
From the Departments of 1Dalhousie Medicine New Brunswick, Saint John, 2Stan Cassidy Centre for Rehabilitation, Fredericton and 3Team Canada Healing Hands, Canada
Objective: To describe a 6-month follow-up of a specialized paediatric wheelchair and seating programme in Haiti.
Design: Descriptive design using a structured survey and open-ended questions.
Methods: Concurrent with a seating and wheelchair programme conducted in northern Haiti, beneficiaries and their families were introduced to the study, and 86 of 91 consented to future contact. A survey was developed with input from international and local partners, and administered by face-to-face or telephone interviews. Donated wheelchairs were assessed in 5 categories: wheelchair utilization, maintenance, fit, environmental access, and perceived benefits of wheelchair use.
Results: A total of 57 beneficiaries (age range < 2–31 years) were located 6 months after receiving their custom-fit wheelchair and consented to the survey. All respondents still had the wheelchair, 70.2% were using it a minimum of 3–5 days/week, 17.5% were using it < 3 days/week and 12.3% were not using it at all. Primary reasons for not using the wheelchair were that it was broken, uncomfortable, or difficult to transport. The commonly reported benefits were improved mobility, independence, participation and social interaction.
Conclusion: The majority of people who received customized wheelchairs continued to use their equipment 6 months later, with predominantly beneficial outcomes. In future seating initiatives in low-resource settings, efforts to optimize equipment durability and training of local technicians should be supported and evaluated.
Key words: wheelchair; developing country; Haiti; rehabilitation; disabled person.
Accepted Oct 27, 2016; Epub ahead of print Jan 18, 2017
J Rehabil Med 2017; 49: 178–184
Correspondence address: Emma Sumner, Dalhousie Medicine New Brunswick, E2K 5E2 Saint John, Canada. E-mail: emma.sumner@dal.ca
Wheelchairs improve the lives of people with disabilities by enabling independent mobility, employment, and equal participation in community life. There is a direct relationship between improvements in these areas, reduction in poverty, and an increase in overall health (1–3). Wheelchairs and other mobility aids are also linked to preventing premature morbidity and mortality (4). There are more than 1 billion people in the world living with a disability; 15% of the global population (1). Of those 1 billion, 80% live in low-resource countries. It is estimated that the number of people with disabilities in developing countries who need a wheelchair is approximately 1% of the population (1, 4, 5). Affordability is one of the many barriers to accessing mobility devices in low-resource countries, particularly considering the well-described relationship between poverty and disability (1, 2, 4, 6–9). Rehabilitation services, including assessment, fitting/adjustment, user training, follow-up and maintenance and repair, are often in short supply, and the production of mobility devices in poorer countries is lacking (4, 6). Thus, many countries rely on charitable and external donations, but unfortunately donated wheelchairs are too often inappropriate for user’s requirements (6, 10–12). The 2008 Guidelines on the Provision of Manual Wheelchairs in Less-Resourced Countries published by the World Health Organization (WHO) define an appropriate wheelchair as one that meets the user’s needs and environmental conditions, provides proper support and fit, is safe and durable, is available, and can be maintained affordably in the country (6).
There is a clear ongoing need for improved access to appropriate mobility devices and rehabilitation services in low-resource countries (6, 10, 11). In Haiti, half of the 10 million population lacks access to basic healthcare, and access to specialized services is even scarcer (13, 14). Haiti ranked 168 out of 187 countries on the 2014 Human Development Index, with 50.2% of the population living in “multidimensional poverty” (15). The 2010 earthquake in Haiti greatly increased the need for assistive technologies and rehabilitation services, yet the capacity of the country to meet these needs remains disproportionate (7, 13, 16–18), with ongoing reliance on non-governmental aid organizations for such services.
Team Canada Healing Hands (TCHH) is a not-for-profit, registered Canadian charity that has been working in Haiti since 2002, focusing on rehabilitation education, training, and care (19). They were intimately involved in the Haiti disaster response efforts, and have regularly sent teams who work with local rehabilitation clinics and hospitals, providing mentoring, training and collaborative care, including complex seating clinics. For a 2014 paediatric seating programme, TCHH therapists assessed and fitted 91 children with donated specialized wheelchairs in collaboration with a local rehabilitation programme in Northern Haiti.
In order to advance our knowledge of how to address the need for improved access to wheelchairs most effectively, the WHO recommends follow-up of wheelchair provision in low-resource countries (6), and the WHO Global Disability Action Plan 2014–2021 calls for more data collection and research on disability and more sustainable rehabilitation programmes (20). The aim of this study was to follow-up the described seating programme in northern Haiti, with a broader goal of collecting and describing data on the experiences of beneficiaries to better inform future guidelines and best practices of wheelchair provision in low-resource settings.
A descriptive survey was conducted using a structured questionnaire developed by the researchers specifically for this study. The Horizon Health Network Research Ethics Board granted approval for the study. The Haiti Hospital Appeal provided permission and facilitation for the study.
Working in partnership with local rehabilitation organizations, hospitals, the Bureau du Secrétaire d’Etat à l’Intégration des Personnes Handicapées (BSEIPH) and other local care providers, TCHH provided seating assessments and customized, donated wheelchairs to 91 beneficiaries near Cap Haitien, Haiti. Beneficiaries of the seating programme were mostly paediatric and non-ambulatory, referred from the BSEIPH, local orphanages, rehabilitation programmes, and respite care programmes. Demographic data was collected, such as name, age, sex and address, and the most responsible diagnosis and wheelchair measurements were recorded for future reference. The majority of patients were diagnosed with cerebral palsy, including other diagnoses, such as spina bifida, hydrocephalus, muscular dystrophy and spinal cord injury.
Wheelchair education was provided to families and other caregivers and staff at the local rehabilitation centre. The training focused on proper wheelchair fitting and adjustment, positioning, and basic maintenance. Clinics were held during a 1-week period and conducted by a team of Canadian rehabilitation and seating experts, including occupational therapists and physiotherapists, seating technicians, and physiatrists, along with local care providers.
At the time of the seating programme, clinicians informed beneficiaries of the study, and asked for their consent to be contacted 6 months later for a follow-up interview. The adult (15+ years) literacy rate in Haiti is 49% (UNESCO, 2011), and as such the informed consent process was verbal, accompanied by a witnessed signature. If the beneficiary did not have the capacity to provide informed consent (based on age and cognitive capacity), it was obtained from a parent/caregiver. Eighty-six of the wheelchair recipients or their parent/guardian provided informed consent to be contacted for a 6-month follow-up interview. The inclusion criteria for participants in the study were that they (or their caregiver) must: (i) have received a wheelchair in the 2014 TCHH seating programme; (ii) be able to understand English, French or Haitian Creole and be able to follow verbal instructions; and (iii) have capacity to provide informed consent.
The survey tool (See Supplement I) was a structured, 28-item questionnaire developed by the research team and TCHH, in cooperation with international aid organizations involved in wheelchair initiatives and local (Haitian) rehabilitation clinics. Information from a combination of literature review and input from seating experts, such as occupational therapists and seating technicians, as well as from non-governmental organizations (NGOs) and other partner organizations involved in wheelchair service, was used to guide development of the survey. These stakeholders were contacted initially to inform them of the project and enquire as to whether the results of such a survey would be valuable to their organizations and, specifically, what information from wheelchair beneficiaries and their families would be most useful in planning and evaluating future programmes.
The survey comprised 20 multiple-choice questions and 8 open-ended questions. An option of “other” was also included in many multiple-choice questions in order to provide the opportunity for additional comments. The survey items were divided into the following 5 main categories: wheelchair use (including extent of use, location of use, and barriers to use), wheelchair maintenance, wheelchair fit, environmental access, and benefits of wheelchair acquisition and use.
The final categories and survey items were selected based largely on the aims of the study, and therefore the information needs of the TCHH seating team and other seating experts. Questions about frequency and location of wheelchair use were included to characterize whether the utility of the wheelchair was truly as an adaptive aid being used to support and assist the person it was provided for, or whether it was serving a different purpose. Investigating barriers of use, including environmental barriers, was important in order to guide appropriate changes to future seating initiatives that could address such issues. The 2014 seating programme in Haiti was the first TCHH programme that had included formal training for local partners in wheelchair repair, thus gathering information about wheelchair maintenance was crucial to determine the advantages of such training, as well as whether the parts most commonly in need of repair could be sourced or repaired locally, which could affect the types of wheelchairs provided in future programmes. Durability of wheelchair fit and support following the seating clinic is also valuable information, because if the appropriate fit is not easily locally maintained without the assistance of seating experts then further training in this area would be indicated. Exploring the benefits of the wheelchair was imperative to determine whether the goals of the wheelchair donation and seating assessment were being met.
The survey was translated by bilingual staff at the local office of a prominent TCHH partner, Haiti Hospital Appeal (HHA). Translation and comprehensibility of survey items was then verified through back-translation by the trained Haitian translator who was employed with the original seating programme.
Six months after the seating clinics, the research team travelled to Haiti, hosted by the partner hospital in Cap Haitien. With assistance from a local partner organization, researchers attempted to contact all 86 consenting beneficiaries or parents/caregivers. The preferred method of contact was through a home visit, and if a current physical address was unavailable then contact via telephone was attempted a maximum of twice. Fifty-seven (66.3%) of the 86 were located and gave additional written and verbal informed consent to participate in the study. We were unsuccessful in contacting the remaining 29 beneficiaries due to logistical and geographical limitations. Two beneficiaries were deceased at the time of the study.
The surveys were administered by means of face-to-face (n = 45) or telephone (n = 12) interviews with participants in or near Cap Haitien. If the wheelchair user was under the age of 12 years or was non-verbal, the interview was conducted with a primary caregiver. The national languages in Haiti are French and Creole, so a trained translator was present during the informed consent process and the interviews. The translator who assisted TCHH with the original seating programme was again hired to assist in conducting the follow-up interviews. For consistency and to minimize potential bias, a single member of the research team, who was unaffiliated with the seating programme and wheelchair delivery 6 months previously, conducted each of the 57 interviews. In order to accommodate the low literacy rate, the consent form and survey questions were read aloud to participants by the researcher and then translated by the translator. Responses were translated back to the researcher, and transcribed electronically onto a password-protected tablet. All beneficiaries were assigned a study ID prior to the interviews; thus all data entered was de-identified.
Descriptive statistics, including frequencies and percentages for categorical data and means with standard deviations for continuous data, were used to summarize participant demographics (sex, age, diagnosis, and place of residence) and characteristics about wheelchair use, wheelchair fit, wheelchair maintenance, environmental access, and perceived benefits of use were obtained from responses to multiple choice questions.
Given that the study participants had the opportunity to comment on benefits other than those that were listed among multiple choices on the questionnaire, a thematic analysis (21) was conducted to identify, analyse and describe common patterns in the qualitative data. Transcripts of participant comments were gathered into a data-set and read multiple times by a member of the research team in order to be adequately familiar with the data. Data extracts relevant to the research question of perceived benefits were identified and systematically colour-coded into meaningful groups. These codes were then grouped into potential themes, and reviewed and re-grouped over several days to refine the themes. This process was subjective to researcher judgement.
The 57 beneficiaries involved in the study ranged in age from < 2 to 31 years, with a mean age of 7.56 (standard deviation; SD 5.50) years. Their characteristics are summarized in Table I.
Table I. Characteristics of wheelchair beneficiaries (n = 57)
All respondents were still in possession of the wheelchair (n = 57). Just under half of the 57 participants (49.1%) were using the wheelchair at least once per day. Other participants indicated that they used it 3–5 times per week (21.1%), less than 3 days per week (17.5%), or that they never used it (12.3%). Responses regarding why the wheelchair was not being used are summarized in Table II.
Table II. Contributors to limited wheelchair use (n = 57)a
The most common location where participants used their wheelchair was at home, including indoors (n = 43) and outdoors (n = 32). Other common locations of wheelchair use included church (n = 22), out in the community (n = 25), and at the respite care centre (n = 13). Only 1 user used it at school, whereas 1 adult reported using it at work. The majority of users needed another person to propel the wheelchair (70.2%), while others could propel it with some assistance (12.3%), and some were able to propel it fully independently (12.3%).
Regarding questions about wheelchair maintenance, 21 of the 57 participants indicated that their wheelchair had broken at some time and 9 indicated that there were parts missing from their wheelchair. Parts of the wheelchair that were most frequently reported to be in need of repair were tyres/wheels (including flat tyres) (n = 9) and brakes (n =7). Fewer participants (n =6) indicated that the tilt mechanism, headrest/armrest/footrest, or trunk support needed repair. Regarding repair of the wheelchair, only 8 (14.0%) of the 57 participants indicated that repair was available in their area of residence. In addition, 47.4% of participants indicated that they were unsure of whether repair would be affordable.
Over half of the wheelchair users (63.2%) indicated that the wheelchair fit had not changed since it was set up at the seating clinic 6 months previously. One-third, 33.3% (n = 19), of users indicated that the wheelchair fit had changed, with the most common reasons being broken parts, or because the user had grown.
Regarding questions about wheelchair accessibility of the user’s environment, 54.4% (n = 31) of participants reported that roads and other daily paths were accessible to the wheelchair, while another 36.8% (n = 21) did not find them accessible. The large majority of users who found the roads inaccessible explained that it was due to the terrain being rocky, unpaved and too rough to propel the wheelchair on easily. See Table III for a selection of direct quotations describing the terrain.
Table III. Explanations provided by participants for roads being reported as inaccessible to the wheelchair
The question of whether there were physical barriers to accessing school did not apply to 89.5% of participants, due to those users not attending school or not bringing the wheelchair to school. When a similar question about accessibility of the home was asked, 38.6% (n = 22) of participants indicated that there were barriers to accessing the home with the wheelchair, and 50.9% (n = 29) reported none. The most commonly reported barrier to the home was steps at the entrance. Many families were able to overcome this barrier by carrying the wheelchair and user up over the steps and into the home. A few homes had a ramp at the entrance to facilitate wheelchair entry.
The majority of participants (86.0%) were able to transport the wheelchair from one place to another. As for specific methods of transport, participants used a “tap tap” (n = 15) (a small bus or pick-up truck that serves as a shared taxi), motorcycle taxi (n = 15), taxi (n = 1) or private vehicle (n = 11), and some (n = 19) reported walking whilst pushing the wheelchair.
The most commonly reported benefits of using the donated wheelchair were improved mobility, increased participation, and greater interaction with others. Other responses are summarized in Table IV.
Table IV. Benefits of using the donated wheelchaira
Thematic analysis suggested 3 main themes emerging from the open-response comments of participants on wheelchair benefits: gratitude, comfort and joy of the child, and relief of the caregivers.
Many caregivers expressed strong gratitude for the wheelchair, describing it as a “blessing” and a “treasure”. An adult wheelchair user reported he “thanks God for TCHH” because the wheelchair allowed him to work again. One caregiver “prays TCHH’s work continues to prosper”. Caregivers explained that before receiving the wheelchair they “desperately needed” one, or that their new wheelchair “is much better” or “more comfortable” than their old one. They acknowledged incomplete satisfaction with the wheelchair after 6 months of use due to certain barriers (i.e. the wheelchair being broken, difficult to transport, uncomfortable), but they maintained that they were happy to have it. A benefit underlying the sense of gratitude reported is that beneficiaries and their families did not sell or discard the wheelchair; they were grateful for the improved quality of life it provided.
Caregivers noticed their child appearing more comfortable, happy and relaxed in the wheelchair. It was relayed that their children were better equipped to eat independently and safely, to be more active, to “get fresh air”, to watch films that they loved, or to sit up and view their surroundings. The wheelchair was described as being “like a friend” to the child, and the “only chair [the child] wants to sit in”.
Caregivers emphasized the positive impact that the wheelchair had on themselves, in addition to their children. Before having a wheelchair, caregivers carried their children in their arms while doing work around the home, or on their back when going anywhere outside the home. They explain that having the wheelchair relieved back pain and facilitated performing other duties.
A key finding of our study was that 6 months after the specialized seating programme, every family that responded to the survey still had the donated wheelchair, and the large majority of children were using their wheelchair consistently with predominantly beneficial outcomes. Caregivers reported the main benefits of the wheelchair to be improved mobility and home accessibility, increased independence, and increased participation and interaction with others. Children were happier and more comfortable when now having a wheelchair, and the acquisition of the wheelchair resulted in reduced physical strain on carers. The study also identified a number of barriers to using wheelchairs in this setting, which decreased overall satisfaction with the wheelchair. A lack of expertise to repair, adjust or modify the equipment contributed significantly to non-use. An additional principal barrier was the physical environment. Typical transportation modes in Haiti are not generally conducive to wheelchair portage, and road conditions or lack of roads in rural areas create difficulties for manoeuvring wheelchairs. Standard wheelchair tyres are often not suitable for such rough and fluctuating terrain.
Our results are in line with other studies that provide direct evidence of wheelchairs improving the lives of people with disabilities (2, 3, 22–25).
Glumac et al. interviewed caregivers in Guatemala regarding their experiences with donated wheelchairs for children with disabilities (24). They determined that the wheelchairs were greatly valued by caregivers, and they provided physical and emotional relief to caregivers. The wheelchairs also had a positive impact on children’s participation in family and community activities. Barriers faced by wheelchair users in Guatemala were similar to those reported in Haiti, such as poor road conditions and inaccessibility of public buildings and home entrances. Also consistent with our study, inappropriate tyres were noted as a wheelchair characteristic that affected their use.
Shore & Juillerat described a survey of wheelchair users in India, Chile and Vietnam 12 months after receipt of a wheelchair and found that recipients reported benefits similar to those in our study, such as improved mood and quality of life, less illness and pain, and increased mobility (25). Another survey of 188 wheelchair recipients in India and Peru found that 93.0% of recipients used their wheelchair every day, and significant improvements in function and skin health were noted (3). In this survey 56.2% of recipients stated that the wheelchair had improved their quality of life. As in the current study, this study reported the most common maintenance problems to be related to the wheels, including flat tyres. A Canadian study showed increased self-care ability, play and activity levels in children with cerebral palsy using adaptive seating devices at home (23).
There is some literature that provides a stark contrast to our results regarding utilization and benefit of wheelchair use. A survey of 162 recipients of donated wheelchairs in India revealed that 71.6% of users abandoned or sold the wheelchairs, with the most common reasons for rejection being pain, fatigue, discomfort, environment incompatibility, and damage (12). The donated wheelchairs were described as being randomly distributed by a variety of NGOs, cheaply made, and of conventional size and configuration. The authors concluded that manual wheelchairs are unsuitable for outdoor ambulation, and of minimal use indoors. In contrast, in our study, 70.2% of participants were using the wheelchair a minimum of 3 times per week, and the majority reported using their wheelchair most often indoors and outdoors at home. We would theorize that 2 particular characteristics of the TCHH seating programme may have contributed to the observed increase in wheelchair usage. Each wheelchair provided by TCHH was customized to the user through clinical assessment by a team of seating experts, and participation and input of local providers was sought early in the process, which included some formal training in basic wheelchair maintenance.
Geographical and logistical factors played a role in data collection. Addresses were lacking for many beneficiaries of the seating programme and numerous telephone numbers were out of service. Most participants lived in rural areas, which lengthened the researchers travel time from house to house, and the majority of homes required the assistance of local partners’ to locate. Language was also a limiting factor, as accurate data transcription relied on precision of translation.
Implications and recommendations
The 2008 WHO Guidelines on the Provision of Manual Wheelchairs in Less-Resourced Countries emphasizes that good practice in wheelchair provision should include assistance in proper wheelchair fitting, training in wheelchair use and maintenance, and follow-up as key steps (6).
The WHO recommends follow-up within 6 months of donating a wheelchair, and it should determine the effectiveness of the wheelchair for the user, problems experienced, and the condition of the wheelchair (6). Appropriate follow-up has many potential benefits, including identification of un-met needs, improvement of future services, increased trust and strengthened partnerships. Follow-up has also been associated with fewer accidents caused by broken or malfunctioning wheelchairs (26).
To our knowledge, this is the first follow-up research on a wheelchair donation programme in Haiti, and it demonstrates that it is feasible and valuable to conduct follow-up studies as part of clinical initiatives in low-resource settings. TCHH will continue to use the survey that was developed for the study as a clinical assessment tool and an instrument to collect follow-up data for future seating programmes.
While not directly implicated in our survey results, it was clear throughout the data collection process that collaboration with local partners can greatly facilitate follow-up, from providing direct logistical assistance to strengthening ties between community members and the organization providing the wheelchairs. We recommend more follow-up studies of wheelchair donation programmes in developing countries, and engaging with local rehabilitation organizations and community stakeholders as much as possible in future follow-up studies.
As this was the first TCHH seating programme to include formal training in wheelchair use and repair, identifying commonly problematic wheelchair parts and barriers to repair was a key goal of the follow-up. The most frequently reported maintenance issues included flat or balding tyres, missing screws and bolts, and broken hand-brakes, all of which would be simple repairs if more services were available locally. As a direct result of this finding, TCHH changed their practice to include additional training the following year.
Therefore, based on our experience and the support of the WHO Guidelines, we would recommend skills training programmes for wheelchair users and caregivers be supported and evaluated in future donation initiatives. The WHO Guidelines provide numerous strategies for the development of training programmes, including the fundamental concept of building the capacity of certain local trainees to become trainers themselves (6). An example of how a strong trainee can benefit an entire community can be found in Box I.
Box I. Papito’s story: a personal anecdote emphasizing the importance of further developing and supporting formal training sessions in wheelchair repair for local community members
The current study also highlights the importance of considering the context and community environment in which the wheelchairs are being provided. Due to the physical environment in Haiti being more challenging for wheelchair users than in most developed countries, durability and stability of wheelchairs should be key considerations in donation efforts in Haiti, similar to other developing countries. Particular attention should be given to tyres that are durable and suitable for rough and unpredictable terrain. There are examples in the literature of effective efforts to create sustainable wheelchairs for developing countries and rugged terrain, with designs that specifically target environmental accessibility (27–29). It has also been shown that wheelchair skills training provided to users and caregivers can improve mobility and increase accessibility of difficult-to-manoeuvre terrain (30, 31). In order to maximize mobility benefits, wheelchair donation programmes should tailor the wheelchair to the specific needs of the recipient population. The information gathered from the survey guided the TCHH seating team to investigate the availability of more durable wheelchairs, rather than continuing to ship only North American wheelchairs to Haiti, which has resulted in a new partnership with a foundation that only donates wheelchairs meant for rugged terrain (Walkabout Foundation, https://walkaboutfoundation.org/).
This study emphasizes that responsible follow-up is a key component to success of wheelchair donation, and provides evidence that appropriate wheelchairs can make a positive difference to the lives of people living with disabilities in Haiti.
The authors would like to thank the wheelchair beneficiaries and their families, Fiona Stephenson, Joseph Janvier, the TCHH Seating Team, Haiti Hospital Appeal and the Maison de Benediction, Footprints of the Son, Children of the Promise, BSEIPH, Healing Hands for Haiti and the Walkabout Foundation for all of their collaboration and assistance. The authors also thank TCHH and the Faculty of Medicine at Dalhousie University for funding this research.


 Click to show fullsize
Click to show fullsize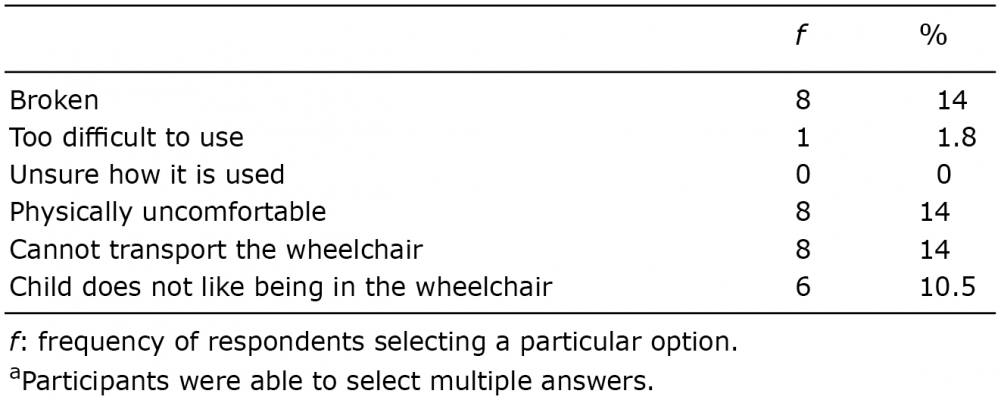 Click to show fullsize
Click to show fullsize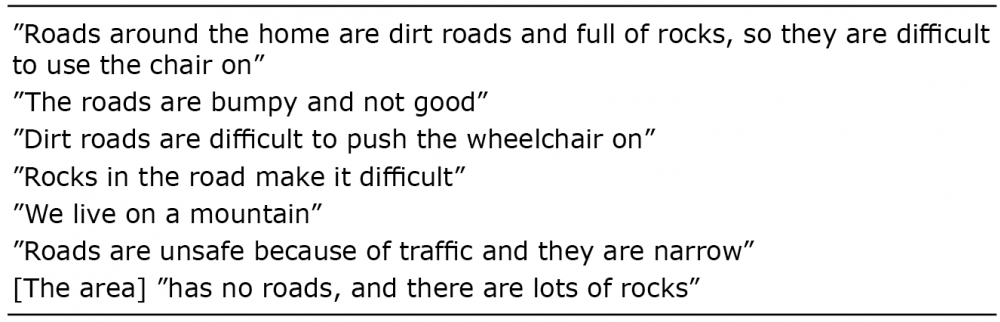 Click to show fullsize
Click to show fullsize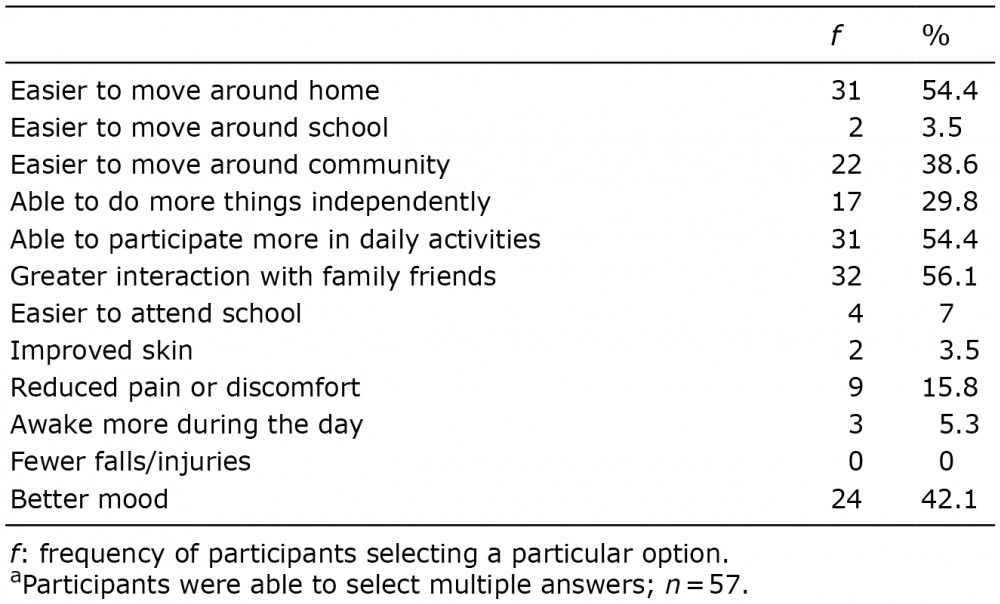 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize