
From the 1Center for Medical Decision Sciences, Department of Public Health, Erasmus Medical Center, Rotterdam, The Netherlands, 2Turku University Hospital, Department of Rehabilitation and Brain Trauma, Division of Clinical Neurosciences, 3University of Turku, Department of Neurology, Turku, Finland, 4Department of Neurosurgery, Antwerp University Hospital and University of Antwerp, Edegem, Belgium, 5Division of Anaesthesia, University of Cambridge/Addenbrooke’s Hospital, Cambridge, UK, 6Rijndam Rehabilitation Center, and 7Department of Rehabilitation Medicine, Erasmus MC, Rotterdam, The Netherlands
Objective: To describe variation in structural and process characteristics of acute in-hospital rehabilitation and referral to post-acute care for patients with traumatic brain injury across Europe.
Design: Survey study, of neurotrauma centres.
Methods: A 14-item survey about in-hospital rehabilitation and referral to post-acute care was sent to 71 neurotrauma centres participating in a European multicentre study (CENTER-TBI). The questionnaire was developed based on literature and expert opinion and was pilot-tested before sending out to the centres.
Results: Seventy (99%) centres in 20 countries completed the survey. The included centres were predominately academic level I trauma centres. Among the 70 centres, a multidisciplinary rehabilitation team can be consulted at 41% (n = 29) of the intensive care units and 49% (n = 34) of the wards. Only 13 (19%) centres used rehabilitation guidelines in patients with traumatic brain injury. Age was reported as a major determinant of referral decisions in 32 (46%) centres, with younger patients usually referred to specialized rehabilitation centres, and patients ≥ 65 years also referred to nursing homes or local hospitals.
Conclusion: Substantial variation exists in structural and process characteristics of in-hospital acute rehabilitation and referral to post-acute rehabilitation facilities among neurotrauma centres across Europe.
Key words: brain injuries; rehabilitation; health services research; survey; Europe.
Accepted Jan 27, 2017; Epub ahead of print Apr 21, 2017
J Rehabil Med 2017; 49: 00–00
Correspondence address: Maryse C. Cnossen, Center for Medical Decision Sciences, Department of Public Health, Erasmus Medical Center, NL-3015CN Rotterdam, The Netherlands. E-mail: m.c.cnossen@erasmusmc.nl
Moderate and severe traumatic brain injuries (TBI) are a growing public health problem and often lead to substantial physical and psychological burden for patients and relatives. Since TBI is not a single event, but a life-long disorder with differential needs over time, it is recognized as one of the most challenging areas in modern rehabilitation medicine (1).
Patients with moderate or severe TBI are usually referred to level I trauma centres where the process of rehabilitation starts with an emphasis on issues such as swallowing, contractures, pressure sores and neuro-behavioural disorders. From the acute care setting patients may be referred to specialized in- or outpatient rehabilitation settings, nursing facilities or, for example, neuropsychiatric wards in psychiatric hospitals. A patient out of post-traumatic amnesia with an attention span and physical condition that allows for 2 or 3 therapy sessions of approximately 10–15 min/day, is usually referred to an inpatient rehabilitation setting. Patients with disorders in consciousness, who recover slowly or who have severe neurobehavioural problems may be referred to nursing facilities or psychiatric hospitals. However, well-accepted algorithms to support the choice of follow-up treatment do not exist (2). Although there is growing evidence that both acute and post-acute rehabilitation interventions are beneficial for patients with acquired brain injury, including TBI (3–5), their specific ingredients, mechanism of action and efficacy is still referred to as a “black box” (6). As a consequence, large variations in structure and process characteristics of TBI rehabilitation may exist. Structures refer to conditions under which rehabilitation care is provided (e.g. availability of an in-hospital rehabilitation unit, personnel, facilities) (7), and processes refer to treatment and referral policies (7). As they may be related to differences in patient outcomes, exploring the variations in structure and process characteristics of TBI rehabilitation might provide directions for the identification of effective interventions.
The objective of this study is to provide a broad overview of structural and process characteristics of TBI rehabilitation among European neurotrauma centres, with a focus on acute in-hospital rehabilitation and referral to post-acute inpatient or outpatient care.
This study is part of the Collaborative European NeuroTrauma Effectiveness Research in TBI (CENTER-TBI) study, which is a prospective longitudinal observational study conducted in 72 centres from Austria, Belgium, Bosnia and Herzegovina, Denmark, Finland, France, Germany, Hungary, Israel, Italy, Lithuania, Latvia, the Netherlands, Norway, Romania, Serbia, Spain, Sweden, UK and Switzerland (8). The included centres were predominately academic hospitals (n = 65, 92%), situated in an urban location (n = 70, 99%), with a level I or II trauma centre designation (n = 52, 74%). Centres had a median of 1,000 (interquartile range 682–1395) hospital beds and treat approximately 91 (interquartile range 52–160) patients with moderate and severe TBI annually. For more information about the participating centres, see our previous publication (9).
Between 2014 and 2016, the local investigators, who are the senior persons supervising the CENTER-TBI study in each centre were approached to complete a set of 11 questionnaires, containing 321 questions: The Provider Profiling (PP) questionnaires. Questions concerned structures and processes of TBI care. For questions about process, we specifically asked for the “general policy” in a particular centre, which was defined as the way the large majority of patients (> 75%) with a certain indication would be treated, recognizing that there might be exceptions. We also explicitly mentioned that we were interested in the general policy at the department or hospital rather than individual treatment preferences.
The set of questionnaires was distributed among 71 out of 72 centres, since 2 CENTER-TBI centres represented different departments from the same hospital with similar structures and processes. The questionnaires were developed based on literature (e.g. the neurotrauma evidence map: http://neurotrauma.evidencemap.org) and expert opinion and were subsequently pilot-tested in 16 of the participating centres. All answers were checked for unexpected or missing values, and ambiguous questions were subsequently reformulated or deleted. Pilot-testers additionally completed a form in which they were asked to provide feedback, which was incorporated accordingly in the final questionnaires. Local investigators were informed about the PP questionnaires by presentations, workshops and emails. To be able to assess the reliability of the questionnaires, 17 (5%) questions were duplicated and asked twice in different parts of the questionnaires. We assessed the percentage of overlap between duplicate questions and calculated the median concordance rate over these 17 questions. The concordance rate was adequate, with a median of 0.85, meaning that 85% of the responses were similar. For more information about the development, administration and content of the total set of PP questionnaires, see our previous publication (9).
The questionnaire about rehabilitation addressed both in-hospital rehabilitation and referral to post-acute rehabilitation facilities (Appendix S1). This questionnaire included fourteen multiple-choice questions about structures (e.g. “what rehabilitation facilities are available at your institution”) and processes (e.g. “where are TBI patients with the following clinical characteristics generally referred to”) of rehabilitation care.
Frequencies and percentages of all categorical variables were reported. We subsequently calculated differences between relatively high- and middle-income countries vs relatively lower-income countries using χ2 test, and, if appropriate, Fisher’s exact test. The designation into relatively lower-income countries was based on a 2007 report by the European Commission (10) and the countries Bosnia and Herzegovina, Bulgaria, Hungary, Latvia, Lithuania, Romania and Serbia were subsequently classified as relatively lower-income countries. Analyses were performed using the Statistical Package for Social Sciences (SPSS) version 21.
The questionnaire about rehabilitation was completed by 99% (n = 70) of the participating centres. In the majority of centres, the questionnaire was completed by a rehabilitation physician (n = 28, 40%) or a neurosurgeon (n = 22, 31%). Other specialists that completed the questionnaire included neurologists, intensivists, heads of in-hospital rehabilitation units and study nurses.
The majority of participants indicated that rehabilitation physicians could be consulted for patients with TBI at the intensive care unit (ICU; n = 48, 70%) and the ward (n = 54, 78%; Table I). Of the centres that indicated that they could consult rehabilitation physicians at the ICU (n = 48) and ward (n = 54), approximately one-third reported that rehabilitation physicians were consulted in all patients with TBI. The remainder indicated that rehabilitation physicians were asked for a consultation on indication.
Table I. In-hospital rehabilitation in 70 European neurotrauma centres participating in the CENTER-TBI study
The large majority of centres could consult physical therapists, occupational therapists, speech therapists, dietician, social workers and/or rehabilitation nurses in both the ICU and ward. Neuropsychologists were available in half of the centres (ICU: n = 36, 52%; ward: n = 45, 65%).
In approximately half of the centres, a multidisciplinary rehabilitation team could be consulted for patients with TBI at the ICU (n = 29, 41%) and ward (n = 34, 49%). A multidisciplinary team was here defined as a full multidisciplinary rehabilitation service and not as isolated physiotherapy provision. There were no differences between high-/middle-income and relatively lower-income countries on any of the described characteristics (Table I).
In only 13 (19%) centres, rehabilitation guidelines or protocols were used when treating patients with TBI. Most of these guidelines were developed based on expert opinion within the centre and not based on evidence-based guidelines.
Half of the participants (n = 34) reported that they use coma stimulation in their centre. In these centres, mobility stimulation (n = 29, 85%) was used most often, followed by sensory stimulation (n = 25, 74%) and pharmacological stimulation (n = 19, 56%, Appendix S1).
Half of the participants (n = 37) reported to have an in-hospital rehabilitation unit, while one-third had an outpatient rehabilitation facility (n = 25). In addition, 57 (81%) participants indicated to have structural connections with rehabilitation facilities in the area. There were no differences between relatively high- and middle-income and lower-income countries on any of these characteristics (Table I).
To assess referral patterns to post-acute rehabilitation facilities, participants were presented 4 cases and they were requested to indicate which referral institutions they would consider. They were allowed to provide more than one answer, as long as it reflected their “general policy”. The cases included: (i) patients < 65 years and (ii) elderly patients > 65 years, both age groups with the following characteristics: (i) not obeying commands and (ii) obeying commands, but still in post-traumatic amnesia (PTA) and with severe behavioural problems.
The large majority indicated that the young patients would be referred to rehabilitation centres (Fig. 1).
Fig. 1. Referral to rehabilitation facilities in 70 neurotrauma centres participating in the CENTER-TBI study. Figure shows which rehabilitation facilities a centre would consider in patients with certain characteristics. Centres were allowed to select more than one facility as long as it reflected their general policy. Elderly patient: age ≥ 65 years.
Young patients not obeying commands could also be referred to nursing homes (n = 17), local hospitals (n = 19) or coma care facilities (n = 16). For young patients obeying commands but still in PTA and with severe behavioural problems, psychiatric hospitals (n = 17), local hospitals (n = 20) or outpatient facilities (n = 15) were also reported as referral possibilities.
For elderly patients, a more mixed image appeared. Elderly patients not obeying commands could be referred to either rehabilitation centres (n = 33), nursing homes (n = 32) or local hospitals (n = 29). For elderly patients obeying commands, but still in PTA, and with severe behavioural problems, rehabilitation centres (n = 46) were most often considered, followed by nursing homes (n = 26) and local hospitals (n = 27).
Participants were asked explicitly whether patient’s age has a major influence on referral decisions. Forty-six percent (n = 32) indicated that this was the case. Participants declared that rehabilitation programmes have age limits or selection favouring younger patients. Also, the rehabilitation potential of older patients is regarded as lower, and as a consequence, older patients are more often referred to non-specialized rehabilitation programmes or nursing homes (Appendix S1).
We elaborated on whether the influence of age on referral decisions was dependent on income, geographical location (North and West Europe vs South and East Europe and Israel), the completer of the questionnaire (rehabilitation physician vs other completer), personnel characteristics (availability of a rehabilitation physician and neuropsychologist) and the availability of an in-hospital multidisciplinary team and an in-hospital rehabilitation unit (Appendix S2). We found that high- and middle-income countries more often indicated that age has a major influence on referral in comparison with relatively lower-income countries (p < 0.01). There were, however, no differences between high- and middle- and relatively lower-income countries in whether they would generally refer elderly patients to nursing homes. In addition, we found a trend toward higher referral to nursing homes in elderly patients with PTA and behavioural problems in North and West Europe in comparison in South and East Europe and Israel (p = 0.09). In addition, we found that centres in which a rehabilitation physician was available more often indicated that age has a major influence on referral decisions in comparison with centres in which a rehabilitation physician was not available (p = 0.05).
We asked for the average waiting time for rehabilitation facilities, which was defined as the time between the moment that the patient is ready to be discharged from the centre and the time of admission or first visit at the referral institute. The mean waiting time was usually no longer than 1 month (Table II). For specialized rehabilitation centres, patients could be admitted within a few days in 7 (10%) centres, within 1 week in 26 (38%) centres and within 1 month in 27 (40%) centres. The waiting time for nursing homes and coma care facilities was slightly longer.
Table II. Waiting time for rehabilitation facilities among 70 European neurotrauma centres participating in the CENTER-TBI study
Participants had to indicate how important certain factors were in their referral decision to rehabilitation facilities. They were asked to give a score of 1 (most important) to 5 (least important) to the following aspects: quality of care, distance to a patient’s home, availability at short notice, specialized neuro-rehabilitation, and funding (Fig. 2). Distance to a patient’s home was rated as the most important factor for rehabilitation referral and funding/financial reason was rated as the least important factor.
Fig. 2. Factors considered important in the referral decision of 70 neurotrauma centres participating in the CENTER-TBI study. Figure shows the number of centres that responded with a 1 (most important) or 2 (second most important) to the 5 factors that could be considered relevant in decisions about referral to rehabilitation facilities.
We subsequently asked participants how satisfied they were with rehabilitation possibilities in their area, using the same criteria (except for funding/financial reason). Regarding quality of care and specialized neuro-rehabilitation possibilities, the majority of centres were satisfied (score 4 or 5 out of 5). However, for distance to a patient’s home and availability at short notice, less than half of the centres gave a score of 4 or 5 (Fig. 3). Three centres, from 3 different countries indicated that they were dissatisfied with all 4 items (score 1 or 2 on all items).
Fig. 3. Satisfaction with rehabilitation facilities in 70 neurotrauma centres participating in the CENTER-TBI study. Centres were asked whether they were satisfied with the rehabilitation facilities in their region: 1 = not satisfied; 5 = completely satisfied.
We found marked variation in structure and process characteristics of early in-hospital TBI rehabilitation and referral to post-acute rehabilitation care among 70 centres participating in a European TBI research project.
The following limitations should be taken into account when interpreting the data. First and foremost, the included centres comprise a selected group of neurotrauma centres participating in a European multicentre study. The centres are all active in the field of neurotrauma care and research, and therefore, it may be that the picture obtained is better than the real overall situation in Europe. The differences in structures and processes may be even larger when considering non-specialized centres. Our findings therefore cannot be generalized and should be interpreted with caution. Secondly, our study provides information on what centres reported rather than characteristics that were directly observed. Lack of concordance between reported and observed characteristics is common in survey studies. For example, a 2007 survey study about intracranial pressure (ICP) monitoring reported that 77% of the patients were treated according to the guidelines (11), while a recent systematic review found that the mean percentage adherence to ICP monitoring guidelines was only 31% (12). We cannot exclude that the centres in our study also provided a more favourable image of their structural and process characteristics. This would again result in a more favourable picture. Related questionnaires were completed by only a few physicians in every centre rather than by all physicians that treat patients with TBI in a particular centre. Although we asked for their general policy, we cannot exclude that some of the answers display personal opinions rather than the department or hospital policy. Results from the ongoing CENTER-TBI study will provide insight into possible discrepancies between these policy opinion statements and actual practice. Another limitation is that the question on referral preferences did not take into account patients’ and proxies’ preferences and needs. It should be acknowledged that referral decisions in clinical practice often incorporate patients’ and proxies’ preferences and might be based on shared decision-making. Therefore, the results on referral preferences should be interpreted as the participant’s rating of relative importance of 5 factors rather than displaying actual referral patterns. The PP questionnaires themselves also have some limitations. For example, the length (321 questions) may have resulted in lower data quality (9).
The observed variation in structure and process is consistent with other surveys about rehabilitation after TBI (13–16). Large variation in rehabilitation practices might be partly explained by the limited use of guidelines. Only one-fifth of the centres in our survey indicated that they use TBI-specific rehabilitation guidelines during the acute treatment phase. These guidelines were based on expert opinion and developed within the centre, rather than based on national/international evidence-based guidelines. This reflects an absence of evidence-based guidelines on this topic. For instance, the Brain Trauma Foundation guidelines, which are probably the most often used guidelines for the treatment of patients with severe TBI, have not included recommendations regarding in-hospital rehabilitation (17). We would therefore recommend guideline developers to include recommendations about early rehabilitation in their guidelines.
Another interesting finding is the influence of age on referral decisions. In our survey, patients above age 65 years are less often referred to specialized rehabilitation centres than younger patients and approximately half of the centres indicated that age has a major influence on referral decisions. This shows a clear disparity in access to care, and is against the Article 21 of the Fundamental Rights of EU. Inequality in access to rehabilitation care after brain injury has been widely shown for racial and ethnic minorities (18–21) and uninsured patients (19, 21) and our study implies that patients with an older age are also at risk. Notwithstanding, it has been shown that elderly patients can make substantial improvements during inpatient rehabilitation and could often be discharged home (22, 23). Since the prevalence of elderly TBI patients is increasing (24), physicians and policymakers should be aware of the age disparity, and the influence of age on rehabilitation potential should be studied further in future studies. The concept of inferior rehabilitation potential in the elderly may be a consequence of a self-fulfilling prophecy in earlier practices and studies. In addition, further qualitative research might unravel as to why age is an important factor in referral to rehabilitation facilities for some doctors and centres and not for others.
Another implication of our work is that the effectiveness of rehabilitation interventions could be studied with comparative effectiveness research (CER). Knowledge about effectiveness and best practices of TBI rehabilitation is critically important, since recent research has suggested that differences in outcome between developed and developing countries are mainly due to differences in rehabilitation care, rather than differences in acute care (25). CER refers to the use of existing differences in policy between centres to analyse treatment effectiveness. A prerequisite for CER is that there is considerable variation in policy among centres, which is shown in our study. We therefore think that CER is an adequate framework to enhance knowledge about effectiveness of rehabilitation interventions in TBI and inform patients, clinicians and guideline developers directly about this information. CER within the CENTER-TBI project can be studied by comparing patients in centres that perform a certain intervention as the general policy to patients in centres that do not generally use this intervention. For example, we can compare the outcome of comatose patients from the 34 centres that use in-hospital coma stimulation with comatose patients from the 36 centres that do not use in-hospital coma stimulation, after correcting for case mix and other differences among centres. Other potential interesting topics for CER based on the current results include the availability of an in-hospital multidisciplinary team, the treatment of elderly patients in specialized rehabilitation centres vs in nursing homes and the impact of waiting time on outcome.
In conclusion, marked variation in structure and process of in-hospital rehabilitation and referral to rehabilitation facilities exists between European neurotrauma centres. This variation provides the possibility to study effectiveness of specific rehabilitation interventions in comparative effectiveness research, but also indicates that there is probably room for improvement in quality of care, long-term outcome and cost-effectiveness of TBI rehabilitation. In addition, this study found a disparity in access to specialized rehabilitation care for elderly patients. Future research is warranted to study referral decision-making processes and further investigate the rehabilitation potential of elderly patients.
Data used in preparation of this manuscript were obtained in the context of CENTER-TBI, a large collaborative project with the support of the European Commission 7th Framework program (602150).
The authors would like to thank all CENTER-TBI investigators and their staff, who are listed at the end of the manuscript, for completing the provider profiling questionnaires.


 Click to show fullsize
Click to show fullsize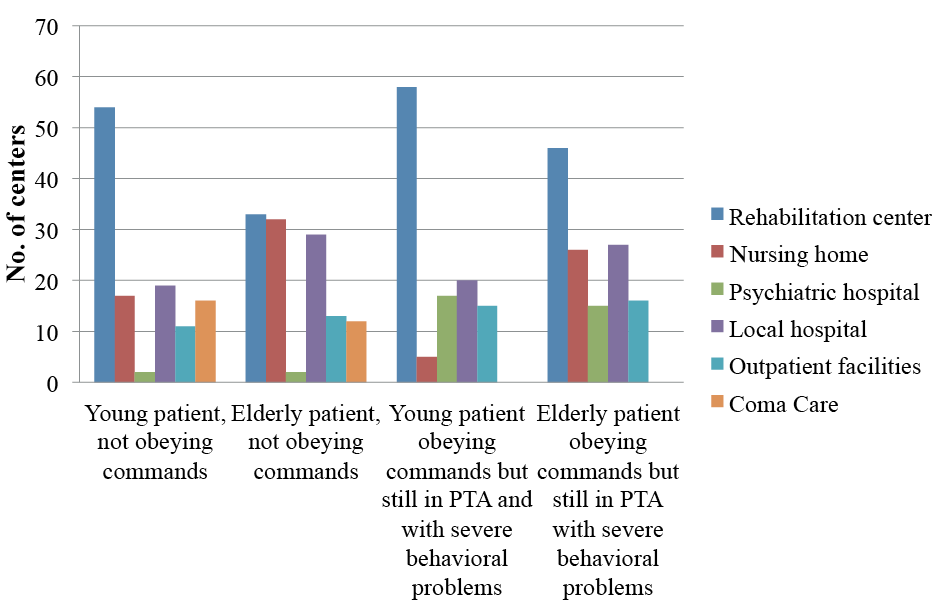 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize