
1From the Parker Institute, Copenhagen University Hospital, Bispebjerg-Frederiksberg Hospital, 2The Research Initiative for Activity Studies and Occupational Therapy, General Practice, Department of Public Health, University of Southern Denmark, Odense and 3Metropolitan University College, Copenhagen, Denmark
Objective: To explore and compare the outcomes of adaptation and physical activity programmes regarding activities of daily living (ADL) ability following interdisciplinary rehabilitation in women with fibromyalgia.
Methods: Participants (n = 85) were quasi-randomized to 16-week adaptation (ADAPT) or physical activity (ACTIVE) programmes following 2-week interdisciplinary rehabilitation. Primary outcomes were ADL motor and ADL process ability, measured with the Assessment of Motor and Process Skills (AMPS) at 4-week follow-up. Data were analysed per protocol.
Results: Participants (ADAPT, n = 21; ACTIVE, n = 27) did not differ from withdrawers (n = 37). Improvements in ADL ability in the ADAPT (ADL motor mean change = 0.43 logits (95% confidence interval (95% CI) = 0.31–0.56); ADL process mean change = 0.34 logits (95% CI = 0.17–0.52)) and ACTIVE (ADL motor mean change = 0.33 logits (95% CI = 0.22–0.43); ADL process mean change = 0.25 logits (95% CI = 0.12–0.38)) groups were statistically significant, with no differences between groups. Responder analyses revealed that 63% of all participants obtained clinically relevant improvements in ADL motor ability and 48% in ADL process ability.
Conclusion: Although limited by a large drop-out, this exploratory study showed that both adaptation and physical activity programmes following interdisciplinary rehabilitation improved ADL ability in the majority of participants. ADL ability outcomes were independent of group allocation (ADAPT vs ACTIVE), suggesting efficacy of both programmes.
Key words: occupational therapy; physiotherapy; Assessment of Motor and Process Skills; ADL; intervention; rehabilitation.
Accepted Dec 6, 2016; Epub ahead of print Feb 27, 2017
J Rehabil Med 2017; 49: 241–250
Correspondence address: Cecilie von Bülow, The Parker Institute, Bispebjerg-Frederiksberg Hospital, Nordre Fasanvej 57, DK-2000 Frederiksberg, Denmark. E-mail: Cecilie.von.Bulow@regionh.dk
Improved functioning is a main goal of rehabilitation (1, 2). Essential to functioning is the ability to perform activities of daily living (ADL), such as self-care and household tasks (1, 2). ADL ability in women with fibromyalgia encountered in tertiary care has been shown to be significantly reduced, and the extent of ADL task performance problems often cause these individuals to need assistance for safe community living (3). Multidisciplinary and interdisciplinary rehabilitation is recommended (4, 5), but despite clinically relevant improvements in ADL ability after rehabilitation, women with fibromyalgia still show considerable ADL disability and large inter-individual patient variability in functional gains (6). It has therefore been suggested that clinical effectiveness may be promoted if intervention programmes are more individually tailored and specifically designed to improve ADL ability (6).
Exercise (e.g. aerobic, strength and flexibility training) and physical activity (e.g. recreational physical activity, sports and brisk walking) are recommended in the management of fibromyalgia to improve functioning, including ADL ability (7, 8). Studies, however, report problems related to adherence, adverse events and high drop-out rates (7, 8) and severely impacted persons seem to gain less effect (9). Thus, while some benefit from exercise/physical activity, others may need other types of intervention to improve ADL ability.
Interventions focusing on adaptation emphasize helping persons to adapt to situations and change the environment, rather than focusing on restoration of body functions and structures (10, 11). Adaptation includes the use of strategies to compensate for performance problems, such as changing routines, using assistive devices, and modifying tasks and physical/social environments (12). Adaptation is not associated with adverse events (5) and has been shown to improve ADL ability in populations with various chronic health conditions (13, 14). Adaptation is also recommended as part of rehabilitation for people with fibromyalgia (5, 15), although evidence supporting its efficacy is lacking.
Thus, the aim of this exploratory study was to investigate changes in ADL ability and to compare ADL ability outcomes of adaptation and physical activity programmes following a 2-week interdisciplinary rehabilitation programme in women with fibromyalgia. As exercise/physical activity seems to be effective in some individuals with fibromyalgia (7–9), others might benefit from adaptation. It was therefore assumed that both programmes would enhance ADL ability outcomes and that no programme would be superior to the other.
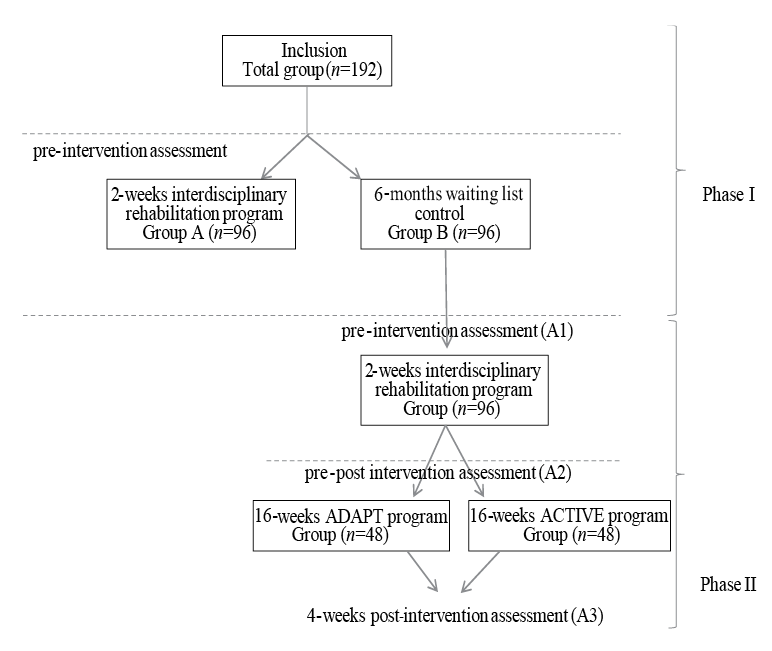
This exploratory, quasi-randomized study was conducted from January 2012 to February 2013. The study constituted the second phase of the IMPROvE study (Interdisciplinary Rehabilitation of Patients with Chronic Widespread Pain: Primary Endpoint of the Randomised, Non-Blinded, Parallel-Group IMPROvE Trial) (6), approved by the local ethics committee of the Capital Region of Denmark (H-2-2010-139), carried out in accordance with principles of the Declaration of Helsinki and registered with www.clinicaltrials.gov, number NCT01352052. While phase I/IMPROvE (6) investiged outcomes of a 2-week interdisciplinary rehabilitation programme, this phase II/IMPROvE explored outcomes of the same 2-week interdisciplinary rehabilitation programme followed by additional 16-week adaptation or physical activity programmes (Fig. 1). Participants in the IMPROvE study were recruited from the outpatient clinic at the Department of Rheumatology, Bispebjerg-Frederiksberg Hospital, Denmark; all women, > 18 years of age and fulfilled the 1990 American College of Rheumatology (ACR) classification criteria for fibromyalgia (16).
Fig. 1. IMPROvE study design for phase I and phase II.
Participants acting as waiting list control group in phase I/IMPROvE were consecutively enrolled in the interdisciplinary rehabilitation programme in groups of 8. Groups (n = 12) were then quasi-randomized by coin-flip by a biostatistician who was not involved in the study. Odd-numbered groups (i.e. 1, 3, 5, 7, 9, 11) were allocated to the adaptation programme (ADAPT) and even-numbered groups (i.e. 2, 4, 6, 8, 10, 12) to the physical activity programme (ACTIVE). Neither staff involved in the interdisciplinary rehabilitation programme nor participants were informed about group allocation until the last day of the interdisciplinary rehabilitation programme, where the therapists conducting the ADAPT and ACTIVE programmes revealed the allocation. Assessments were performed by blinded assessors not informed about the participants’ allocation and not involved in the ADAPT and ACTIVE programmes. Questionnaires were completed using touch screens, which have been shown to give comparable results to answers given on paper (17).
The interdisciplinary rehabilitation was a 2-week outpatient, group-based programme conducted by a rheumatologist, psychologist, nurse, and occupational and physical therapists. The programme had a daily time schedule between 3 and 5 h and included a team conference aiming at monitoring individuals’ progression towards overall rehabilitation goals, i.e. increasing functional ability and coping with pain (6).
The ADAPT and ACTIVE programmes were developed to investigate whether adaptation and physical activity programmes provided as an add-on would enhance ADL ability outcomes in women with fibromyalgia. Both programmes lasted 16 weeks, were group-based and inspired by an existing programme (18) supporting education, reflection, brainstorms, group discussions and peer exchange, as a means to promote changes in everyday life. Sessions typically began with a short lecture or a discussion initiated by the therapist posing a question. Over time the participants were to assume the role of experts and share knowledge from their own experiences. The programmes were primarily education-based and, to a lesser extent, encompassed practical exercises. Participants were encouraged to implement adaptation strategies or increase the level of physical activity at home in-between sessions.
ADAPT programme. The ADAPT programme (Appendix I) was developed and led by an occupational therapist, included 16 2-h sessions and aimed at improving ADL ability by means of adaptation (10–12). This approach was based on the assumption that adaptation strategies could be used to compensate for task performance problems and thus improve ADL ability. The compensatory and educational models (12) were used as primary means to teach the participants how to adapt more successfully, i.e. how to solve ADL task performance problems by implementing adaptation strategies, such as assistive devices, modifications of ADL tasks, and physical and/or social environments. The sessions took place in a clinical ADL unit, i.e. a 2-room flat used to observe and practice ADL task performance in a simulated, but naturalistic, home environment.
Appendix I. Summary of the ADAPT programme
ACTIVE programme. The ACTIVE programme (Appendix II) was developed and led by a physiotherapist, included 10 2-h sessions and aimed at improving ADL ability by means of graded physical activity (19, 20). This approach was based on the assumption that increased physical activity improves body functions and structures and allows ADL tasks to be performed at a lower percentage of maximum capacity (7). Education was the primary means to implement strategies to increase physical activity in everyday life. The programme was conducted in a clinical unit fitted for group discussions and performance of light exercises (e.g. resistance-band exercises).
Appendix II. ACTIVE programme
The study included 3 assessments points. Baseline assessment 1 (A1) was performed 3 weeks prior to the interdisciplinary rehabilitation programme. There was approximately 1 month between the end of the interdisciplinary rehabilitation programme and the beginning of the additional programmes. Assessment 2 (A2) was performed 3 weeks after the rehabilitation programme, and served as a baseline prior to entry to the additional programmes. For logistical reasons, assessment 3 (A3) was performed 4 weeks after the additional ADAPT/ACTIVE programmes (Fig. 1). While the primary endpoint was change during the interdisciplinary rehabilitation programme and additional ADAPT or ACTIVE programmes (A1–A3), the secondary endpoint was change during the additional programmes (A2–A3).
Change in observed ADL ability was the primary outcome measured with the Assessment of Motor and Process Skills (AMPS) (21).
Assessment of Motor and Process Skills (AMPS). The AMPS evaluates 2 aspects of ADL ability; ADL motor ability (amount of effort, fatigue and/or clumsiness) and ADL process ability (degree of disorganization, inappropriate use of time, space or objects and adapting actions) (21). The quality of 16 ADL motor skills (move self and objects) and 20 ADL process skills (organize and adapt actions) is scored on a 4-point ordinal scale in terms of ease, efficiency, safety, and independence. Raw scores are analysed using a many-faceted Rasch-based computer-scoring software program, which converts the raw ordinal scores into 2 overall linear measures of ADL motor and ADL process ability, expressed in logits (i.e. logistically transformed probability units) adjusted for rater severity as well as ADL task and skill item difficulty (21). Both the AMPS ADL motor ability measure and the AMPS ADL process ability measure served as primary outcomes in this study. ADL ability measures below the 1.50 logit independence cut-off on the ADL motor scale and below the 1.00 logit independence cut-off on the ADL process scale indicate a likely need for assistance (21). Measures below the lower independence cut-offs of 1.00 and 0.70 logits for ADL motor and ADL process ability, respectively, mark a need for moderate/maximal assistance (22). The AMPS has demonstrated sound psychometric properties when applied to women with fibromyalgia, including sensitivity to change post-intervention (23). According to the AMPS manual (21) a difference of ≥ 0.30 logits on the ADL motor and/or ADL process scales defines a clinically relevant difference in ADL ability.
Secondary outcomes included self-reported ADL ability evaluated with the ADL-Questionnaire (ADL-Q) (24) and the physical functioning subscale of the MOS 36-item Short Form (25) (SF-36 PF). Disease severity was evaluated with the total score of the Fibromyalgia Impact Questionnaire (FIQ) (26) and pain with the FIQ pain subscale. Health-related quality of life was evaluated with the SF-36 Physical Composite Score (PCS) and Mental Composite Score (MCS) (25).
ADL-Questionnaire (ADL-Q). ADL-Q is a standardized instrument developed to measure a person’s perceived quality of ADL task performance in 12 domains related to 47 ADL tasks. The person marks the quality of the ADL task performance using 7 response categories reflecting efficiency, effort/fatigue, safety, and independence. ADL-Q requires Rasch-measurement methods in order to convert the raw ordinal data into linear measures of ADL ability (24, 27). The ADL-Q has demonstrated sensitivity to change when applied in women with fibromyalgia (24). Clinically relevant differences were determined based on the criterion of 0.5 standard deviation (SD) (28) for a comparable study sample (29), i.e. ≥ 1.00 logits.
MOS 36-Item Short Form (SF-36). The SF-36 is a generic instrument constructed to evaluate physical and mental health-related quality of life expressed in 2 composite scores, i.e. SF-36 PCS and SF-36 MCS. The ordinal scale scores are transformed into linear scales, ranging from 0 to 100, and standardized to reflect a general population (US) mean of 50 (SD 10). Measures of 0 = worst possible health status, and 100 = best health status. The SF-36 PF subscale evaluates the extent of perceived limitations of task performance due to health-related problems (i.e. perform vigorous and moderate activities, lift or carry groceries, climb 1 or several flights of stairs, make beds, walk 1 block or more than 1 mile, and bathe or dress). Response categories are scored on a 3-point Likert scale (i.e. 1 = limited to 3 = not limited at all). Raw scores are summed into 1 overall score for functioning, ranging from 0 to 100 points, in which 0 = severely limited and 100 = the person performs all types of tasks (25). Based on the criterion of 0.5 SD (28) in a comparable study sample (30), clinically relevant differences were determined as: SF-PF ≥ 10.00 points, SF-36 PCS ≥ 3.34 points and SF-36 MCS > 5.98 points.
Fibromyalgia Impact Questionnaire (FIQ). FIQ is a disease-specific questionnaire, composed of 10 subscales, designed to evaluate disease severity (FIQ total). The average person with fibromyalgia is expected to obtain a FIQ total score of approximately 50 points, whereas more severely impacted persons score > 70 out of 100 (31). The fifth item in the FIQ is a 100-mm visual analogue scale (VAS) used to evaluate pain intensity; 0 = no pain to 10 = very severe pain (26). Based on the criterion of 0.5 SD (28) in a comparable study sample (30), clinically relevant differences were determined as: FIQ total ≥ 9.27 points and FIQ pain > 0.98 mm.
Sample size was based on the sample size calculation from phase I/IMPROvE (6). With AMPS as primary outcome, a 2-sample pooled t-test of a normal mean difference with a 2-sided significance level of 0.05, assuming a common SD of 0.4, a sample size of 86 per group was required to obtain a power of at least 0.9 to detect a group mean difference of 0.2 (6). Because participants would be enrolled in groups of 8 it was decided to include 96 participants in each arm, thus including a total of 192 participants in phase I/IMPROvE (Fig. 1). This sample size calculation allowed for an expected drop-out rate of 20% in phase II/IMPROvE. Efficacy was analysed on a per protocol basis, only including participants with an attendance of at least 25% in the additional programmes. Participants who withdrew or attended less than 25% were not reassessed 4-weeks post-intervention. Consequently, no intention-to-treat analyses were performed. Distribution of data was tested for normality. Primary outcomes, i.e. AMPS ADL ability measures, were investigated using analyses of variance (ANOVA) with time (A1, A2, A3) by programme (ADAPT/ACTIVE) as repeated measure, followed by post hoc paired-samples and independent-samples t-tests, and reported as means and 95% confidence intervals (95% CI) at the primary (A1–A3) and secondary endpoints (A2–A3). Secondary outcomes were analysed at the primary endpoint. Changes in the linear ADL-Q measures were analysed and compared using paired-samples and independent-samples t-tests, while changes in the ordinal SF-36 and FIQ scores were analysed and compared using Wilcoxon signed-rank test and Mann–Whitney U test and reported in medians and quartiles (Q).
Responders were defined as participants achieving a clinically relevant improvement in ADL ability measures on instruments specifically designed to measure ADL ability, i.e. the AMPS (≥ 0.30 logits) and ADL-Q (≥ 1.00 logits). The proportions (number and percentages) of responders were calculated and compared by Pearson’s χ2 tests and mean changes in observed and self-reported ADL ability for responders were analysed and compared using paired-samples and independent-samples t-tests and reported in means and 95% CI. SPSS software was used in all analyses (32).
Overall, 85 participants were enrolled in the interdisciplinary rehabilitation programme and were quasi-randomized to the ADAPT (n = 43) or ACTIVE (n = 42) programmes. Fig. 2 illustrates the flow of participants through the study, including time points and reasons for the large dropout (n = 37). Baseline characteristics for participants completing the ADAPT or ACTIVE programmes and participants who withdrew are presented in Table I.
Fig. 2. CONSORT flow diagram showing participants’ flow through the study. A1, A2, A3; assessments 1, 2, 3.
Table I. Baseline characteristics for the total sample and when grouped into ADAPT participants, ACTIVE participants and withdrawers
In all 3 groups, the pain duration averaged 10 years and participants reported high levels of pain and fatigue. ADL ability measures indicated considerable disability, 72% were unemployed, and 44% had a pending social welfare application. No significant differences in baseline characteristics between the 3 groups were identified.
Changes over the 3 assessment points (A1–A3) in primary outcomes, i.e. AMPS ADL motor and process ability measures are illustrated in Fig. 3a–b. Improvements in ADL motor ability in the ADAPT (mean change = 0.43; 95% CI = 0.31 to 0.56) and ACTIVE (mean change = 0.34; 95% CI = 0.17 to 0.52) groups from baseline (A1) to 4-week follow-up (A3) were statistically significant and clinically relevant, but without significant differences across groups (95% CI = –0.13 to 0.32) (Table II). In addition, the ADL process ability improved statistically significant in the ADAPT (mean change = 0.33; 95% CI = 0.22 to 0.43) and ACTIVE (mean change = 0.25; 95% CI = 0.12 to 0.38) groups at the primary endpoint, but only the improvement in the ADAPT group was clinically relevant and there were no significant group differences (95% CI = –0.11 to 0.25) (Table II).
Fig. 3. (a) Mean changes in AMPS ADL motor ability over time. (b) Mean changes in AMPS ADL process ability over time. (A1, A2, A3) by programme (ADAPT/ACTIVE). ADAPT: adaptation programme; ACTIVE: physical activity programme; AMPS: Assessment of Motor and Process Skills; ADL: activities of daily living; A1, A2, A3: Assessment 1, 2, 3.
Table II. Changes in primary outcomes at primary and secondary endpoints and secondary outcomes at primary endpoint
At the secondary endpoint (A2–A3), i.e. prior to the additional programmes (A2) to 4-week follow-up (A3), the ADL motor ability improved statistically significant in the ADAPT group (mean change = 0.25: 95% CI = 0.13 to 0.37), but not in the ACTIVE group (mean change = 0.04; 95% CI = –0.07 to 0.15). The difference between groups was statistically significant (95% CI = 0.03 to 0.39) (Table II). No significant changes in ADL process ability in either of the groups (ADAPT: mean change = 0.07; 95% CI = 0.00 to 0.15; ACTIVE: mean change = 0.07; 95% CI = –0.01 to 0.15) were observed at this assessment point (Table II).
While the ADAPT group reported no significant change in ADL ability evaluated with ADL-Q (mean change = –0.21; 95% CI = –1.40 to 0.80), the ACTIVE group reported statistically significant lower levels of ADL ability (mean change = –0.63; 95% CI = –1.13 to –0.16). This observed decline, however, was not clinically relevant and differences between groups in ADL-Q ADL ability was not statistically significant (p = 0.47) (Table II). None of the other self-reported secondary outcomes showed any significant change over time or differences at group level (Table II).
Responder analyses revealed that 63% (30/48) of the total sample obtained clinically relevant improvements in ADL motor ability (mean change = 0.60; 95% CI = 0.51 to 0.70) and 48% (23/48) in ADL process ability (mean change = 0.53; 95% CI = 0.47 to 0.61) at the primary endpoint. Sixty-seven percent (14/21) in the ADAPT group showed clinically relevant improvements in ADL motor ability (mean change = 0.58; 95% CI = 0.48 to 0.71) and 52% (11/21) in ADL process ability (mean change = 0.52; 95% CI = 0.43 to 0.59). In comparison, 59% (16/27) in the ACTIVE group showed clinically relevant improvements in ADL motor ability (mean change = 0.62; 95% CI = 0.47 to 0.77) and 44% (12/27) in ADL process ability (mean change = 0.55; 95% CI = 0.45 to 0.67) at the primary endpoint. Measures at the secondary endpoint showed that 71% (10/14) of the ADAPT responders and 50% (8/16) of the ACTIVE responders gained their ADL motor ability improvements during the additional programmes. Correspondingly, 18% (2/11) and 25% (3/12) of the responders gained their ADL process ability improvements during the ADAPT and ACTIVE programmes, respectively. Neither the proportion of responders nor the mean improvements in ADL ability differed statistically significant between groups at primary or secondary endpoints (Table III).
Table III. Proportion of responder and mean changes in activities of daily living (ADL) ability at primary and secondary endpoints
Subgroup analysis showed that in ADAPT/ACTIVE responders the mean ADL motor ability measure was 0.91 (95% CI =0.78 to 1.04) logits and the mean ADL process ability measure 0.68 (95% CI = 0.61 to 0.75) logits at baseline (A1). These ability measures were clinically and statistically significantly lower (ADL motor mean difference = 0.58; 95% CI = 0.43 to 0.74: ADL process mean difference = 0.47; 95% CI = 0.36 to 0.59) than baseline measures for the non-responders (ADL motor ability = 1.45; 95% CI = 1.28 to 1.61: ADL process ability = 1.05; 95% CI = 0.96 to 1.13).
A total of 10% (5/48) reported clinically relevant improvements (mean change = 2.50; 95% CI = 1.45 to 4.33) in ADL ability at the primary endpoint on the ADL-Q, while 90% (43/48) reported no clinically relevant change (mean change = –0.80; 95% CI = –1.34 to –0.38).
To our knowledge, this is the first study to explore changes in ADL ability and compare the ADL ability outcomes of individually tailored add-on adaptation or graded physical activity programmes following an interdisciplinary rehabilitation programme in women with fibromyalgia. The results of this exploratory study indicated that participants achieved statistically significant improvements in ADL motor and ADL process ability at 4-week post-intervention independent of group allocation to the ADAPT vs the ACTIVE programme. Although responder analyses demonstrated inter-individual patient variability, clinically relevant improvements in ADL motor and ADL process ability were observed in 63% and 48% of the overall study sample, respectively. No previous studies have shown similar functional responder rates among women with fibromyalgia.
In phase I/IMPROvE (6), evaluating the outcomes of the interdisciplinary rehabilitation programme, 36% of the participants obtained clinically relevant improvements in ADL motor ability and 18% in ADL process ability, respectively. Thus, adding additional programme components to the rehabilitation programme, which were specifically developed to improve ADL ability, seems to have improved functional gains considerably, even in this sample of women with fibromyalgia presenting with substantial disability established over many years.
Assessed with the AMPS, the observed performance difficulties in our study sample were dominated by decreased ADL motor ability and it was within this domain that most participants achieved a clinically meaningful improvement. The study revealed no significant differences between the ADAPT and ACTIVE groups in ADL motor ability outcome at the primary endpoint, suggesting efficiency of both programmes. However, the observed larger mean change in ADL motor ability and a 95% CI indicating a clinically relevant improvement in the majority of participants in the ADAPT group, could indicate that this programme was superior to the ACTIVE programme. Overall, the participants attending the ADAPT programme obtained a mean change of 0.43 (95% CI = 0.31 to 0.56) logits in ADL motor ability vs 0.34 (95% CI = 0.17 to 0.52) logits in the ACTIVE programme. Although not significant, the notion of a better ADL motor ability outcome in the ADAPT programme was further supported by a higher proportion of ADL motor responders in this group, 48% vs 30% in the ACTIVE group. This could indicate that participants in the ACTIVE group had more differential treatment effects compared with participants in the ADAPT group, possibly reflecting problems with adherence. Adherence constitutes a known problem in fibromyalgia, as physical activity may be experienced to increase symptoms (8). The seemingly less differential treatment response and higher responder rate in the ADAPT group may support a broader relevance of applying adaptation strategies to improve ADL ability in women with moderate to severe fibromyalgia. Adaptation may be an easier and better tolerated approach and may therefore promote adherence. This hypothesis, however, needs testing in future larger studies.
Post hoc subgroup analysis revealed significant baseline (A1) differences in the AMPS ADL profiles of responders and non-responders. At baseline, the non-responders presented with overall higher levels of ADL ability, i.e. they used less effort, were more efficient, safe and independent during ADL task performance compared with responders. Responders presented with ADL ability measures below the lower independence cut-offs at baseline, indicating increased effort, fatigue, inappropriate use of time, space or objects and decreased ability to adapt actions efficiently during ADL task performance. The observed extent of performance problems probably caused these participants to have a need for moderate/maximal assistance in everyday life prior to entering the intervention (21). At 4-week post-intervention the obtained AMPS ADL ability measures in the responders indicated that ADL tasks were performed with significantly less effort, increased efficiency, less safety risk and less need of assistance. These findings are in accordance with existing guidelines, recommending interdisciplinary rehabilitation for more severely impacted persons (4, 5). The results of this study, however, seem to support the relevance of offering additional targeted interventions, as the majority of the participants gained their improvements in ADL motor ability during the additional programmes (A2–A3).
Despite the observed clinically relevant improvements in AMPS ADL ability measures among a rather large proportion of the participants, only 10% reported clinically relevant improvements in ADL ability using the ADL-Q. Several studies (24, 33, 34) support that self-report and observation provides distinct information about ADL ability and cannot substitute for each other. Individuals’ perception of functioning seems to be influenced by factors such as disease severity, pain and health-related quality of life, and may therefore not reflect actual performance (34). As none of these factors changed during the intervention the participants’ reporting may still be influenced. The lack of changes in disease severity, pain and health-related quality of life suggests that assessments at the body level and global assessments, cannot substitute for observation-based evaluation of ADL ability (34).
The study had several limitations. Due to the study design, with no control group, it was only possible to evaluate the ADL ability outcome of the combined intervention and not of the individual ADAPT and ACTIVE programmes. Still, it seems that the additional programmes significantly enhanced the proportion of responders. The study included only moderately/severely impacted women with fibromyalgia and findings may therefore not be generalized to the overall referral population. A large proportion of the sample withdrew prior to the ADAPT/ACTIVE programmes; however, the reasons for dropping out were not adverse events, as reported previously (7, 8). The resulting smaller sample size, the lack of intention-to-treat analysis and per protocol analysis may have increased the risk of overestimating outcomes, whereas the use of blinded assessors is considered to reduce reporting bias (35). The small sample size may also have underpowered the study to identify changes in secondary outcomes and differences between groups, and future larger studies are therefore warranted.
In conclusion, although limited by a large dropout rate, the study showed that both adaptation and physical activity programmes following interdisciplinary rehabilitation improved observed ADL ability, as indicated by decreased effort, increased efficiency, safety and independence. These improvements were identified in more than two-thirds of a sample of women with fibromyalgia presenting with longstanding pain and substantial ADL disability at baseline. No significant group differences were observed in this smaller study sample, indicating efficiency of both programmes. Still, the study pointed towards less differential treatment response and higher responder rate in participants allocated to adaptation. Thus, the results of this exploratory study provide initial evidence for using adaptation to improve ADL ability in women with fibromyalgia, and support existing recommendations (7, 8) of integrating physical activity programmes in the management of fibromyalgia populations.
This study was supported by The Oak Foundation, Schioldanns Foundation, The Danish Rheumatism Association and The Danish Association of Occupational Therapy. The authors would like to thank OT, PhD. Karen la Cour for reviewing the manuscript and database consultant Christian Cato for support with data entry. The authors would also like to thank OT, MSc, Mette Gramstrup Søndergaard for collecting data, and Marianne Uggen Rasmussen, RN, MPH, PhD, together with all other colleagues at the Parker Institute for good scientific discussions as well as the staff at the Department of Rheumatology, Bispebjerg-Frederiksberg Hospital for contributing to data collection. Finally, the authors gratefully acknowledge the participants in this study.
Conflicts of interest: The ADAPT and ACTIVE programmes were developed and conducted by 2 of the authors, but none of the named authors have a conflict of interest related to the study content


 Click to show fullsize
Click to show fullsize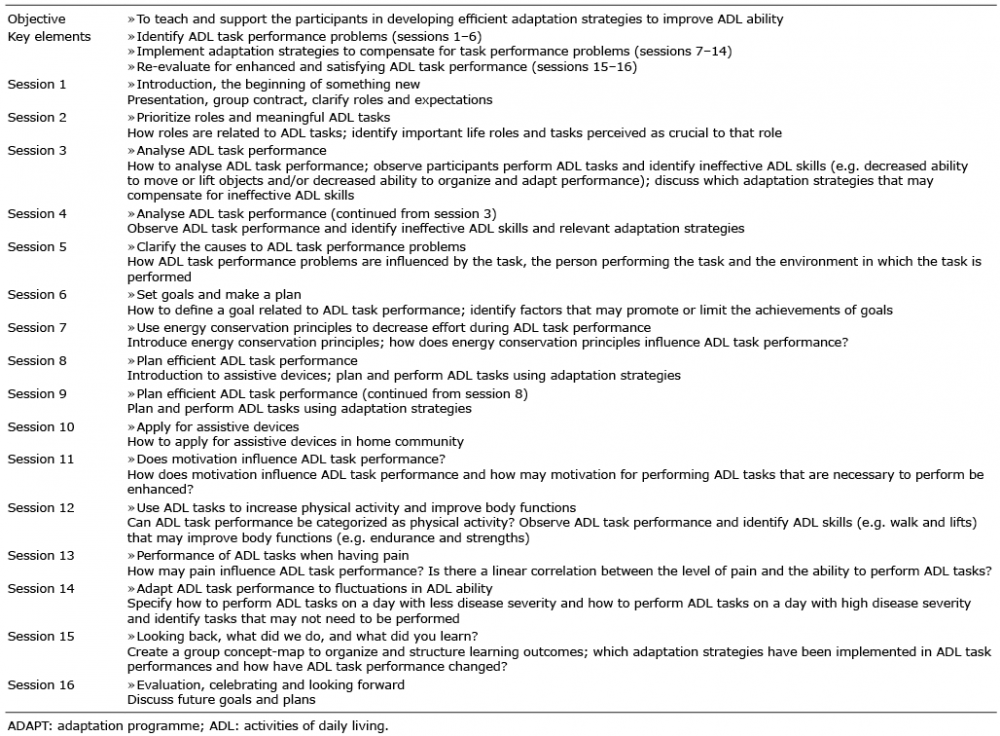 Click to show fullsize
Click to show fullsize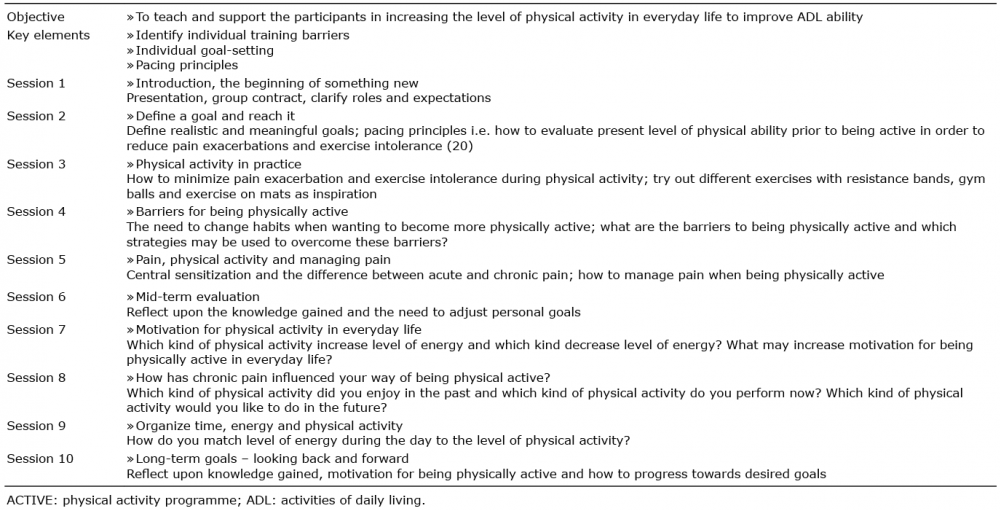 Click to show fullsize
Click to show fullsize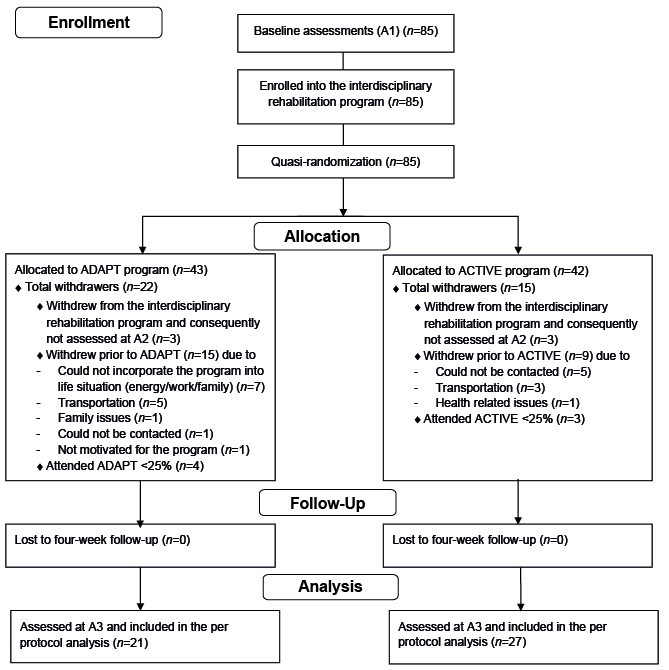 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize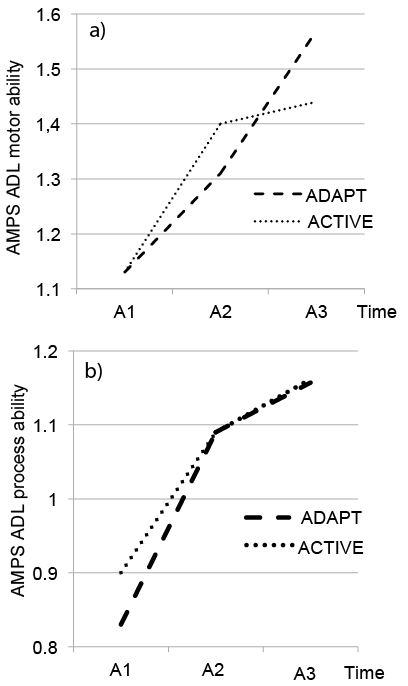 Click to show fullsize
Click to show fullsize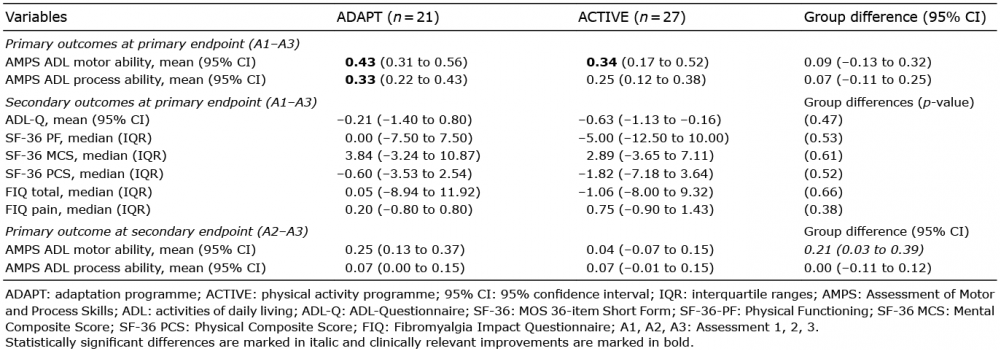 Click to show fullsize
Click to show fullsize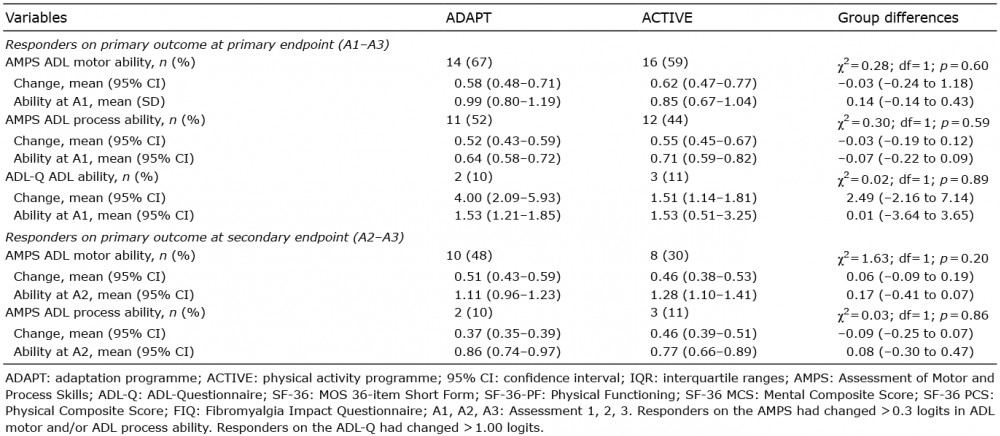 Click to show fullsize
Click to show fullsize