorders. Moreover, most of the interventions of the included studies in these reviews consisted of a simple workstation adjustment, such as replacing a keyboard or a computer mouse (11, 45), while the studies included in our systematic review compared ergonomic adjustments evaluated and tailored to the worker’s need by a specialist. Ergonomic interventions are complex and workstation modifications may need to be specific to the worker’s environment (46). It may also be that such interventions may have greater effects for workers with shoulder pain than for other musculoskeletal disorders or for certain occupations. More research is needed to fully conclude on this.
Other workplace interventions included in the present review included the efficacy of a vibrating computer mouse in one trial or supplementary rest breaks in another; both interventions showed a statistically significant decrease in shoulder pain at a medium-to-long-term follow-up (23, 29). However, since these results are only in one trial each, it is premature to draw any conclusion on the effectiveness of these interventions and more research is warranted.
This systematic review highlights the relevance of performing specific workplace interventions, such as exercises and ergonomic interventions specifically for workers currently with shoulder pain. Also, since rehabilitation programmes may differ depending on shoulder pathology, it would be interesting to study the efficacy of workplace interventions in different cohorts of workers with specific diagnoses of shoulder disorders as the prognosis and specific therapeutic efficacy may be different.
A complete literature search was performed using 4 major bibliographic databases. The results were pooled and 3 meta-analyses performed to give an overview of the treatment effects for these interventions. No other research design than RCTs, the highest form of evidence, were included in the present review. The methodological quality of the included studies was evaluated rigorously and the inter-rater reliability for the methodological quality appraisal was high to perfect. Our review also has limitations that arise from the included RCTs that had no specific inclusion criteria in terms of shoulder pathology, and the fact that the exercise and ergonomic interventions were very heterogeneous, which limits our conclusions. Moreover, studies often included a mixed cohort of injured and uninjured workers, which limits the ability to differentiate between preventive and therapeutic effects.
In conclusion, low-grade evidence exists that an exercise programme provided in the workplace is an effective modality to reduce shoulder pain intensity in workers. Low-grade evidence exists that workstation modifications are effective to reduce the prevalence of shoulder pain in workers. Further studies comparing different exercise programmes tailored to the worker’s tasks and specific ergonomic interventions on specific working populations are needed to draw firm conclusions on the effectiveness of workplace interventions for the prevention and reduction in shoulder pain and disability.
Funding: Réseau Provincial de Recherche en Adaptation-Réadaptation/ Fonds de Recherche du Québec en Santé (REPAR/FRQS) and Institut de Recherche Robert-Sauvé en Santé et Sécurité au Travail (IRSST).
The authors declare no conflicts of interest.


 Click to show fullsize
Click to show fullsize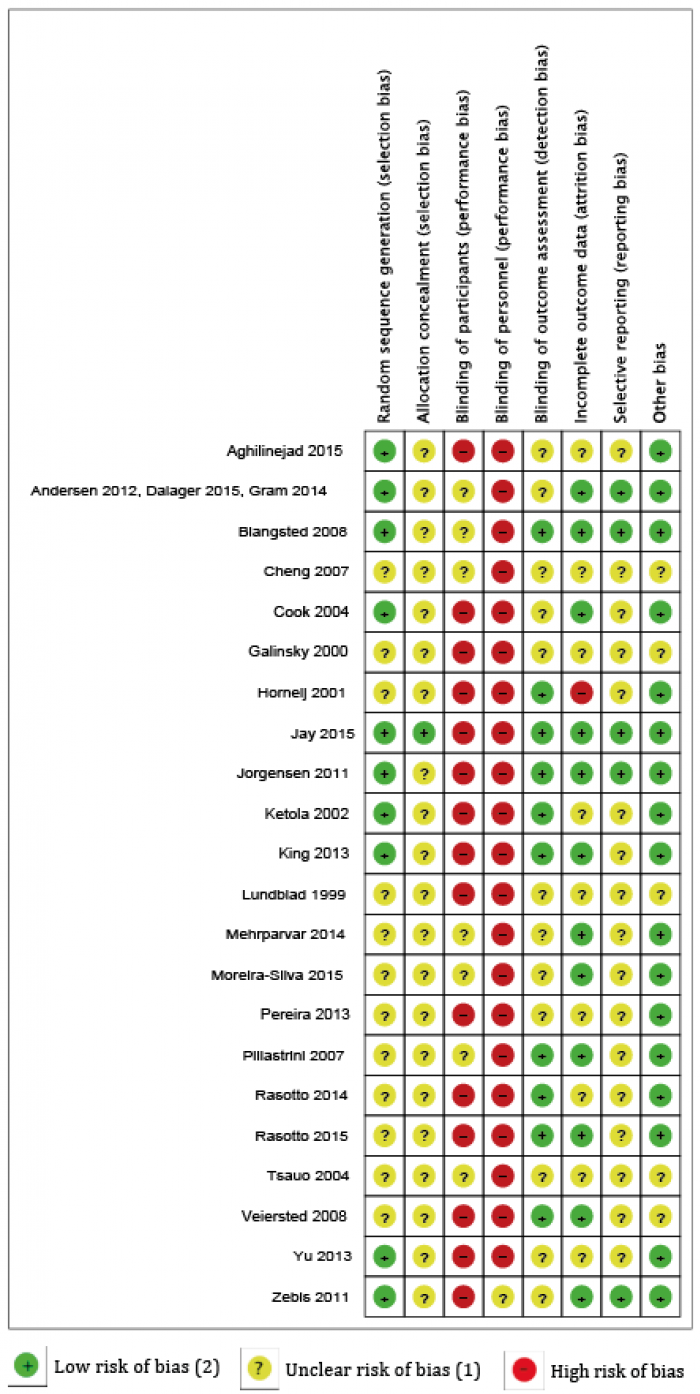 Click to show fullsize
Click to show fullsize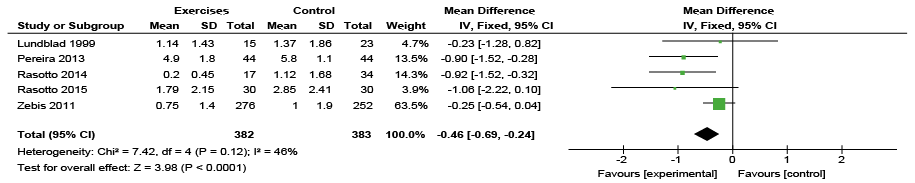 Click to show fullsize
Click to show fullsize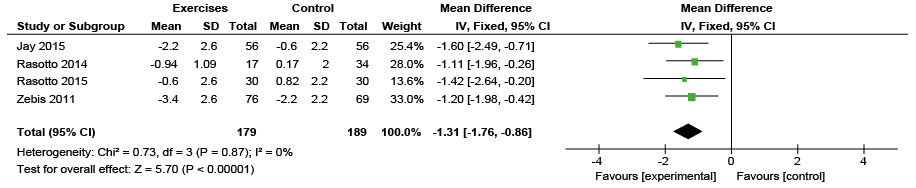 Click to show fullsize
Click to show fullsize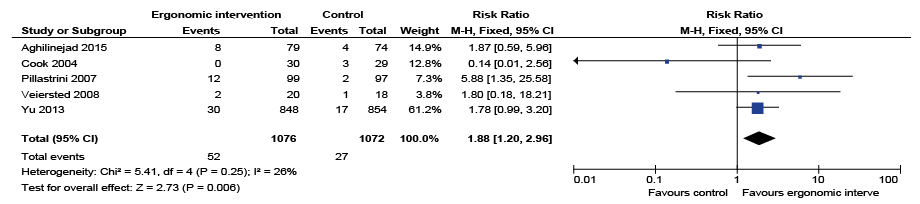 Click to show fullsize
Click to show fullsize