
From the 1Department of Health Studies, College of Applied Sciences “Lavoslav Ruzicka” in Vukovar, Vukovar, 2School of Medicine, Josip Juraj Strossmayer University of Osijek, Osijek, 3School of Medicine, University of Zagreb, 4Department of Obstetrics and Gynecology, University Hospital Centre Zagreb, 5Institute for Expert Evaluation, Professional Rehabilitation and Employment of People with Disabilities, Zagreb, Croatia, 6Southmead Hospital, North Bristol NHS Trust, Bristol, UK and 7Science and Research Centre of Koper, Institute for Kinesiology Research, Koper, Slovenia
Objective: To investigate the effect of a supervised, structured exercise programme on the occurrence and severity of pregnancy-related lumbopelvic pain.
Design: Randomized controlled trial.
Subjects: A total of 45 pregnant women were randomly assigned to 2 groups: an experimental group (n = 20; mean age 32.8 (standard deviation (SD) 3.6) years) and a control group (n = 22; mean age 32.2 years (SD 4.9)).
Methods: Exercise intervention for the experimental group consisted of aerobic and resistance exercises performed bi-weekly from the date of inclusion into the study until the end of pregnancy, together with at least 30 min of brisk daily walks. A numeric rating scale, Roland-Morris Disability Questionnaire (RMDQ), and Pelvic Girdle Questionnaire (PGQ) were used to measure outcomes. The control group received only standard antenatal care.
Results: There were significant differences between the 2 groups on the numeric rating scale, PGQ and RMDQ scores in the 36th week of pregnancy (p = 0.017; p = 0.005; p < 0.001, respectively) in favour of the experimental group.
Conclusion: The exercise programme had a beneficial effect on the severity of lumbopelvic pain in pregnancy, reducing the intensity of pain and the level of disability experienced as a result.
Key words: pregnancy; exercise; low back pain; pelvic girdle pain.
Accepted Dec 6, 2016; Epub ahead of print Feb 24, 2017
J Rehabil Med 2017; 49: 251–257
Correspondence address: Iva Sklempe Kokic, Department of Health Studies, College of Applied Sciences “Lavoslav Ruzicka” in Vukovar, Zupanijska 50, 32000 Vukovar, Croatia. E-mail: iskokic@vevu.hr
Low back pain or pelvic pain (LBPP) during pregnancy is defined as recurrent or continuous pain around the lumbar spine or pelvis that lasts for more than 1 week (1). The pathogenesis and aetiology of LBPP are unclear and probably multifactorial. Several determinants have been identified: altered posture during pregnancy, ligamentous laxity, and fluid retention within connective tissues (2). The main symptom is pain, which usually increases as pregnancy advances, with negative effect on daily activities (3). Furthermore, postpartum depressive symptoms are 3 times more prevalent in women who experience LBPP during pregnancy, compared with those who do not (4).
Pregnant women without contraindications should engage in regular, moderate-intensity physical activity for at least 20–30 min per day on most or all days of the week (5). Observational studies have demonstrated the protective effects of physical activity before pregnancy on the development of lumbopelvic pain (1, 7). However, pregnant women tend to reduce their physical activity levels, and those with lumbopelvic pain are less likely to exercise regularly (6, 8). Inactivity leads to deconditioning and there is a recognized positive association between reduced muscle function and the development of lumbopelvic pain in pregnancy (9).
Lumbopelvic pain usually resolves after delivery. However, 51% of women with pain during pregnancy report experiencing LBPP 1 year postpartum (10), and 20% of women report LBPP 3 years postpartum (11). It has been shown that a higher intensity of pain experienced during pregnancy indicates a worse prognosis after delivery (12). Despite this, the majority of women receive little or no treatment from healthcare providers for lumbopelvic pain in pregnancy (13).
Physiotherapy is the main treatment for LBPP. This includes passive therapies, such as manual therapy, and active treatment, such as therapeutic exercises (14). Further treatment modalities include aquatic therapy, acupuncture, ergonomic advice, and the use of a pelvic belt. Exercise can reduce the intensity of pain, improve function and reduce disability (15, 16). However, there are no specific guidelines regarding the type, duration and frequency of exercise for lumbopelvic pain in pregnancy. A supervised exercise programme is recommended as a first-line treatment for patients with non-specific chronic lower back pain in the non-pregnant population (17). The European guidelines for pelvic girdle pain (PGP) recommend individualized exercises in pregnancy (14). However, the amount of research into the effects of exercise on LBPP is relatively small, with only moderate overall methodological quality. The resulting data is therefore often inconsistent.
The objective of this study was to examine the effect of a supervised, individualized, structured, therapeutic exercise programme, consisting of aerobic and resistance exercises along with daily vigorous walks, on the occurrence and severity of pregnancy-related lumbopelvic pain.
The study was designed as a pre-planned secondary analysis of the data from a randomized controlled trial, the primary purpose of which was to investigate the effects of an exercise programme on outcomes of gestational diabetes mellitus. Ethical approval was obtained from the University Hospital Centre Zagreb and the University Hospital Merkur, Zagreb, Croatia and the trial was registered with Clinicaltrials.gov (NCT 02196571). Participants gave their informed consent and the trial was conducted according to the Declaration of Helsinki.
Subjects were healthy pregnant women or women diagnosed with mild gestational diabetes mellitus treated only by diet and lifestyle change, but with no other medical conditions. They were recruited by direct contact at the 2 above-mentioned hospitals. Inclusion criteria were: pregnancy, age between 20 and 40 years, with the ability to read, understand and speak Croatian. The upper limit for inclusion was set at 30 weeks’ gestation to allow a minimum exercise period of 6 weeks, until at least the 36th week of pregnancy. Exclusion criteria were: a medical history of miscarriages, pharmacological treatment during pregnancy, contraindications for exercise, as set out in the criteria published by the American College of Obstetricians and Gynecologists (ACOG) (18), smoking, previous trauma to the lumbopelvic region, or a history of severe lumbopelvic pain prior to pregnancy. Participants were randomized by block randomization using a computerized service into 2 groups: experimental (EG) and control (CG). The study was not blinded for participants because of its nature; however, the assessors were blinded.
Baseline information, taken at the initial interview, included: demographic and occupational data, medical and obstetric history, lifestyle habits and physical activity levels, height and body mass at the start of the pregnancy, and the existence and onset of pregnancy-related LBPP. Body mass was measured and recorded by a blinded physiotherapist using a medical grade digital scale measuring to the nearest 0.1 kg (Body Composition Monitor BF511, Omron Healtcare, Kyoto, Japan). Body mass index (BMI) was calculated according to the standard equation. Pregnant women randomized to the EG were scheduled for their first exercise session.
Both groups were seen in the 36th week of pregnancy, when their levels of physical activity were recorded using a Pregnancy Physical Activity Questionnaire (PPAQ) (19). The intensity of lumbopelvic pain and level of disability experienced as a result were also measured on this occasion, using a numeric rating scale (NRS), Roland-Morris Disability Questionnaire (RMDQ) and Pelvic Girdle Questionnaire (PGQ). Relevant medical documentation was also reviewed to assess the course of the pregnancy.
An NRS is a reliable and valid method of measuring pain intensity (20). We used the most common 11-item NRS, which is a segmented numeric version of the visual analogue scale (VAS), in which the respondent selects a whole number between 0 (no pain) and 10 (worst pain imaginable) that best reflects the intensity of their pain. The recall period was 1 week (21). The RMDQ is a condition-specific, patient-reported, reliable and valid health status measure for assessment of physical disability due to LBP (22). We used a 24-item version of the RMDQ. The PGQ is the first condition-specific, patient-reported outcome measure developed for people with PGP (23). It has a high reliability and validity in women with PGP during pregnancy.
Women from the EG participated in an individualized, supervised, structured, exercise programme twice per week, along with standard antenatal care. The duration of the exercise session was 50–55 min. They were also instructed to undertake at least 30 min of brisk walking once per day. The exercise programme commenced within 1 week following inclusion into the trial and continued throughout the duration of the pregnancy. Attendance was recorded and the women were asked to keep a diary of daily walks. The minimum duration of the intervention was 6 weeks. The minimum acceptable attendance rate between the time of inclusion into the trial and the 38th week of pregnancy was set at 70%. Participants in the CG received only standard antenatal care, but were not discouraged from exercising on their own.
The exercise programme was developed in accordance with official guidelines for exercise in pregnancy (18). It consisted of aerobic exercise (20 min), resistance exercises (20–25 min), pelvic floor exercises, stretching and relaxation at the end of the session (10 min). The treadmill (Axos Runner, Heinz Kettler GmbH, Ense-Parsit, Germany) was used for the aerobic part of the training. The target exercise intensity was within the aerobic zone (65–75% of maximum heart rate), i.e. 13–14 on the Borg Rating of Perceived Exertion scale (24). Maternal heart rate (HR) was monitored (Mio Alpha, Mio Global, Vancouver, BC, Canada) continuously during the exercise and the target heart rate (THR) was calculated according to Karvonen’s formula. Maximum HR was calculated according the traditional formula 220 – age.
The aerobic part of the exercise programme started with a warm-up for the first 5 min, which included walking on the treadmill at normal pace, gradually adjusting velocity and incline. After that, the women were free to adjust the velocity and incline of the treadmill themselves in order to achieve the desired intensity. Resistance exercises incorporated all major muscle groups at each session. They included stabilization exercises for the lumbopelvic area, exercises for upper and lower limb muscles, back extensors and deep abdominal muscles. Exercises were performed using body weight, elastic bands (TheraBand, The Hygenic Corporation, Akron, OH, USA) and hand-held weights of 0.5 and 1 kg (Aerobic Dumbbels, Heinz Kettler GmbH, Ense-Parsit, Germany). Intensity target values were the same as for the aerobic part of the session. Six different exercises were performed in 3 sets of 10–15 repetitions per set. There were 3 standardized resistance exercise protocols developed and interchanged during the intervention period. Stretching and pelvic floor exercises were performed at the end of every exercise session.
Statistical analyses were performed with SPSS 19.0 (IBM, Armonk, NY, USA). Descriptive statistics were performed for all variables of interest. This included mean, standard deviation and minimum and maximum values, where appropriate. Normality of data was checked with the Shapiro–Wilk test. Homogeneity of variances was checked with Levene’s test. The distribution of data was not normal and we used the 2-tailed Mann–Whitney U test without Bonferroni correction for comparison of baseline participant characteristics, the results of the PPAQ, NRS, RMDQ and PGQ, and onset of lumbopelvic pain. The level of significance was set at p-value < 0.05. Cohen’s d (d) and effect size (r) were calculated for all outcome variables with a significance level ≤ 0.05.
The number of exercise sessions, duration of the intervention in weeks and number of daily walks were correlated with NRS, PGQ and RMDQ scores in the 36th week of pregnancy, using Spearman’s rank correlation coefficient (rs). Point-biserial correlation coefficient (rpbi) was calculated to determine the relationship between the number of exercise sessions, number of daily walks, duration of the intervention in weeks and the onset of lumbopelvic pain.
Initially, a total of 45 pregnant women were enrolled in the trial and randomized into 2 groups. We assigned 22 women to the EG and 23 to the CG. Three participants (6.7%) dropped out of the trial, 2 from the EG (9.1%) and 1 from the CG (4.4%) (Fig. 1). Both groups were well matched (Table I).
Fig. 1. Flow chart of study participants.
Table I. Baseline characteristics for the experimental and control groups
A total of 419 exercise sessions were performed during the trial. The mean (standard deviation (SD)) number of exercise sessions per subject was 21 (SD 7.6). General characteristics of the exercise sessions are detailed in Table II. The mean adherence to protocol was 83.7%. No warning signs or adverse effects caused by exercise were reported. Our primary determinant of exercise intensity was to achieve values 13–14 on the Borg Rating of Perceived Exertion scale, which corresponded with mean of 64.5% (SD 4.7) of maximum heart rate. Participants performed a mean of 84.7 (SD 34.5) brisk walks vs planned 87.9 (SD 33.6). The adherence to protocol was 95.8% (SD 4.4%).
Table II. General characteristics of exercise sessions
Whilst there were no differences between the groups in baseline levels of physical activity (Table I) we found difference in the 36th week of pregnancy (Table III). Pregnant women from the EG recorded higher levels of total activity of light intensity and above (≥ 1.5 METs) (p = 0.027, d =0.63, r = 0.30). Pregnant women from the EG also recorded significantly higher levels of sport/exercise, with a very large effect size (p < 0.001, d = 2.26, r = 0.75). Furthermore, levels of moderate physical activity (3.0–5.9 METs) were higher in the EG in the 36th week of pregnancy (p = 0.014, d = 0.63, r = 0.30). Women from the EG also recorded higher levels of transportation activities (p = 0.027, d = 0.77, r = 0.36) in the 36th week of pregnancy.
Table III. Results of Pregnancy Physical Activity Questionnaire (PPAQ) in the 36th week of pregnancy
There was no significant difference between the groups in the number of women who developed pregnancy-related lumbopelvic pain. However, a lower percentage of women (EG = 55%; 11/20) from the EG developed pain compared with the CG (CG = 81.8%; 18/22; p = 0.064), and only 4/11 after the start of the exercise (36.4% of the total number of women from the EG who developed the pain). Furthermore, there was no significant difference between the groups in the number of women with existing pregnancy-related lumbopelvic pain prior to inclusion in the trial (EG = 35% (7/20) vs CG = 22.7% (5/22)). Women from the EG, however, had an earlier onset of lumbopelvic pain (EG mean 23 weeks (SD 5.4); CG mean 26.7 (SD 5.1)), but without significant difference between groups. Mean start of the exercises was 4 weeks (SD 3.5) after the onset of lumbopelvic pain. The onset of lumbopelvic pain in the EG negatively correlated with both number of performed exercise sessions (rpbi = –0.470, p = 0.036), and duration of the intervention in weeks (rpbi = –0.445, p = 0.049). It also negatively correlated with the number of performed vigorous walks (rpbi = –0.470, p = 0.036).
The result of the numeric rating scale for intensity of pain was significantly lower in the EG in the 36th week of pregnancy (p = 0.017, d = –0.80, r = –0.37). The duration of the intervention negatively correlated with the NRS score (rs = –0.380, p = 0.049), as well as the number of performed walks (rs = –0.415, p = 0.031).
Likewise, there was significant difference in PGQ score in the 36th week (p = 0.005, d = –0.85, r = –0.39) week of pregnancy. The EG had lower scores on the PGQ, i.e. a lower level of disability experienced and fewer symptoms reported (Table IV; Fig. 2). There was a negative correlation between the duration of intervention and PGQ score (rs = –0.380, p = 0.049). Also, the number of exercise sessions and daily walks negatively correlated with PGQ score (rs = –0.419, p =0.033; rs = –0.528, p = 0.008), respectively.
Table IV. Results of numeric rating scale (NRS), Pelvic Girdle Questionnaire (PGQ) and Roland-Morris Disability Questionnaire (RMDQ) in the 36th week of pregnancy
Fig. 2. Results of numeric rating scale (NRS), Pelvic Girdle Questionnaire (PGQ) and Roland-Morris Disability Questionnaire (RMDQ) in the 36th week of pregnancy.
A significant difference in the RMDQ scores was found in the 36th week (p < 0.001, d = –0.90, r = –0.41). Pregnant women from the EG recorded lower scores on RMDQ and experienced a lower level of disability (Table IV; Fig. 2).
Even with an insignificant difference in the percentage of women who developed pregnancy-related lumbopelvic pain, those in the EG were less affected by it and appeared to cope better with it. They reported significantly lower levels of pain, a higher quality of life and experienced lower levels of disability. There was a negative correlation between the number of sessions, duration of the intervention and the severity of lumbopelvic pain, which might implicate a positive dose-response relationship.
To the best of our knowledge, this is the first study to evaluate the effects of an individualized, supervised, exercise programme for pregnancy-related lumbopelvic pain. This study is also one of the few (25–29) to investigate the effect of combining aerobic and resistance exercises. Furthermore, this is the second trial (27) to add daily walking intervention to biweekly exercise sessions.
Levels of adherence to the study protocol were very high. This is probably due to the individualized nature of the programme. Participants were able to choose the time and days of the week that best suited them to attend exercise sessions. In this way, some of the barriers to exercising in pregnancy were removed. Furthermore, none of the participants developed warning signs or experienced adverse effects requiring termination of the exercise programme.
This study found that there was no significant difference between the groups in the rate of self-reported pregnancy-related lumbopelvic pain. However, a lower percentage of women in the EG developed lumbopelvic pain in comparison with the CG (55% vs 81.8%). Still, pre-pregnancy lumbopelvic pain was also different between EG and CG (45 vs 54.5%) and it represents the major risk factor for the development of lumbopelvic pain during pregnancy.
Mørkved et al. (26) also investigated the effect of a supervised exercise programme, which combined aerobic and resistance exercises with similar results. Following the implementation of their intervention (36th week of pregnancy) 43.9% women from the EG vs 56.2% women from the CG reported lumbopelvic pain (p = 0.03). Beyaz et al. (27) also confirmed a lower frequency of LBP in their EG compared with the CG following the implementation of their exercise intervention (p < 0.001).
In contrast, Eggen et al. (30) did not find significant differences in the frequency of self-reported LBP and PGP following their exercise intervention. Neither Stafne et al. (28) found a significant difference in self-reported lumbopelvic pain in the 36th week of pregnancy, following a 12-week exercise programme which combined aerobic and resistance exercises, an intervention similar to ours. Likewise, Miquelutti et al. (31) and Haakstad & Bö. (29) did not find any significant differences in symptoms reported by EG and CG.
Pain intensity, as assessed by the NRS score, was lower in the EG with a large effect size (median 2 vs 4) (p = 0.017, d = –0.80, r = –0.37). A similar intervention, the exercise programme performed from the 2nd trimester of pregnancy until the 37th week of pregnancy, 3 times per week with the addition of daily walks also significantly reduced VAS scores in the exercise group (p < 0.001) and increased them in the control group (p = 0.0001) (27). In contrast, Eggen et al. (30) did not find a significant difference in NRS scores between EG and CG after the implementation of an exercise intervention that consisted of supervised weekly exercise combining aerobic and strengthening exercises for local and global muscle groups lasting between 16 and 20 weeks.
This study found that there was a significant difference in PGQ score between the 2 groups in the 36th week of pregnancy, with the EG recording lower scores on the PGQ (median 1.3 vs 18.7), with a large effect size (p = 0.005, d = –0.85, r = –0.39). The EG had better quality of life and they experienced fewer problems carrying out several activities of daily life often associated with aggravating PGP. Another study (33) examined severity of pelvic girdle pain, assessed by an independent examiner, before and after implementation of an exercise intervention comparing stabilization exercises and acupuncture with standard antenatal care. Both intervention groups reported significantly superior effects to those receiving standard antenatal care alone.
Regarding the RMDQ score, there was also a significant difference in the 36th week, with a large effect size (p < 0.001, d = –0.90, r = –0.41). The EG recorded lower scores on the RMDQ (median 0 vs 3), hence a lower level of disability caused by LBP. In contrast to that, Eggen et al. (30) did not find a significant improvement in RMDQ scores following implementation of their exercise interventions. Mørkved et al. (26) used a Disability Rating Index (DRI) for the assessment of disability experienced and the results were significantly improved in the exercising group following the intervention (p = 0.011). In contrast, Stafne at al. (28) did not find any significant difference in DRI scores between EG and CG following the implementation of an exercise intervention.
The main limitation of this study was the small sample size. However, the nature of the intervention, which included individually supervised exercise sessions, would have been very difficult to implement with a larger number of participants. In addition, there is no data on the exact prevalence of lumbopelvic pain amongst the population of pregnant women in Croatia. As a result it is possible that the population studied is not representative of the general population affected by pregnancy-related lumbopelvic pain. Since these women volunteered to participate in this study it is also possible that there was a selection bias towards those more interested in active and healthy lifestyles.
Another limitation of this study was not distinguishing between LBP and PGP. There are 2 reasons for this: firstly the sample size being studied was relatively small. Secondly, there is currently no single standard diagnostic test for PGP, and it is also not always straightforward to distinguish LBP from PGP, due to the fact that the symptoms often overlap and the 2 conditions can exist at the same time.
Future research should aim to compare the levels of supervision required to achieve an optimal level of adherence to protocol and, therefore, the best possible outcomes. It is predicted that a higher level of supervision and an individualized approach improves participation and outcomes. Future research should, furthermore, investigate the effects of different protocols of exercise, and combinations of aerobic and resistance exercises on short- and long-term outcomes.
In conclusion, the data suggest that exercise offers significant benefits for pregnant women in reducing LBPP, specifically beneficial effects on severity of pain, and thus on the functional abilities and quality of life of the women affected. Further prospective studies are needed to confirm these findings.
The authors declare no conflicts of interest.


 Click to show fullsize
Click to show fullsize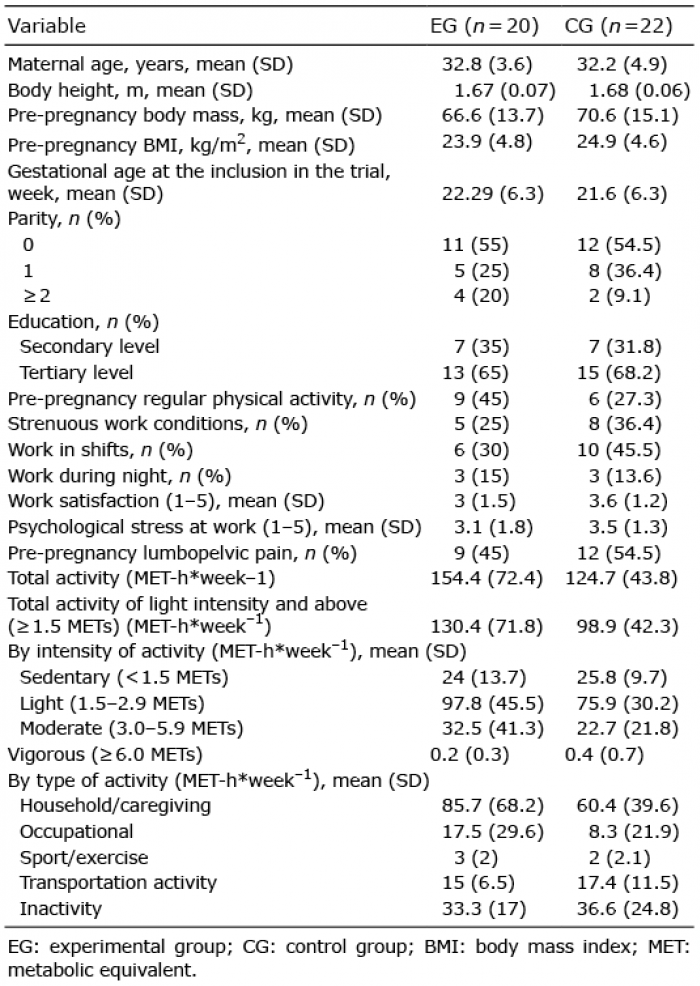 Click to show fullsize
Click to show fullsize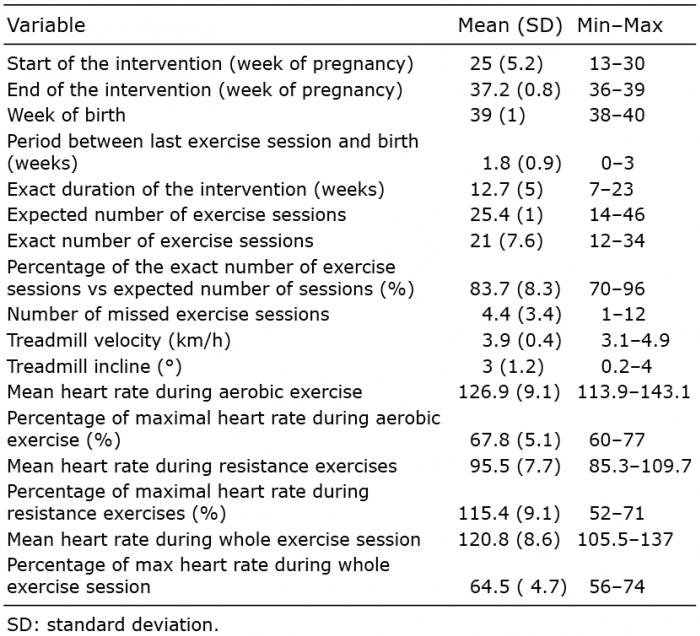 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize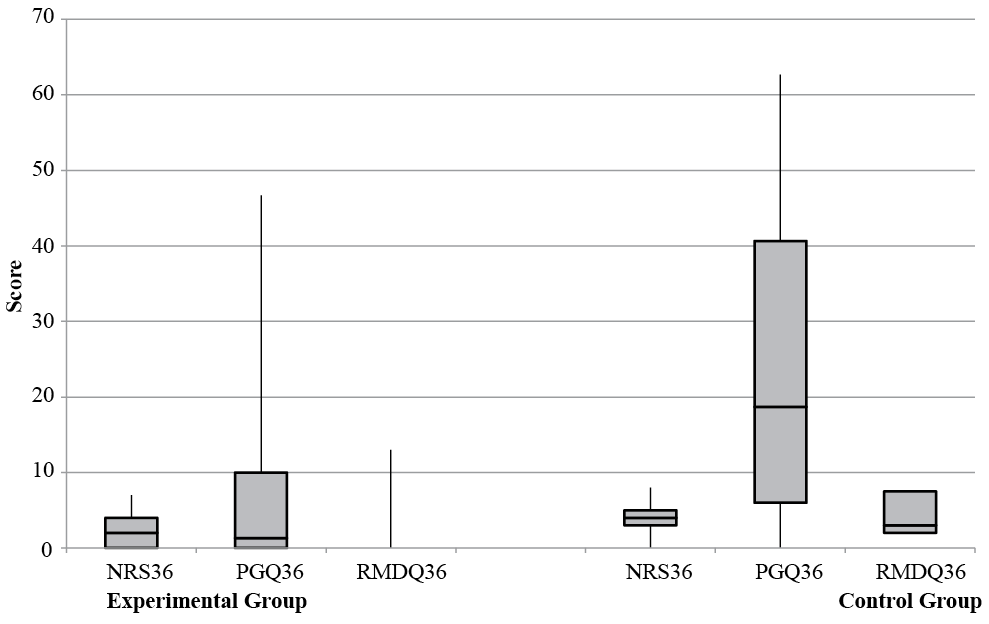 Click to show fullsize
Click to show fullsize