
From the Department of Pediatric and Adolescent Medicine, Mayo Clinic, Rochester, MN, USA
Objective: Chronic fatigue and chronic pain both deter people from participating in exercise, even though exercise is often a key component of treatment. While reasons for this may seem obvious, the extent and mechanism(s) of reduced exercise performance among affected individuals, particularly those with chronic pain, are not well described. We hypothesized that patients with chronic fatigue are more deconditioned than those with chronic pain, due to the nature of their illness or disability.
Design: Retrospective chart audit June 2012 to December 2014.
Subjects: Adolescents with chronic fatigue (320, 73 males) or chronic pain (158, 30 males).
Methods: Maximal cardiopulmonary exercise test to determine peak oxygen uptake (V?O2) and work efficiency.
Results: Mean (standard deviation (SD)) peakV?O2 was similar between patients with chronic fatigue and chronic pain: males 36.5 (SD 8.3) vs 34.2 (SD 7.3) ml/kg/min (p = 0.17); females 27.3 (SD 6.1) vs 27.6 (SD 6.6) ml/kg/min (p = 0.67). PeakV?O2 was < 90% predicted in 80% and 75% of females, or 77% and 83% of males, with chronic fatigue and
chronic pain, respectively. Peak O2pulse and work efficiency were likewise similar.
Conclusion: Patients in both groups manifest exercise responses typical of cardiopulmonary deconditioning and to similar extent. Failure to detect unique cardiopulmonary or muscle pathophysiology suggests a shared pathway to low aerobic work capacity.
Key words: chronic pain; chronic fatigue; deconditioning; oxygen consumption; work efficiency.
Accepted Feb 3, 2017; Epub ahead of print May 4, 2017
J Rehabil Med 2017; 49: 441–446
Correspondence address: Paolo T. Pianosi, 200 First St. SW, Rochester MN, 55905, USA. E-mail: paolo.pianosi@nhs.net
Fatigue is common in adolescence: population-based studies indicate that 1.2% of American adolescents reported fatigue ≥ 6 months’ duration, whereas only ~0.34% met the criteria for chronic fatigue syndrome (CFS) (1). A Dutch study found that 9.6% of girls and 2.3% of boys were troubled by fatigue ≥ 3 months’ duration (2). Chronic fatigue (bothersome fatigue for at least 3 months) and CFS (bothersome fatigue in patients who meet the 1994 definition (3)) are both associated with decreased exercise tolerance. The definition of CFS has varied over time, but has invariably included substantial reduction or impairment in ability to engage in pre-illness levels of activities, plus post-exertional malaise (4, 5). Patients with chronic fatigue often have multiple co-morbidities (6–8), but almost universally have lower exercise capacity than their healthy peers. Lower peak oxygen uptake (V?O2) and peak work capacity were found in Dutch adolescents with chronic fatigue compared with normal reference values (9). A US study also reported lower peak V?O2, but similar peak work capacity in patients with CFS following infectious mononucleosis compared with “controls” (10). Thus, oxygen cost of work (ΔV?O2/ΔW) was lower in chronic fatigue patients, contradicting an earlier report of greater metabolic cost for the same external work in subjects reporting excessive exertional fatigue (11).
Chronic (i.e. persistent or recurrent) pain affects 20–35% of children and adolescents (12, 13), substantially more than the prevalence of chronic fatigue. Young people with chronic pain may also tend to withdraw from physical activity, like those with chronic fatigue. Although the relationship between chronic pain and physical activity is complex (14), in general adolescents with chronic pain are less active than healthy peers, documented both objectively via actigraphy and subjectively by reports of reduced physical functioning (15, 16). Thus, individuals with either chronic fatigue or chronic pain may succumb to the vicious cycle of inactivity–deconditioning. Our literature search revealed only 2 studies of children and adolescents with non-arthritic, musculoskeletal pain: one reporting lower z-scores for peakV?O2 (17); and another reporting peakV?O2 before and after intervention (18). It had been proposed that ΔV?O2/ΔW, which reflects muscle perfusion and O2 extraction during exercise, may be altered in fibromyalgia, although normal ΔV?O2/ΔW was found in a study of adults with fibromyalgia (19).
Adolescents presenting to Mayo Clinic with chronic fatigue, musculoskeletal pain, chest pain, abdominal pain, or chronic daily headache, routinely undergo maximal exercise testing. We audited these results to compare and elucidate their cardiac response to exercise. Our primary hypothesis was that deconditioning is greater, i.e. lower peakV?O2, in patients with a chief complaint of chronic fatigue compared with those with chronic pain. Deconditioned patients were expected to manifest typical changes of cardiovascular deconditioning, i.e. small heart that beats rapidly to meet exercise demands. A secondary hypothesis was that ΔV?O2/ΔW would differ between patients with chronic fatigue compared with those with chronic pain if post-exertional malaise in CFS were explained by greater O2 cost of mechanical work.
We conducted a retrospective audit of medical records of adolescents (12–19 years of age) seen in the Mayo Pediatric Diagnostic and Referral Clinic between June 2010 and December 2014 with symptoms of chronic fatigue of at least 6 months’ duration, dizziness, abdominal discomfort (nausea or pain), or other pain (headache, myalgia or arthralgia) and who had both undergone autonomic reflex testing (to exclude postural orthostatic tachycardia syndrome) and maximal cardiopulmonary exercise test. Patients with alternative medical diagnoses were excluded. Testing was conducted for clinical indications and therefore informed consent was not required. Patients were included in this study, and their medical records reviewed, if the patient had not denied access to their medical records for research purposes in accordance with a research authorization statute for the state of Minnesota. Mayo Clinic Institutional Review Board approved the study.
Patients performed a symptom-limited, maximal cycle ergometer exercise test according to the Godfrey protocol with 1-min incremental steps of increasing work (20). Gas exchange was measured breath-by-breath at rest and throughout exercise using a MedGraphics CPX/D (Medical Graphics Corp, St Paul, MN, USA). Blood pressure was measured by auscultation at rest, during warm-up (initial workload) then every other workload, with continuous monitoring of 12-lead electrocardiogram (ECG) throughout the test. Work increments were chosen in order to achieve test duration somewhere between 9 and 15 min. Patients were strongly encouraged to exercise to voluntary exhaustion, but given their chronic fatigue, some patients failed to achieve criteria for a maximal effort: heart rate (HR) > 185 bpm, respiratory gas exchange ratio > 1.1 at peak exercise. They were classified as deconditioned. PeakV?O2 was determined as the highest achieved V?O2 averaged over 30 s and expressed as percent predicted (21). James’ normal values are computed based on sex, body surface area, and standing height, yielding values in l/min. Work efficiency was calculated by linear regression of work (W) vs V?O2 (?V?O2/?W). Oxygen pulse was calculated as V?O2/HR. These 3 (peakV?O2, ?V?O2/?W, and V?O2/HR) were the primary exercise outcome variables.
Patients were stratified into clusters according to their chief complaint: fatigue (with or without dizziness), headache, abdominal pain or nausea, and musculoskeletal pain, in which group we included individuals with chest pain (adolescent costochondritis). Preliminary analyses showed no difference in outcomes of interest (?OV?2/?W, peakV?O2, and peak O2pulse) between those with chronic headache, abdominal pain/nausea, or musculoskeletal pain. They were therefore combined into a unified chronic pain group for comparison with the chronic fatigue group. Analyses were stratified by sex since exercise measurements are known to differ between adolescent males and females. Each exercise outcome measurement was compared between patients with chronic fatigue vs chronic pain, based on fitting a separate linear regression model. Additional models were fit adjusted for age and haemoglobin (Hgb) as potential confounders, and adjusted least-square means are reported for the exercise outcome measurements. All tests were 2-sided and p-values < 0.05 were considered statistically significant. Statistical analysis was performed with SAS 9.3 (SAS Institute, Cary, NC, USA).
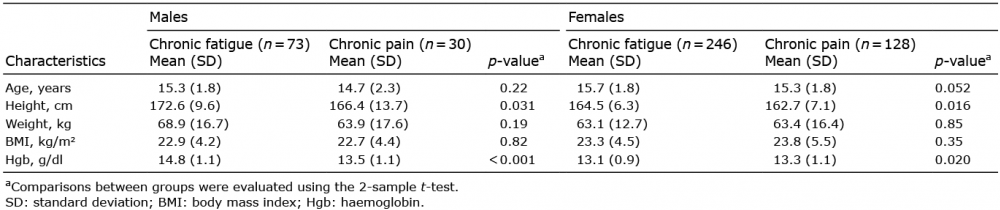
Anthropometric data for the 319 patients with chronic fatigue and the 158 with chronic pain are shown in Table I. Symptoms at the time of initial presentation included fatigue (100%), dizziness (90%), headache (70%), nausea or abdominal pain (48%), and other pain, e.g. chest, muscles, joints (49%). Females who presented with chronic fatigue had marginally lower mean Hgb, whereas among males presenting with chronic fatigue mean Hgb was slightly higher.
Table I. Subject characteristics
Overall mean peak HR during exercise was 187 standard deviation (SD 11) beats/min, well within expected range for maximum effort, although 20% of patients with chronic fatigue and 22% of patients with chronic pain did not reach the 180 beat/min threshold. Most patients were deconditioned, but as there is no agreement as to what constitutes low peakV?O2 in adolescents, we display frequency histograms of peakV?O2 values, separately by sex and grouped into pain or fatigue patients (Fig. 1). PeakV?O2 was < 90% predicted in 80% and 75% of females, or 77% and 83% of males, with chronic fatigue and chronic pain, respectively.
Fig. 1. Frequency distribution histograms of primary outcome variable, peakV?O2. Note that abscissae and ordinates differ in scale between females and males.
Table II shows peak exercise data for all patients. Absolute peakV?O2 (l/min) and peak work capacity were higher in males with chronic fatigue compared with males with chronic pain, though these differences disappeared when peakV?O2 was normalized as a percentage of predicted value or subject’s weight; or if work was expressed as a percentage of predicted value.
Table II. Peak exercise data. Comparisons between groups based on fitting two separate general linear one models adjusted and another unadjusted for age and haemoglobin, from which adjusted least-square means reported
Peak O2pulse was also lower in males with chronic pain vs those with chronic fatigue, but both peak O2pulse and peakV?O2 (l/min) were not significantly different after adjusting for age and Hgb values between the 2 groups: adjusted mean peakV?O2 2.41 vs 2.24 l/min (p = 0.20); adjusted mean peak O2pulse 12.9 vs 11.7 ml/beat (p = 0.10). No differences were found in exercise variables of interest among females. Box plots comparing the distribution of the work efficiency and peak O2 pulse between chronic fatigue vs chronic pain patients segregated by sex are shown in Fig. 2.
Fig. 2. Box and whisker plots of work efficiency (?V?O2/?W) and peak O2pulse (V?O2/HR), showing females on left and males in right panels. p-value shown in top-right corner of each.
These data on aerobic fitness and work efficiency during incremental exercise to volitional limit comprise the largest reported cohort of adolescents with chronic fatigue. As expected, most patients had low peakV?O2 and peak O2pulse, typical findings of classic cardiac deconditioning. Furthermore, exercise performance in patients with chronic pain was very similar, implying there is nothing unique or distinguishing with respect to circulatory response to exercise or peak aerobic capacity between patients with chronic fatigue and those with chronic pain, be it cranial, musculoskeletal, or abdominal. We failed to prove our primary hypothesis, but the histograms shown provide insight into both prevalence and severity of deconditioning in these populations.
The deconditioned state results in changes at the muscular level (22) that could lead to altered work efficiency, and conceivably cause fatigability and post-exercise malaise. However, ?V?O2/?W was normal (23) in patients with chronic pain or chronic fatigue, both suggesting neither alterations in the pathway for oxygen to muscle nor biomechanical efficiency play a role in either condition. Thus, we could not confirm our secondary hypothesis.
We found only 2 studies of peak work or aerobic capacity in paediatric patients with chronic fatigue. Takken et al. reported lower HR and V?O2 at peak exercise in 20 children and adolescents with CFS compared with normal reference values in a Dutch population (9). Katz et al. examined exercise responses in a well-defined, prospective, cohort of adolescents with post-infectious chronic fatigue compared with matched “controls” who recovered from infectious mononucleosis (10). PeakV?O2 values in their patients were similar to those from the Dutch study; but peakV?O2 and peak O2pulse were higher in recovered “controls”, indicating lower fitness in those whose fatigue persisted ≥ 6 months after illness. Mean peak O2pulse and V?O2 values were lower in our patients compared with either of these reports, perhaps due to greater duration of symptoms in our patients (~2.5 years). Oxygen pulse (V?O2/HR) can be thought of (within certain limitations) as a surrogate measure for stroke volume during exercise, according to the Fick equation:
Low O2pulse implies low SV, which combined with relative tachycardia, are hallmarks of classical cardiovascular deconditioning.
The most common chronic pain conditions in a paediatric population are musculoskeletal pain, abdominal pain, and headache (24), identical to constituents of our heterogeneous study population. We amalgamated patients with different primary pain localization into a single group since results of maximal exercise tests were very similar. There are conflicting findings among the plethora of studies describing aerobic fitness parameters in adults with fibromyalgia (19, 25). We found only 2 reports of peakV?O2 determination in paediatric patients with chronic pain, both non-arthritic, musculoskeletal. An intervention trial of exercise training in adolescent patients with fibromyalgia found pre- and post- peakV?O2 values below generally accepted norms (18), similar to those seen in Fig. 1. Lower z-scores for peak work and V?O2 attributed to deconditioning were found in paediatric patients with joint hypermobility and non-specific musculoskeletal pain (17). We are aware of no similar studies in paediatric patients with chronic abdominal or chest pain, or headache. The fact is that many children and adolescents report more than one pain (26) and we thus felt justified combining our patients with musculoskeletal, abdominal, or cranial pain into a single group for purposes of analysis. Patients in both groups pushed themselves equally to volitional limits during the maximal test (Table II), and findings support such an amalgam a posteriori.
The distinction between chronic fatigue, as defined in the introduction, and CFS is somewhat artificial and contrived, in as much as patients who believe their fatigue is associated with more severe consequences, or will last longer and accounts for more additional symptoms, are more likely to be classified as CFS; while patients who are more physically active and adopt a behaviour pattern characterized by vigorous activity followed by rest (in contrast to limited activity in favour of accruing more time resting) are less likely to be classified as having CFS (27). The issue is more complex than simply choosing to refrain from exercise. One study found similar activity levels reported by adolescents with CFS and matched controls (28); whereas another found that days spent in bed since the onset of infectious mononucleosis was a predictor of subsequent chronic fatigue (29). Similarly, there is overlap in clinical presentation of patients with chronic fatigue and chronic pain, fibromyalgia being the entity most studied (30–32). Comorbidities, such as headache and irritable bowel syndrome, are common in chronic fatigue, but most of our adolescent patients reported nausea or abdominal pain rather than diarrhoea or constipation. We separated our patient population per their chief complaint(s) after thorough chart reviews, but despite this distinction, conflation of patients with chronic pain and chronic fatigue or CFS is inescapable. Our findings indicate that chronic pain and chronic fatigue patients are similarly deconditioned, and as such, one may postulate that deconditioning is a final common pathway in both chronic pain and CFS (33). Rather than being separate entities, albeit heterogeneous, they may share common pathophysiology, such as central sensitization to various afferent impulses (34). There were individuals in both the chronic fatigue and chronic pain groups who achieved respectable peakV?O2 values (Fig. 1). Thus, perceptual responses affecting symptom awareness trump objective performance in these individuals (35). Exercise tolerance and termination during an incremental test to maximal effort (such as we employed) is influenced by the pre-frontal cortex (36), a motivational factor that is difficult to estimate or measure.
Exercise is promulgated as effective therapy in both chronic fatigue (37) and chronic pain (38) states, which benefits may be greater in younger vs older participants (39). Guidelines for exercise prescription are not well established, but it is generally guided by the patient’s report of symptoms, specifically of a prolonged post-exertional exacerbation of fatigue characteristic of the condition. Thus, training effects may accrue slowly or the patient may reach a ceiling too readily in order to avert (fear of) sustained exacerbation of symptoms and functional decline. A scale was very recently described to capture this constituent symptom in order to document response to graded exercise therapy (40), which ought to enable some quantification of this facet. Our relatively large and statistically powerful data on key outcome variables, such as peakV?O2, O2pulse, and work efficiency, provide an excellent springboard for large, multicentre trials on exercise as medicine in patients with chronic fatigue or chronic pain.
There were several limitations of our study. While this was a retrospective review without a control group, our purpose was not to compare these patients with healthy controls but to describe aerobic parameters of, and circulatory response to, cycle ergometry to see if there were differences between patients with chronic fatigue vs those with chronic pain. Virtually all reported reduced physical activity (most doing very little in this regard) and were schooled at home, but we made no attempts to quantitate this during clinic visits. Thus, we cannot determine whether any threshold with respect to degree of inactivity was a determinant of their response to exercise. Since all patients had fatigue ≥ 6 months, symptom duration ought not account for differences in cardiac responses between fit and unfit. It is recognized that immobilization longer than 4 weeks results in large increases in (muscle) fatigability linked to loss of oxidative capacity (41). Blood sampling was not routine, but it would have been worthwhile to measure lactate during exercise in these patients. We failed to routinely have patients rate dyspnoea or perceived exertion, an oversight which may have shed light on why some patients achieved a healthy peakV?O2 yet still complained of chronic pain or fatigue. Equally, if not more important, was omission of post-exercise follow-up, i.e. we did not survey patients 24 h afterwards to enquire about post-exertional malaise. However, this criterion was elaborated only in the most recent guidelines for systemic exertion intolerance disease (5), after our data had been collected.
In conclusion, most adolescents with chronic fatigue or chronic pain are deconditioned, and have low peak O2pulse; a manifestation of cardiovascular sequelae of prolonged inactivity. A minority in both groups presumably maintained a healthy stroke volume response to exercise and achieved normal peakV?O2 nonetheless. Oxygen cost of work was ~9 ml/watt, marginally lower than the 10 ml/watt usually quoted for exercise below the ventilatory anaerobic threshold, but well within normal limits (23). Our inability to demonstrate altered ?V?O2/?W implies O2 delivery to and utilization by exercising muscle is appropriate. We found no unique mechanism(s) to explain the similarly reduced peakV?O2 in adolescents with chronic fatigue or chronic pain other than deconditioning, though we cannot exclude cortical/volitional influences perhaps prompted by altered perceptual responses to vigorous activity.
This research was supported by unrestricted grants from the American Dysautonomia Institute and the Hohmann Foundation. Authors thank Patricia Ervin, MLS, for her assistance with the literature search.
The authors declare no conflicts of interest.


 Click to show fullsize
Click to show fullsize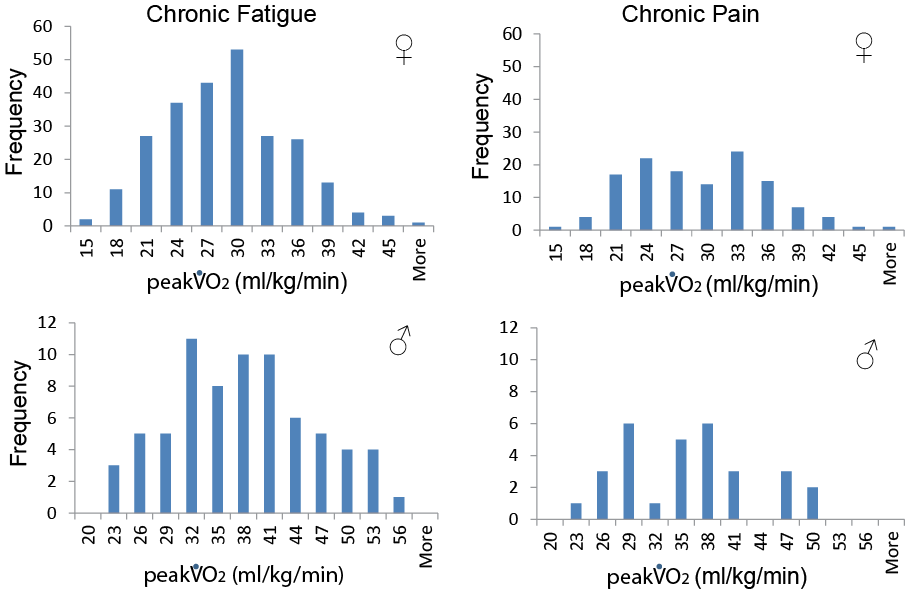 Click to show fullsize
Click to show fullsize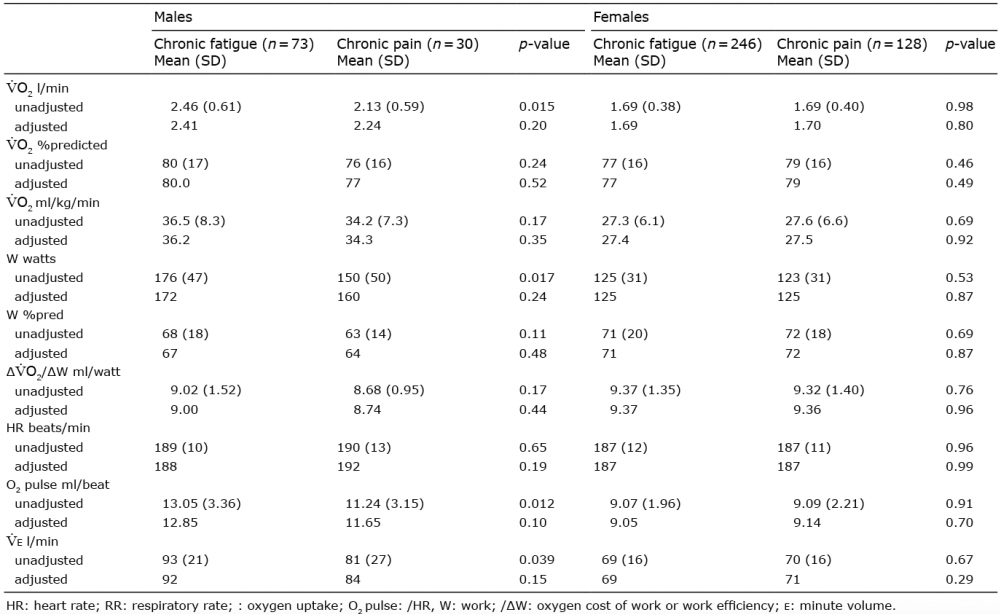 Click to show fullsize
Click to show fullsize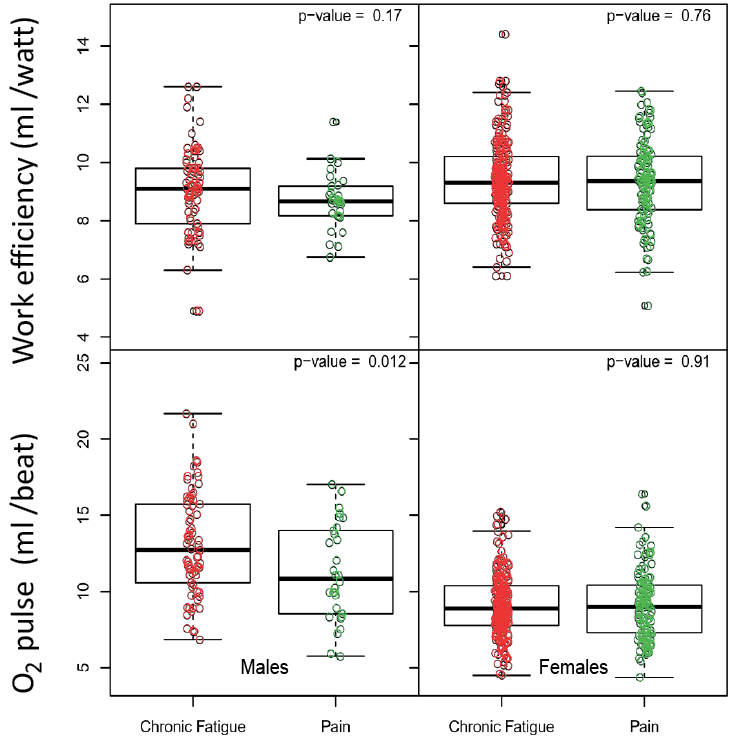 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize