
From the 1Department of Public Health and Caring Sciences, Uppsala University, Sweden and 2Centre for Clinical Research Dalarna, Uppsala University, Falun, Sweden
Objective: Mental illness and chronic pain are common reasons for long-term sick leave, typically more so for women. This study investigated the effects on return to work of 2 vocational rehabilitation programmes.
Methods: In this randomized controlled study, 308 women were allocated to treatment with acceptance and commitment therapy, to multidisciplinary assessment and individualized rehabilitation interventions, or to a control group. Return-to-work at 12 months was assessed as: (i) returning to health insurance; (ii) number of reimbursed health insurance days during follow-up; (iii) self-reported change in working hours; (iv) a composite measure of self-reported change in work-related engagement.
Results: The mean age of the Swedish study population was 48.5 years (standard deviation (SD) 6.3 years) and the mean time on sick leave 7.5 years (SD 3.2 years). There were no significant differences in reimbursed days or returning to the health insurance at 12 months. The multidisciplinary assessment and individualized rehabilitation interventions group, compared with control, reported a significant increase in working hours per week, as well as a significant increase in work-related engagement.
Conclusion: Multidisciplinary assessments and individual rehabilitation interventions may improve the chance of return-to-work in women with long-term sick leave due to pain condition or mental illness.
Key words: return to work; vocational rehabilitation; multi-disciplinary rehabilitation; acceptance and commitment therapy, chronic pain.
Accepted Nov 4, 2016: Epub ahead of print Jan 18, 2017
J Rehabil Med 2017; 49: 170–177
Correspondence address: Per Lytsy, Department of Public Health and Caring Sciences, Husargatan 3, Box 564, SE-75122, Uppsala University, Sweden. E-mail: per.lytsy@pubcare.uu.se
Mental illness (1) and chronic pain (2) are common causes of long-term sick leave in many Western countries and these conditions are major public health and occupational health challenges.
Different types of interventions aim to facilitate return-to-work (RTW) for people on long-term sick leave. The interventions include mono-therapy approaches, such as psychotherapy with cognitive behaviour therapy, as well as multidisciplinary or multimodal rehabilitation approaches. The present study investigates the effect of 2 vocational rehabilitation programmes, 1 being mono-therapy with acceptance and commitment therapy (ACT), a form of cognitive behavioural therapy that uses acceptance and mindfulness strategies together with behavioural strategies to increase function and quality of life (3). ACT is believed to have a mediating role of acceptance of symptoms (4), improving functional status in patients with chronic pain (5, 6) also when used in interdisciplinary program of rehabilitation (7). ACT has also been shown to have an effect on patients with mental disorders, such as anxiety (8), social phobia (9) and depression (10).
The other programme tested was multidisciplinary assessments and individual rehabilitation interventions, meaning that a patient met with several health professionals, assessing symptoms, disability and functioning from different perspectives. The multidisciplinary approach seems to be effective in reducing disability and improving time to RTW in patients with chronic pain (11, 12) as well as in multiple target groups (13). The multidisciplinary approach seems to further reduce persistent work-related stress (14) and increase chances of RTW (14, 15).
The present RTW study was conducted in Sweden and targeted women on long-term sick leave for pain syndrome and/or psychiatric disease, which are known to be of high comorbidity (2, 16), in whom psychiatric disease is the most common reason for long-term sick leave (17). The health insurance regulation was reformed in Sweden in 2008, introducing a maximum of 365 refunded days within a 450-day period. During 2010–2012 approximately 40,000 people reached the maximum time in the health insurance and were transferred to the public employment insurance system.
This randomized controlled study investigated the effect on RTW of 2 vocational rehabilitation interventions in women reaching their maximum time in the health insurance system.
The hypotheses were that persons in the 2 interventions groups, compared separately with the control group, would be less likely to have used health insurance benefit or to have returned to health insurance at the 12-month follow-up. Further hypotheses were that persons in the intervention groups would have increased their working time as well as having increased their degree of work-related engagement, which was a composite measure of increased work time/work training/work rehabilitation activity and studying.
This randomized controlled intervention study compared 2 intervention groups with 1 control group. All women in Uppsala County on sick leave or time-restricted disability pension due to mental illness and/or pain syndromes who were about to reach the newly set maximum sick leave, were eligible for the study. The study was conducted between 2010 and 2012.
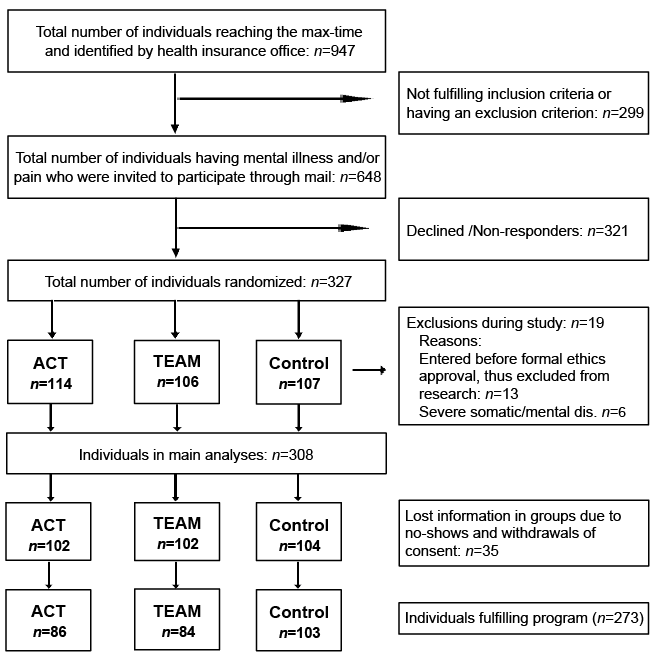
The Uppsala office of the Swedish Social Insurance Agency identified a total of 947 women who were expected to reach their maximum time of sick leave between June 2010 and June 2011. Persons with clearly non-included diagnoses (n = 114) were omitted by the Social Insurance Office administration. The remainder had their doctors’ certificates screened by a physician and an occupational therapist or psychologist in order to determine fulfilment of the inclusion criteria, being: (i) on sick leave for a pain syndrome and/or a mental illness; (ii) aged between 20 and 64 years; as well as not fulfilling the exclusion criteria, being: (i) at high suicidal risk; (ii) having ongoing alcohol/substance abuse; (iii) having major mental disorder (schizophrenia, bipolar disorder type I, severe social dysfunction/personality disorder); (iv) currently in psychotherapy or other structured vocational rehabilitation programme, according to information from the doctors’ certificates.
A total of 185 subjects were excluded at screening, mainly due to being on sick leave due to non-inclusive diagnoses. After screening and exclusion, a total of 648 women were contacted by post to receive information about the project and were invited to participate. A total of 176 did not respond and 145 responded but declined to participate. The remaining 327 women gave consent to participate and were block randomized in even triplets (the first 13 were straight randomized) by the central Swedish Social Insurance Agency to: (i) control group; (ii) multidisciplinary assessments and individual rehabilitation interventions (TEAM); or (iii) psychological treatment with acceptance and commitment therapy (ACT). Inclusion, randomization and allocation were performed consecutively during the project and all participants had an equal chance of being allocated to either group. The first 13 were excluded from the study due to being contacted before the formal approval by the ethics committee. Six individuals were excluded from the project in the early stage for having too severe somatic or psychiatric disease, being in a concurring rehabilitation programme or withdrawing consent. Thus the final sample comprised 308 individuals allocated to ACT (n = 102), TEAM (n = 102) or control group (n = 104) group (Fig. 1).
Fig. 1. Flow-chart of inclusion and exclusion procedure. ACT: acceptance and commitment therapy; TEAM: multidisciplinary assessment and individualized rehabilitation intervention.
No formal power-analysis was conducted. The project included participants over a 1-year period, during which all eligible patients were invited to participate. All participants provided written informed consent to the study, which was approved by the regional ethics committee Uppsala (Dnr 2010/088).
The 2 intervention groups were treated with multidisciplinary assessments and individual rehabilitation interventions or ACT. Both interventions started 1–3 months ahead of each participant’s expected transferral to the employment insurance system. The lengths of the interventions were individualized and could continue over the project time of one year. In addition to the interventions, all participants also obtained scheduled collaboration meetings with their administrator at the employment office and their contact person in the project. The control group did not receive any planned intervention, but were free to receive “usual care” provided by their regular health contacts. The control group was followed with the same questionnaires as the intervention groups. The control group did not receive any collaboration meeting support and went through the usual procedures when transferred from health insurance to employment insurance.
The multidisciplinary team consisted of a physician, a psychologist, an occupational therapist and a social worker. Each team member met with the participant separately at the clinic for a 1.5–2 h meeting to assess the situation from each speciality’s perspective. The team members then met without the participant to consider the situation as well as the participant’s strengths and hindrances for returning to work. The team agreed, using consensus, on an individualized rehabilitation plan with suggested interventions, such as further medical investigation/treatment, physiotherapy, evaluation and training by an occupational therapist and social and economic counselling by a social worker. A contact person, being one of the team members, then brought the plan back to the participant. The participants had the choice of accepting the whole, none or parts of the plan. The team met weekly during the project time to evaluate the situation and to synchronize the planned or ongoing activities for each participant.
ACT is a form of cognitive behavioural therapy that uses acceptance and mindfulness strategies, together with behavioural strategies, to increase function and quality of life rather than decreasing symptoms (3). Participants in the ACT group received only treatment with ACT; in the TEAM group ACT was an option if suggested by the team. Most psychotherapy sessions, for both the TEAM and ACT group, occurred at the clinic, but there was a possibility to schedule sessions at the participant’s home, work or elsewhere. Sessions were typically approximately 1 h long.
All participants received a structured collaboration with the local social insurance office and the local unemployment office. The contact person, from the team or the ACT therapist in the ACT group, participated at the meetings with representatives of the health and unemployment offices together with the participant. The main objective was to increase the individual’s commitment to being an active participant in the rehabilitation process. Another purpose was to establish agreement on the RTW goal for the participant as well as for the participating organizations.
Baseline data on age, sick leave diagnoses (from standard and extensive health certificate), length of sick leave, employment status, type and magnitude of reimbursement were collected from the social insurance agency register. Most participants had, according to the certificates, several sick leave diagnoses believed to affect their work status; a physician used them to classify each participant’s main problem as either psychiatric, pain-related or both. The total number of International Statistical Classification of Diseases and Related Health Problems (ICD-10) as well as number of M and F diagnoses were assessed from the extended sick leave certificate, which existed for all participants.
The participants were followed up with postal questionnaires at 0 (response rate 87%) and 12 months (response rate 67%) assessing various aspects of their health and social situation as well as their motivation to RTW. Health was assessed using validated instruments of Hospital Anxiety and Depression Scale (HADS) (18), General Health Questionnaire (GHQ-12) (19), General Self-efficacy Scale (20), and Satisfaction With Life Scale (SWLS) (21). Pain was assessed with the question “Do you have pain? (yes/no)”. If they did have pain the respondents were asked to rate the past week’s pain as well as the mean pain over the past 3 months, each on a 0–10 scale using question 8 and 9 in the Linton pain screening questionnaire (22). Activity was assessed using questions 12–16 from the same screening questionnaire and an activity score ranging from 0 to 50 was calculated.(22)
Alcohol risk use was assessed using the summed score of AUDIT-C with a cut-off of ≥ 3 (women) (23). Queries about the use of pharmaceuticals were phrased as 4 separate questions: “Do you use: antidepressant medication/tranquillizers/sedatives/analgesics?”
Self-reported work, work training and participation in organized rehabilitation activities, currently and 12-months previously, were assessed at 12-month follow-up using the questions with the structure: “How many hours a week do you... ...now/1 year ago”. The questions on studying were assessed at 12-month follow-up and were phrased: “Are you a student today/12 months ago.” Answers were phrased “No”, “Part-time” and “Full-time”.
Participants who received interventions (ACT or TEAM group) performed a self-rating Montgomery Asberg Depression Rating Scale (MADRS) (24) at their first clinical visit. The Mini-International Neuropsychiatric Interview (MINI) (25) was used for screening of psychiatric disease by a physician or psychologist in the intervention groups.
Other studies have used the study population to describe baseline health measures (26) and investigate predictors of self-efficacy (27). The effect of the interventions on different aspects of health will be published separately.
Four outcome measures were used to assess the effect of the interventions on RTW at 12 months; 2 using register data from the health insurance system and 2 using self-reported data on working hours and changes in work-related engagement. The 4 outcomes were:
Differences in baseline characteristics between each intervention group and the control group were investigated using χ2 tests for proportions and t-tests for continuous data. The 4 outcomes were tested using regression modelling; logistic regressions for the dichotomous outcomes (1 and 4) and ordinal regressions for the ordinal outcomes (2 and 3). Assumptions of proportional odds were found to be valid for ordinal regressions. Results were presented as odds ratios (OR) with 95% confidence intervals (95% CI). Intention-to-treat-analyses were performed for complete register-based data (outcomes 1 and 2) and complete cases from responders were used for self-reported data. All tests were 2-sided and a level of p < 0.05 was considered statistically significant. Statistical analyses were performed using SPSS statistics (IBM Corp., Armonk, New York, USA), version 22.0.
The study population’s mean age was 48.5 years (standard deviation (SD) 6.3) and their mean duration of sick leave was 7.5 years (SD 3.2). Approximately two-thirds of the study population were employed and most participants (51.3%) had full sick reimbursement (100%) from the health insurance system when entering the study.
At baseline, approximately one-third of subjects were on sick leave with a psychiatric diagnosis, approximately one-third with pain condition diagnosis, and approximately one-third due to a combination of pain and psychiatric illness. Most participants had several ICD-10 diagnoses (on mean 2.8 (SD 1.4) for total group), assessed by the physician to affect functioning and work ability. The 5 most common pain-related diagnoses in the musculoskeletal system and connective tissue (M-group) were M79, M54, M51, M53 and M25. The 5 most common mental and behavioural disorders groups (F-group) were F32, F43, F41, F33 and F34 (see Table I).
Table I. Baseline study group characteristics, by group allocation and total
Screening of mental illness in the interventions groups using a structured diagnostic psychiatric interview (25) showed high levels of suspected depression as well as other psychiatric comorbidity. For the total group there was a high self-reported use of analgesics (74.1%), anti-depressants (42.2%) and sedatives (33.3%), as well as high-risk use of alcohol. Baseline characteristics were well balanced between the study groups and the control group, (see Table I).
Treatment with ACT was scheduled for all participants in the ACT group and for 60% in the TEAM group. The mean number of ACT sessions was 10.0 (range 1–38) in the ACT group and 9.2 (range 1–31) for those receiving ACT in the TEAM group. The TEAM participants further received evaluation and training from an occupational therapist (72%, mean number of meetings 3.7; range 1–20); counselling from a social worker (36%, mean number of meetings 6.5; range 1–20). Additional medical attention from a physician, other than the initial meeting, was received in 41% of the participants; such actions typically included more thorough examinations/tests and/or referral/contact with other medical health specialists. Several participants in the ACT (n = 16) and TEAM (n = 18) groups chose, despite reminders, not to attend the clinic. Thus, only 86 (82%) in the ACT group and 84 (86%) in the TEAM received the interventions as planned.
At 12-month follow-up, 51.5% of participants in the control group had returned to the health insurance system (outcome 1), compared with 43.5% in the ACT group (OR 0.72, 95% CI 0.41–1.24, p = 0.23) and 39.2% in the TEAM group (OR 0.61 95% CI 0.35–1.06, p = 0.079) (Tables II and III).
Table II. Descriptive results of return to work outcome measures at 12-month follow-up
Table III. Logistic and ordinal regressions of the 4 outcomes in acceptance and commitment therapy (ACT) and multidisciplinary assessment and individualized rehabilitation interventions (TEAM) groups compared with control
The median and mean number of reimbursed days from the healthcare system for groups is shown in Table II. Regression modelling of outcome 2 did not reveal any substantial group effects (Table III).
The change in self-reported working time (outcome 3) was assessed in 195 individuals (63%) and the variable ranged from –25 to +40 h per week for the total group, where 20 participants (10%) had decreased their working time, 124 (64%) reported no change, and 51 (26%) reported increased working time. Regression analysis showed that the ACT group had an OR of 0.95 (95% CI 0.46–1.95, p = 0.90) for increasing their working time compared with control. The corresponding numbers for the TEAM group was OR 2.20 (95% CI 1.09–4.44, p = 0.028) (Table III).
The composite measure of self-reported change in degree of engagement (outcome 4) was assessed in 195 participants (63%). In the total group 40% reported increased and 60% not increased degree of engagement. In the control group 29.9% reported increased engagement compared with 40.3% in the ACT group (OR 1.59 95% CI 0.77–3.29, p = 0.21) and 50.8% in the TEAM group (OR 2.20 95% CI 1.19–4.95, p = 0.015) (Tables II and III).
The major findings of all outcome measures remained alike or were somewhat strengthened when analyses were restricted only to subjects actually receiving any intervention, defined as attending at least once. There was no data on the 6 excluded participants, but including them in a worst-case scenario analysis (in which their outcomes were set to “no” or “worsening of effect” for these 6 participants) lowered the effect for outcome 3 to 1.87 (95% CI 0.95–3.71, p = 0.072) and for outcome 4 to OR 2.28 (95% CI 1.12–4.64, p = 0.023).
The aim of this study was to investigate the effects of 2 vocational rehabilitation interventions on RTW for women on long-term sick absence due to pain and/or mental illness, where different outcome measures were used as indicators of RTW, improved working time or working ability. The study population had a very long (a mean of 7.5 years) history of full-time or part-time sick leave, and at the time of study inclusion they were about to lose their sickness benefits. It is believed that these circumstances led to inclusion of some participants who otherwise would not have been interested in vocational rehabilitation, thus creating a study population with relatively low motivation and belief in their own ability of ever returning to work. Since long absence from the labour market is also a known risk factor for failure of RTW (28, 29), the present project was believed to target a difficult group.
There were no statistically significant findings regarding the outcomes based on register data from the health insurance office (outcomes 1 and 2), although there was a trend in the TEAM group of a lesser proportion of participants returning to the health insurance at 1 year (39.2% vs 51.5%, p = 0.079; Table III). The trend of favourable effect in the TEAM group is supported by an independent evaluation of the cost-effectiveness of the project, performed by the analytic department of the Swedish Social Insurance Agency. In their analysis, using available follow-up periods of between 12 and 30 months, they found a mean reduction of 26% in reimbursed sick leave days in the TEAM group compared with the control group and concluded that, with projected benefits longer than the follow-up period, this suggests an overall net benefit (30).
The suggested positive effects in the TEAM group were supported by the self-reported measures in the present study, where the TEAM group reported both having a greater chance of reporting increased working hours as well as increased work-related degree of engagement. There is evidence that multidisciplinary treatment has an effect in chronic pain (31) as well as in persons with work-related stress (14). The differences in proportions of TEAM participants compared with control group participants reporting increased working time (16.1 percentage points higher in the TEAM group) and increased activity (20.9 percentage points higher in the TEAM group) are considered clinically significant, especially considering the study groups’ long history of sick leave. Altogether, the different ways of measuring indicators of RTW and increased working ability all point to a potential effect in the TEAM group.
The main characteristic of the TEAM intervention was the possibility of focusing the intervention on different domains, each containing potential hindrances for RTW. Such an approach is very flexible. It allows consideration of the therapeutic relationship when deciding on suggested actions, i.e. focusing on contacts between a health professional and a participant based on their mutual agreement and understanding. The findings add to the evidence that multidisciplinary interventions, such as vocational rehabilitation, may increase RTW in patients with mental illness and pain (32, 33).
This study did not include any work-directed intervention, which is a factor seen to increase chances of RTW goals (34). Most participants (approximately 64%) in the present study had an employer, but for the rest even a successful intervention, improving work ability, would leave the participant in a highly competitive labour market, with an unemployment rate at the time of approximately 8%. Future studies of multidisciplinary assessment and individual RTW interventions may consider combining health interventions with work-directed interventions; for instance, within the concept of individualized placement and support (IPS) (35, 36).
The strengths of this study include the randomized prospective controlled design. The balance in baseline characteristics between groups suggests that the observed effects may be attributed to the interventions. However, unmeasured potential confounders, such as actions, including treatments, which were initiated outside the programme, may exist. Also, persons in the control groups seemed to have lower activity levels in 1 measure at baseline, which could affect their RTW ability. Participants in the control group did not have MADRS or a neuropsychiatric interview performed.
Other limitations involve how to measure RTW in a reliable way. The 2 first outcomes in this study are based on register data. The main advantage of register data is its reliability and that there was no attrition. The main disadvantage is that not having returned to the health insurance is only a proxy for working. There are other reasons why participants have not returned; these include if they live on social economic support, loans or savings, etc. However, it is reasonable to assume that randomization would equalize such effects across groups, which would then suggest that the observed differences may be attributed to the interventions.
The other outcome measures are based on self-reported data and, as such, one may question their accuracy and loss of information due to lower response rates. The self-reported change in working hours and “degree of engagement” was assessed at the 12-month follow-up, which means there is a potential risk of recall bias. Furthermore, the variable measuring change in engagement is a composite measure, which may thus be unclear. We believe, however, that measures of hard RTW outcomes are too insensitive in capturing subtle changes that have moved an individual closer to achieving competitive work. Such changes may include studying and work-related activities, which is why we see the composite measure as an important measure complementing other ways of measuring RTW.
There was a high number of persons not showing up or dropping out. There could be different reasons for this; both that participants in fact did not want to be part of the programme, were too sick to participate, or judged themselves to have a problem that would not benefit from the programme.
Another potential problem with this study is that it combines 2 types of intervention, in which participants in the treatment groups received individual treatment as well as organizational collaboration. This raises the question of which of these interventions mediates the effect, if any. The reason to include organizational collaboration was to set and mutually agree on each individual’s RTW goal. This was seen as an important contributor to success. The fact that participants in both the ACT and TEAM group received the same organizational collaboration, but only the latter group showed an effect on some of the outcome measures, suggests that organizational collaboration alone is not enough and that the effect seen in the TEAM group may be attributed to the multidisciplinary assessments and individual rehabilitation interventions.
A further limitation involves the generalizability of the results. Although many western countries experience problems with increasing long-term sick leave due to pain syndromes or mental illness, different work and insurance systems may have key effects on an individual’s motivation and possibilities of returning to work.
This randomized controlled study of vocational rehabilitation in women with long-term sick leave due to pain condition and/or non-psychotic mental illness found preliminary evidence that multidisciplinary assessments and individual rehabilitation interventions increase the possibility of coming off health insurance and returning to work.
The authors are grateful for financial support from REHSAM, a research programme financed by the Swedish Ministry of Health and Social Affairs, the National Insurance Office, the Swedish Association of Local Authorities and Regions and Vårdalstiftelsen. The funding organizations had no part in the planning of the study or the collection, analysis and interpretation of the data.
The authors would like to thank Ms Lill Haglund, at the local social insurance agency office, for assistance acquiring register data.
The author declare no conflicts of interest.


 Click to show fullsize
Click to show fullsize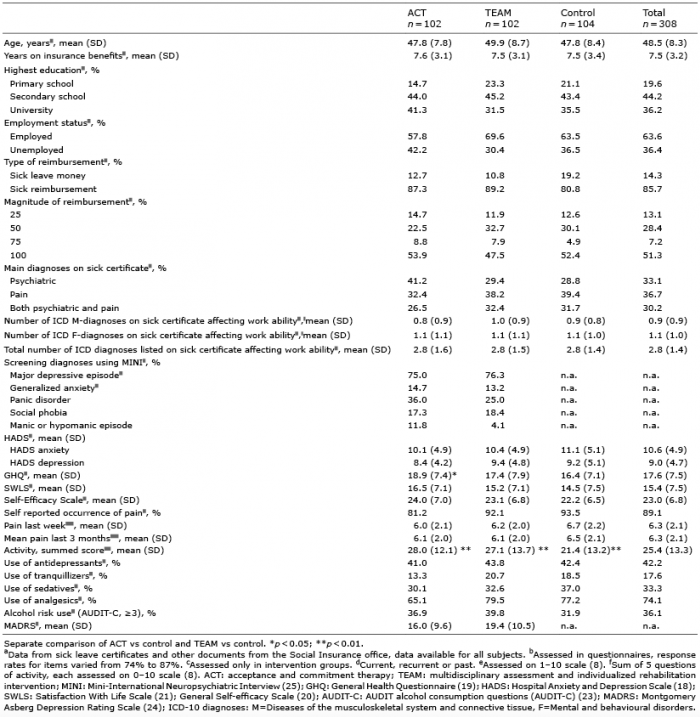 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize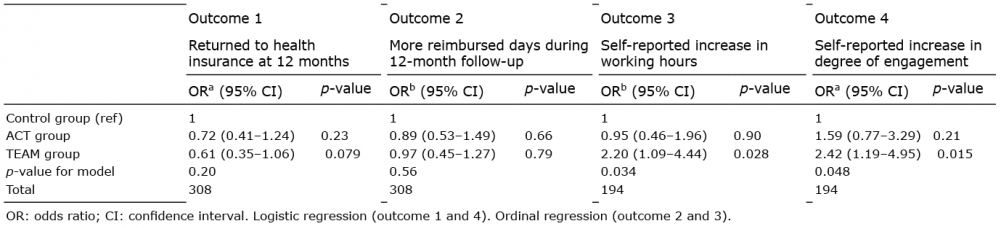 Click to show fullsize
Click to show fullsize