
From the 1Department of Physical Medicine and Rehabilitation, Keçiören Education and Research Hospital, and 2Department of Physical Medicine and Rehabilitation, Gazi University School of Medicine, Ankara, Turkey. The authors contributed equally to this study.
Objective: To investigate the effect on balance control of postural changes related to ankylosing spondylitis.
Design: Thirty-four subjects with ankylosing spondylitis and 34 healthy individuals were enrolled. Examination of postural alignment was conducted using lumbar Schober, hand to ground distance, tragus to wall distance and occiput to wall distance measurements, and Bath Ankylosing Spondylitis Metrology Index. Balance was evaluated by Berg Balance Scale, Functional Reach Test, Lateral Reach Test, and Static Balance Index. Postural sway during quiet standing was assessed by centre of pressure displacement in 2 conditions: eyes open and eyes closed.
Results: Functional reach test and right-side lateral reach tests were significantly lower in subjects with ankylosing spondylitis. Eyes closed anteroposterior centre of pressure sway was significantly higher in the subject group.
Conclusion: Ankylosing spondylitis can lead to balance deterioration due to postural changes.
Key words: ankylosing spondylitis; balance; posture.
Accepted Mar 29, 2017; Epub ahead of print May 4, 2017
J Rehabil Med 2017; 49: 437–440
Correspondence address: Elif Balevi Batur, 29.sk 52/8 Emek/Çankaya/Ankara, PC: 06490 Turkey. E-mail: elifbalevi@hotmail.com
Ankylosing spondylitis (AS) is a chronic, inflammatory rheumatic disease that results in structural deformity and limitation in spinal mobility by affecting the axial skeleton. The main clinical features are fatigue, inflammatory back pain, and joint stiffness. AS leads to some structural and functional impairments. It also results in reduced general health (1). In advanced phases of this disease, flexibility decreases, and the typical kyphotic posture occurs (2, 3). Kyphosis results in difficulty in looking upwards, decreased visual field, and limitation in daily activities, such as communication, driving, going outside, and/or performing personal hygiene (4, 5). This postural malalignment makes it difficult for the body to assume and maintain an optimal position. Consequently, falls may occur due to impairment in balance (6, 7).
Balance is the ability to maintain the body’s centre of gravity within the base of support with minimal postural sway. Balance is a complex function maintained by sensorimotor control systems, including sensory input and neuromuscular responses. Effective motor responses and an intact neuromuscular system are required to return the centre of mass (COM) of the body over the support surface when balance is lost (8). Balance control is important for static and dynamic postures (3). Balance impairment is an important risk factor for falls. Falls and loss of balance most commonly occur during movement-related activities, such as walking and, less frequently, during static activities. In 1994, Maki et al. (9) stated that changes in postural mobility may lead to impaired postural control, which is associated with increased risk of fall.
Identifying the mechanism of balance deterioration due to postural changes in AS might prevent falls in these subjects. Although it is known that postural changes affect balance, there are only a few studies examining balance in subjects with AS (4, 10, 11). As existing studies have inconsistent results, we investigated the impact of postural changes on balance with clinical balance tests and postural sway in subjects with AS.
Thirty-four subjects with AS, diagnosed according to Modified New York Criteria, and 34 healthy individuals applied to the Rheumatology division of Gazi University School of Medicine Physical Medicine and Rehabilitation Department between April 2011 and October 2012 were enrolled into the study. Healthy individuals were selected to match subjects with AS in terms of demographic features, such as age, sex, weight, and body mass index (BMI). Subjects with vision problems, cognitive problems, neurological diseases affecting the balance and the posture, orthopaedic problems interfering with the balance measurements and who were under 20 years and above 65 years, were not included in the study. All assessments were performed by the first researcher (E.B.B.) and completed in a total of 2 h. This study was approved by the local institutional ethics committee and was conducted according to the Declaration of Helsinki as well as local institutional guidelines. All subjects provided written informed consent.
A detailed musculoskeletal system examination was performed, including range of motion at hip and knee joints, Thomas test to evaluate any flexion contracture at the hip joint, measurements of lumbar Schober, hand to ground distance (HGD), tragus to wall distance (TWD) and occiput to wall distance (OWD). The axial status of subjects was evaluated using the Bath Ankylosing Spondylitis Metrology Index (BASMI). Subjects whose OWD is more than 0 cm were categorized as kyphotic (12).
Lateral Reach Test (LRT) were used to evaluate functional balance; Static Balance Index (SBI) was used to evaluate static balance. Postural sway was assessed with Emed®-X system.
The BBS consists of 14 tasks that evaluate the patient’s ability to maintain balance either statically, or while performing different functional movements for a specified duration of time. Each item is scored from 0 to 4, giving a maximum global score of 56 points. The scale takes 10–20 min to complete.
In the FRT, each subject is asked to stand erect with their feet shoulder width apart and reach forward as far as they can, without taking a step. Functional reach is measured as the maximum distance (cm) during the reaching task with the hand and arm, extended and parallel to a measuring stick at shoulder height. This test was repeated 3 times and mean values were used for analysis. The LRT was performed similarly for right and left sides (13, 14).
The SBI was assessed using a Kinesthetic Ability Trainer 3000 (KAT-3000, Med-Fit Systems Inc., Fallbrook, CA, USA). The KAT-3000 is a balance platform designed for training and testing of static and dynamic balance. The SBI quantifies the ability to keep the platform near the reference position. For the static balance test, a low SBI value reflects low postural sway during quiet standing and is interpreted as “good” balance. The static balance test was performed with the subject standing on the platform on both feet, folding their arms across their chest. Subjects stood with the second toe of both feet on the parallel lines to the Y-axis located 10.5 cm away from this axis, and the top of their foot intersecting with the X-axis. Before the test, each person was allowed a 3-min practice period. For the static balance test, they were asked to keep the red “x” sign at the centre of the platform in the centre of the screen for 30 s.
Postural sway was calculated by using the Emed®-X (Novel GmbH, Munich, Germany) system. A standard sample duration of 30 s was selected. Postural sway during quiet standing was assessed by measuring maximal anteroposterior (AP) and mediolateral (ML) displacements of centre of pressure (COP) from COP trajectory with eyes open (EO) and eyes closed (EC). Maximal AP and ML displacement with eyes open (EOAP, EOML) and eyes closed (ECAP, ECML) were measured. A standard distance between the feet was achieved by drawing the foot position on acetate paper, which was placed on the Emed®-X platform.
Sample size justification was not performed at the beginning of the study. The power of the study was calculated based on the results. The post hoc power was calculated as 99% due to the difference in ECAP. The reporting of the present study follows the STROBE (Strengthening the Reporting of Observational Studies in Epidemiology) guidelines, using the checklist for cross-sectional studies (15).
SPSS for Windows version 18.0 software program was used for statistical analysis. Distribution of the variables was assessed by Shapiro–Wilk test. To evaluate the difference between the independent groups, Student’s t-test was used as parametric test and Mann-Whitney U test as non-parametric test. The relationships among variables were described with Spearman’s correlation coefficient. Statistical significance value was accepted as p < 0.05. Bonferroni correction (dividing alpha level by number of tests) was used to counteract the problem of multiple testing. There were no missing data in this study.
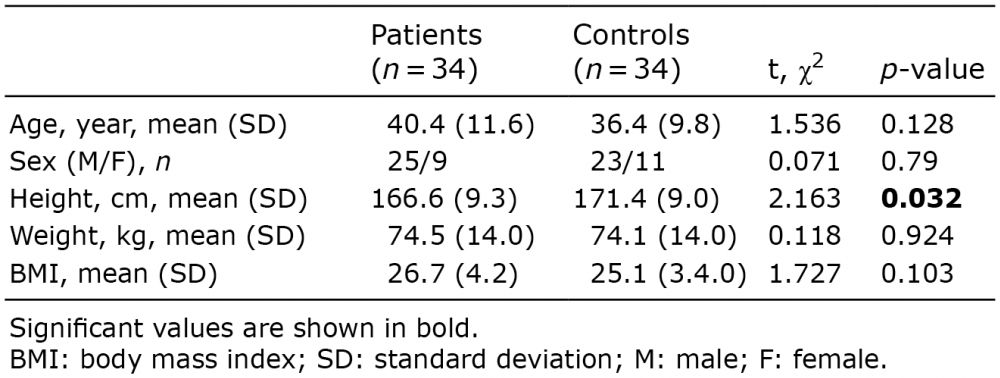
The demographic and anthropometric features of the subjects are shown in Table I. The only statistically significant difference between the 2 groups was their height (p < 0.05). The values for the lumbar Schober, HGD, TWD and OWD measurements in the patient group ranged from 0.5 to 7 (median 3) cm, from 0 to 50 (median 18.5) cm, from 9 to 28 (median 18) cm and from 0 to 19 (median 4.5) cm, respectively. The median BASMI score was 4.5 (0–19).
Table I. Demographic and anthropometric features of the patient and the control groups
FRT and LRT on the right side were worse in the subject group. The differences between groups were statistically significant (Table II). Postural sway parameters with eyes open and eyes closed are shown in Table II for both groups. ECAP sway was found to be significantly higher in the subject group (p < 0.001).
Table II. Balance measurements and postural sway parameters for the patient and control groups
Kyphosis was found in 29 (85%) subjects. Hip and knee flexion contracture was found in 3(8.8%) and 11 (32.4%) subjects, respectively. The median values of the spinal mobility measurement values, balance tests and postural sway parameters of the subjects with and without kyphosis in the subject group are summarized in Table III. Statistically significant differences between the 2 groups were found for TWD and BASMI score (p < 0.001 and p = 0.001, respectively).
Table III. Median values of the spinal mobility measurements, balance tests and postural sway parameters of the patients with and without kyphosis
The results of correlation analyses among tests of balance and postural alignment are shown in Table IV. EOAP and ECAP COP sway were positively correlated with OWD (Table IV).
Table IV. Correlation analyses (r values) of balance tests, postural sway and spinal mobility parameters in the patient group
In this study, clinical tests and force platform variables were used to evaluate the balance of subjects with AS. FRT, LRT on the right side, and ECAP displacement were found to be different between subjects with AS and the healthy individuals. TWD and BASMI scores were significantly different in subjects with kyphosis compared with non-kyphotic subjects. In accordance with these results OWD was found to be correlated with anteroposterior COP sway. These results suggest that postural changes associated with AS could lead to balance problems.
Postural control or balance is a complex process that requires interactions between musculoskeletal, sensory, and cognitive systems (14). Considering the pattern and natural course of the disease in AS, the postural malalignment component of this complex process might lead to deterioration of balance. The results of the present study also suggest that postural and specific proprioceptive exercises should be added to rehabilitation programmes of subjects with AS to improve their balance in various conditions.
Limitation in spinal mobility is the fundamental finding in AS. Lumbar lordosis becomes flattened and thoracic kyphosis increases. Spinal kyphosis causes a forward and downward shift of COM with respect to the base of support. Because of the spinal column stiffness, subjects try to achieve postural control by compensation with dorsiflexion of the ankle and flexion of the knee (16). Although there are many studies concerning pain relief, spinal stiffness and joint problems in AS, studies investigating AS-related postural changes and balance disorders are rare.
In a study by Vergara et al. (10), eyes open and closed COP sway was evaluated in subjects with AS. Postural sway of the patient group was found to be higher than the control group in frontal and sagittal planes. Subjects with AS demonstrated a significant increase in frontal plane net COP displacement in the eyes-closed condition (9). Our study used similar methods and similar results. In addition to the force platform indicators of balance, our battery of clinical balance tests and SBI found balance deficits in subjects with AS.
In contrast, Aydog et al. (4) evaluated dynamic standing balance in subjects with AS with Biodex Stability System (3) and found that AS did not have a negative effect on postural stability. However, Aydog et al. (4) used the “eyes open” condition in the aforementioned study.
Murray et al. (11) investigated the horizontal displacement of hip movements with eyes open and closed position, using sway magnetometry. Balance impairment ratios have been found in 3% of healthy individuals in eyes open and closed positions, whereas these ratios were 18% and 23%, respectively, in the subjects with AS. Although they stated that the number of subjects with AS with poor balance for both conditions was significantly greater than expected, they did not find significant difference between subjects with AS and healthy individuals. Unlike that study, authors in this study assessed postural sway with Emed®-X system and found statistically significant difference between subjects and healthy controls for anteroposterior COP sway with eyes open and eyes closed conditions. A positive correlation was determined between EOAP, ECAP COP sways and spinal mobility parameters in the patient group. The increased postural sway in the sagittal plane caused by anterior displacement of the COM as a result of the kyphotic posture, might cause a balance impairment in AS. This study suggests that subjects with AS have a significant increase in postural sway in the sagittal plane. Also, spinal stiffness might lead to impaired postural control.
One of the limitations of this study was that there were no subjects with contractures. If the subjects with peripheral involvement, such as hip contracture, had been included, differences due to impaired manoeuvres of the affected hip could have been detected.
Another limitation of our study is that BBS in the control group has zero variability as all subjects’ scored maximum points. Thus we could not evaluate differences between the groups. In addition, according to observations during the tests, pain could have a negative impact on performance in balance tests and postural sway. Considering this observation, not to assess the pain intensity could be another limitation of this study. Thus, future research is needed to identify the relationship of the pain with these parameters.
In conclusion, this study shows that subjects with AS have poorer balance than healthy subjects matched for age, sex, weight, and BMI. In advanced stages of AS, the increase in kyphosis could lead to impairment in anteroposterior stability, increase in COP sway displacement and deteriorated balance. Larger study groups with more subjects with joint contractures are required to detect such a relationship.
The authors declare no conflicts of interest.


 Click to show fullsize
Click to show fullsize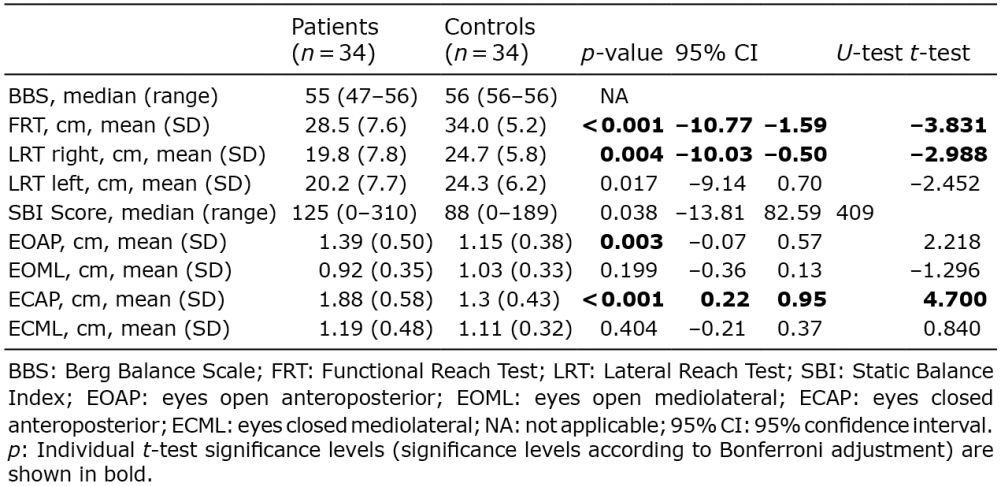 Click to show fullsize
Click to show fullsize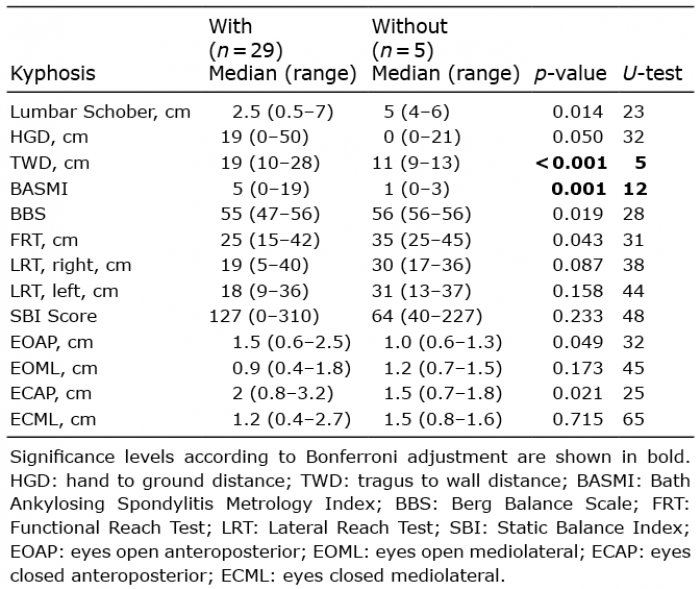 Click to show fullsize
Click to show fullsize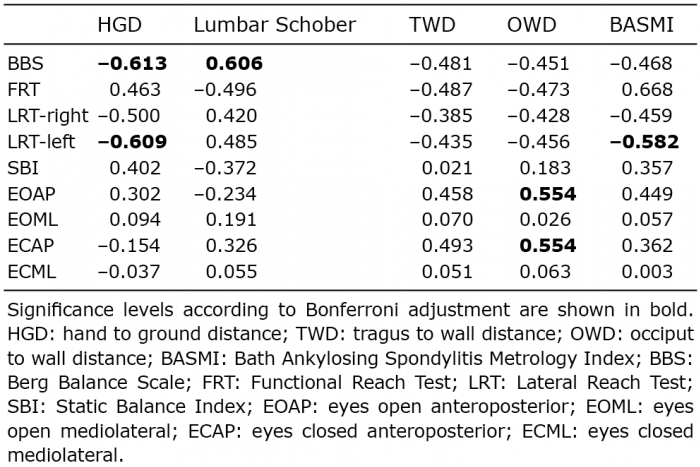 Click to show fullsize
Click to show fullsize