
From the 1Salisbury NHS Foundation Trust, 2Faculty of Science and Technology, Computing, Bournemouth University, Poole and Odstock Medical Ltd, Salisbury, Wiltshire, UK
*Some of the data from this study was presented at the UK Stroke Conference on 2–4 December 2014, in Harrogate, UK.
Objective: To examine the evidence for a training effect on the lower limb of functional electrical stimulation.
Design: Cohort study.
Patients: A total of 133 patients >6 months post-stroke.
Methods: Training and orthotic effects were determined from walking speed over 10 m, associated minimal and substantial clinically important differences (i.e. >0.05 and >0.10 m/s), and Functional Ambulation Category (FAC), ranging from household walking to independent walking in the community.
Results: An overall significant (p < 0.01) training effect was found that was not a clinically important difference (0.02 m/s); however, “community” FAC (≥ 0.8 m/s) and “most limited community walkers” FAC (0.4–0.58 m/s), but not “household walkers” (< 0.4 m/s), benefitted from a clinically important difference. A highly significant (p< 0.001), substantial clinically important orthotic effect (0.10 m/s) was found. In terms of overall improvement of one or more FACs, 23% achieved this due to a training effect, compared with 43% due to an orthotic effect.
Conclusion: The findings suggest that functional electrical stimulation provides a training effect in those who are less impaired. Further work, which optimizes the use of the device for restoration of function, rather than as an orthotic device, will provide greater clarity on the effectiveness of functional electrical stimulation for eliciting a training effect.
Key words: electrical stimulation; peroneal nerve; stroke; long-term training effect; therapeutic effect; temporary carry-over effect; walking speed; foot drop.
Accepted Oct 7, 2016; Epub ahead of print Jan 18, 2017
J Rehabil Med 2017; 49: 113–119
Correspondence address: Tamsyn Street, Salisbury NHS Foundation Trust, SP2 8BJ Salisbury, UK. E-mail:tamsyn.street@nhs.net
Functional electrical stimulation (FES) of the peroneal nerve seeks to restore a normal walking pattern in those with drop foot, which is characterized by weakness or paralysis leading to an inability to activate the dorsiflexor muscles. An “orthotic effect” describes the immediate improvement in walking observed with FES compared with that without FES. A “training or therapeutic effect” describes a long-term improvement in walking without the FES after using FES for several weeks. In contrast, a “temporary carry-over effect” is experienced as an immediate, short-term improvement in function, following a brief period of using FES, which lasts up to 1 h (1–3). A close association has been found between peroneal nerve stimulation and an increase in excitatory synapses in the brain (2–4), suggesting that a carry-over effect may be associated with a long-term training effect. However, the identification of a long-term training effect is complicated by the potential presence of a temporary carry-over effect. Therefore, researchers attempting to measure a long-term training effect may be misled by the presence of a short-term carry-over effect, temporarily increasing the speed of walking.
A number of studies have found evidence for a training effect of FES, ranging between 0.06 and 0.18 m/s using the timed 10-m walking test (10MWT) (5–8). It is unclear from these studies how much of the observed improvement can be attributed to a stable long-term training effect, which would be present without FES, as there have been no studies of the impact of a temporary carry-over effect. Furthermore, the temporary carry-over effect may also mask any benefits due to the orthotic effect, as temporarily increasing unassisted walking speed would reduce the size of the difference compared with walking with FES. A masking of the true orthotic effect is of particular interest when interpreting previous research (6, 8–10) that has examined the differences between FES and other orthotic devices, as the measurement protocol may have led to an underestimation of the benefits of FES. One method to more reliably measure a long-term training effect is to maintain a set order of walking with the non-stimulated measurement being made first. A further issue with using the 10MWT as a measurement is that it includes 3 walks without and 3 walks with the assistance of FES, requiring a distance of 60 m to be covered. Studies that have measured FES use in this way (6, 7, 9, 10) are not representative of the FES user population who are unable to complete this distance.
A further limitation of some studies is to neglect the impact of the first 6 months post-stroke (6–8), which is when most spontaneous recovery is commonly reported to occur (11, 12). Therefore, any benefits observed could be due to the usual neuroplastic changes that occur after insult to the brain.
The current study examined the existence of a long-term training effect of FES in patients more than 6 months after stroke using an adapted 10MWT protocol to minimize any temporary carry-over effect.
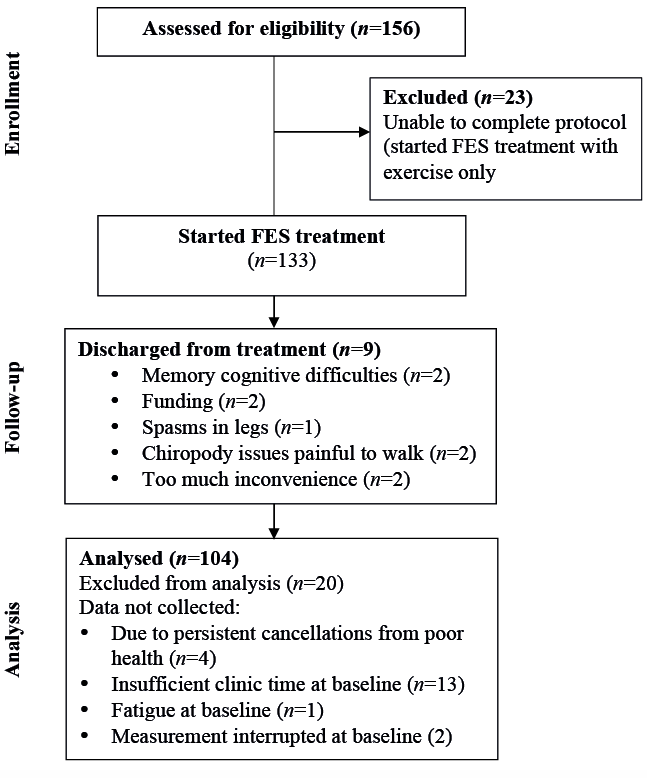
A total of 133 participants, > 6 months post-stroke (53 females, 80 males, mean age 59 years, age range 8–87 years, median time post-stroke 2.7 years, range 29 weeks to 34 years) with a drop foot, formed a referred sample for treatment (Fig. 1). A sample of convenience was used in the study, with participants being referred on an outpatient basis to the FES clinic by either general practitioners or hospital consultants. The majority were funded by the UK’s National Health Service (NHS). All patients seen between 2008 and 2015 who met the study inclusion criteria were included in the study. Analysis was conducted using routine audit data collected at each appointment; therefore ethical approval was not required. The study conforms to the principles of the Declaration of Helsinki.
Fig. 1. Flow of patients through the study. FES: functional electrical stimulation.
Seventeen participants had previously used and rejected an ankle-foot orthosis (AFO). The main reason for rejection was due to the AFO not helping with walking. Twenty-seven participants were currently using an AFO at the start of treatment.
Exclusion criteria were: patients less than 6 months post-stroke at the start of treatment; inability to walk 10 m even with the assistance of a walking aid; poorly controlled epilepsy; fixed skeletal deformities; recent injury; fracture; surgery; major skin conditions; proximity of cancerous tissue to the site of stimulation. Subjects with a cardiac pacemaker, implanted defibrillator or other active implanted device were investigated by a cardiac technician to ensure that there was no interaction with FES.
After an initial assessment to determine whether FES was a suitable treatment for use as a daily walking aid, patients were invited to return for 2 set-up appointments. At the first appointment they were instructed how to use the FES equipment. FES was applied using 2 electrodes placed over the common peroneal nerve either at the head of the fibula or popliteal fossa and over the motor point of the tibialis anterior. Stimulation was timed to the swing phase of gait using a foot switch under the heel, causing dorsiflexion with a small degree of eversion. Patients were instructed to gradually introduce the device into their everyday walking to become accustomed to the stimulation as an orthotic device. Patients were encouraged to use the device whenever they felt it would assist their walking. No further instructions were given as to the duration and frequency with which participants should use the device. Patients used the ODFS PACE (single channel) (Odstock Medical Ltd, Salisbury, UK). All devices stimulated at 40 Hz using either a symmetrical or asymmetrical biphasic waveform, with current intensity up to 100 mA and pulse width up to 360 ms. Stimulation, intensity, waveform, and timing parameters were adjusted to optimize the correction of drop foot for each individual.
All measurements were taken at baseline and again after a median of 20 weeks (interquartile range (IQR) 19–20 weeks). Timed 10MWT was measured using 3 different walks. The first walk was unassisted and used as a “warm-up”, the second measured unassisted walking, and the third was used as a measure of the effect of FES. A fourth walk measured unassisted walking following the use of FES immediately after the preceding walks, to determine whether there was a temporary carry-over effect from using FES.
Walking speed was measured in order to determine any long-term training effect, orthotic effect and temporary carry-over effect. An initial orthotic effect was defined as the difference between walking with no stimulation and walking with stimulation at baseline. A continuing orthotic effect measured the difference between no stimulation and stimulation at follow-up. A total orthotic effect measured the difference between no stimulation at baseline and stimulation at follow-up. A long-term training effect was measured as the difference between no stimulation at baseline and no stimulation at follow-up, to ascertain whether use of the device for 20 weeks had led to measurable improvements when it was switched off. A temporary carry-over effect was measured as a check, to ensure that the benefit observed from a long-term training effect, was not simply due to a temporary carry-over. It was not expected that temporary carry-over effect would be statistically significant. A temporary carry-over effect was calculated as the difference between unassisted walking after 20 weeks immediately prior to the FES walk and compared with the unassisted walk immediately after the FES walk.
Clinically important differences in 10MWT were defined as a substantial clinically important difference (≥ 0.10 m/s) or a minimal clinically important difference (≥ 0.05 to < 0.10 m/s) (13). FAC were also derived from unassisted walking speed, ranging from household walking to independent walking in the community (< 0.4 m/s = household walking only, 0.4–0.58 m/s = most limited community walking, 0.59–0.79 m/s = least limited community walking, ≥ 0.8 m/s = community walking) (14). Speed of walking without using FES measured on day 1 was used to define initial Functional Ambulation Category (FAC) of each participant prior to using FES. In addition, clinically important differences were used to examine the effect of FES on patients in the highest and lowest FAC. The measures were included to determine whether there was a difference in the clinically meaningful effects of FES on 10MWT in those in the lowest FAC compared with the highest FAC (14).
Clinical observations were recorded at baseline and follow-up. These included life events unrelated to FES, such as a back operation requiring bed rest, and adverse events related to the device, such as skin irritation. They also included technical issues that the patient encountered with the device itself, which required repair, as well as technical issues that the patient encountered while using the device, such as a difficulty in finding the optimum electrode position. Anything that had led to the patient not using the device regularly in the 20-week period of the study, such as a hospital stay for 2 weeks, a technical fault that required repair, and patient-reported frequency of FES use per week, was recorded as “infrequent use” of FES. Other clinical observations that may have had an impact on use of the device were recorded, such as cognitive issues, dysphasia, and whether the patient presented with complex mobility issues including spasticity and clonus.
Data from the step-counter of the device were recorded for the total number of steps, walks and walk duration. These measures were only included for 35 users, as the software has only recently been developed to allow these measures to be recorded reliably. A step was measured from the end of the rising ramp to the point of heel strike on the affected limb, in order to prevent small movements that are not steps being measured (Fig. 2). A walk count is taken from the number of times that the pause function on the device is unpaused and the walk duration is the total time spent unpaused. Therefore, people who do not pause the device while sitting down will have longer walk durations. The FES device measured steps, walks and walk duration continuously for the 20-week period; therefore the number of steps, walks and walk duration per day was not available. To provide an estimate of the total number of steps per day, the total number of steps for the 20-week period was divided by the individual time period each person used FES. The same procedure was used to estimate the number of walks and walk duration per day for each person.
Fig. 2. Stimulation envelope: a step is measured from the end of the rising ramp (the rising ramp starts at heel rise and is the adjustable gradual increase in the stimulation pulse width from zero to reach the set pulse width) to the point of heel strike.
Statistical analysis was performed using NCSS 9 statistical software (NCSS LLC, Utah, USA). Data were explored using histograms and box-plots and found not to be in a normal distribution. Planned comparisons were conducted using the Wilcoxon signed-rank test. A significance level of p < 0.05 was used. The Holm-Bonferroni Sequential correction was used to adjust for multiple comparisons. The planned comparisons included a long-term training effect, and initial, continuing and total orthotic effects, as described above.
A total of 124 patients (93%) still used FES 20 weeks after the start of the study, with 104 complete data-sets being available for analysis. The most common reason for patients to be excluded from the analysis was insufficient clinic time at baseline to undertake the outcome measures (n = 13). Insufficient clinic time describes a lack of time available following the set-up of the FES device, which may be due to the presentation of the patient being more complex. Nine participants were discharged from treatment due to memory or cognitive difficulties (n = 2), issues with funding (n = 2), chiropody issues making it painful to walk (n = 2), and finding FES to be too much inconvenience (n = 2). One participant discontinued treatment due to leg spasms; however, it is unclear whether the FES was linked to this occurrence. Nine patients experienced some degree of minor skin irritation from using the electrodes. This number was inconsistent with that found in individual clinical observations in each patient record (n = 16), therefore suggesting a lack of reporting. Thus, 12% of participants encountered some form of minor skin irritation, but in all cases clinical management enabled continued use of FES. Further clinical observations are provided below. The study included 2 participants with cardiac pacemakers, following the use of cardiac monitoring at the initial appointment, to ensure that there was no interaction with the FES device. The participants experienced no adverse events, providing the first study to report on the safe use of FES for people with pacemakers.
The main planned comparison of interest was training effect, which achieved a significant difference between unassisted walking speed on day 1 (0.50 m/s) compared with unassisted walking speed after using FES for 20 weeks (0.53 m/s) (Z=2.64, p = 0.008); however, this difference was not clinically meaningful (median difference 0.02 m/s, IQR 0.05–0.12) (Table I). A substantial clinically meaningful change (median difference 0.10 m/s, IQR 0.02–0.20) was found for total orthotic effect between day 1 unassisted walking speed (0.50 m/s) compared with walking with FES after 20 weeks (0.64 m/s) (Z=6.64, p = 0.001). An immediate initial orthotic benefit on day 1 and continuing orthotic effect after 20 weeks were also found to be significant (Table I).
Table I. Walking speed (m/s) for stroke patients with and without functional electrical stimulation (n=104)
A temporary carry-over effect was measured as a check to ascertain whether the observed long-term training effect was inflated by a temporary improvement in unassisted walking. No significant difference was found between the median speed for walking unassisted prior to stimulation of 0.64 (SD 0.31) m/s and walking without stimulation 0.64 (SD 0.30) m/s (p = 0.73). Therefore, this suggests that the long-term training effect had not been affected by a temporary carry-over effect.
Excluding the community FAC, which could not improve as it was the highest category, overall, 43% (32/75) of participants improved their speed by one FAC or more in terms of an orthotic effect and 23% (17/75) improved in terms of a training effect (Table II). Clinically important differences in training effect, according to FAC, were used to explore the data further (Table III). Community walkers in the least impaired category were found to benefit from a median clinically important difference in training effect (both 0.06 m/s). In contrast, household walkers, who were the most impaired walking category, appeared less likely to have a clinically important training effect (0.02 m/s).
Table II. Number of patients who improved or declined one Functional Ambulation Category or more for training and total orthotic effect
Table III. Frequency of patients according to Functional Ambulation Category who demonstrated a clinically important difference (> 0.05 m/s) in training effect
Overall, clinically important differences for each planned comparison revealed continuing orthotic effect to have the highest proportion of people 66 (64%) with a clinically important difference, whether it was substantial or minimal. Unassisted walking had the highest amount of decline, with 28 (27%) people having a clinically important decline whether substantial or minimal (Fig. 3).
Fig. 3. Clinically important differences for improvement and decline in walking speed due to training effect (n = 104). Training effect is the difference between unassisted walking at baseline and at 20 weeks follow-up. Initial orthotic effect is the difference between unassisted walking and functional electrical stimulation (FES) on day 1. Continuing orthotic effect is the difference between unassisted walking and walking with FES at follow-up. Total orthotic effect is the difference between unassisted walking on day 1 and FES walking at follow-up.
The clinical observations are shown in Table IV. The most frequent clinical observation was “patient technical” issues of using the stimulator, of which 47 issues were identified. These most frequently involved difficulty in positioning electrodes (n = 17), followed closely by poor electrode care (n = 15), i.e. allowing the electrodes to become dry and not changing them. The second most common clinical observation was “complex presentation” issues (n = 33), which included spasticity and clonus. Thirty-six percent (16/45) of participants with a clinically important improvement had 2 or more identified clinical observations, in contrast 82% (27/33) of those who had a clinically important decline had 2 or more identified clinical observations. Similarly, 82% (23/28) of those who did not achieve a clinically meaningful improvement or decline had 2 or more identified clinical observations.
Table IV. Life events unrelated and related to functional electrical stimulation use and adverse events that may have had an impact on the use of functional electrical stimulation categorised by clinically important differences in training effect
Step counter data recorded on the FES device was collected to measure quantitatively the frequency of using the FES device (n = 35). The median number of steps per day was 813 (IQR 108–1,244 steps) (Table V). The number of steps per day, walks and duration of walking per day was further examined for those who benefitted from a clinically meaningful training effect (n = 16) and those who experienced a clinically important decline (n = 8). The data revealed that those who achieved a clinically important training effect walked with stimulation for a longer duration of walking, walked more often, and took a greater number of steps (Table V).
Table V. Median and interquartile range (IQR) for total steps, walks and duration of walking (minutes) per day for those with a clinically important decline in unassisted walking speed (no training effect) (n = 8) and those with a clinically important improvement in walking speed (training effect) (n = 16)
Evidence was found for a significant training effect for FES of the lower limb; however, this was not clinically important (0.02 m/s). Further exploration revealed a clinically important training effect in the least impaired community ambulation category (0.06 m/s). In contrast, household walkers in the most impaired category did not gain a clinically important difference (0.02 m/s). Nevertheless, household walkers achieved an overall substantially clinically important orthotic effect (0.10 m/s). These findings suggest that the main benefit of FES is likely to be an orthotic effect; however, FES may be associated with a long-term training effect in those who are less impaired.
The more impaired group may have been less likely to acquire a training effect due to less residual cortical function. The new protocol for measuring the 10MWT also enabled a greater number of more impaired walkers to be included compared with previous work, potentially leading to an overall decrease in the size of the training effect. The results for less impaired walkers were consistent with the findings (0.06–0.08 m/s) of previous studies examining a training effect (5, 6, 8), suggesting that the reduced size of the training effect in the current study was influenced by the inclusion of a greater number of more impaired participants.
The finding of a highly significant, substantially clinically important orthotic effect (0.10 m/s) was consistent with a recent study using the same clinical model in multiple sclerosis (MS) (15). Stroke patients appear to exhibit both orthotic and training effects. In contrast, although people with MS are able to maintain their FAC for longer while using the device, the majority benefit only from an orthotic effect. This may be due to deterioration of the myelin and a reduced capacity for neuroplasticity. The findings suggest that FES may be useful as a rehabilitation tool following a stroke for those who are less impaired, while for more impaired stroke users and in those with a progressive diagnosis, it may be a means of maintaining functional mobility for longer.
Exploratory analysis of recorded clinical observations and preliminary steps counter data both suggest that increased frequency of using FES is associated with a long-term training effect. These initial observations are consistent with the literature on rehabilitation and exercise in stroke (16). Furthermore, the mean number of steps per day was towards the lower end of previous work (< 0.42 m/s) of 2,837 (SD 1,503) steps (17). Potentially, this may be due to many participants not using FES every day, as revealed by clinical observations, therefore as the number of steps per day was calculated using the total number of days that FES was available to each patient, the calculation may have been an underestimate. Furthermore, patients are encouraged only to use the device as an orthosis rather than for rehabilitation. Further research would benefit from studies designed to optimize the potential for a long-term training effect.
The alternative 10MWT protocol, which included a walk to measure unassisted walking compared with a walk for FES was a limitation to the study, as it opened up an increased likelihood of error. The 10MWT may not have been the most appropriate measure for more impaired users, as previous research on patients’ perceptions has found that a reduction in effort and falls were amongst the primary perceived gains from using FES (18). Furthermore, the measure did not capture gains made by those unable to walk without stimulation or comply with the alternative 10MWT protocol. A further limitation is that the study was not a randomized controlled trial; however, the sample was representative of the effectiveness of using FES in the community and a large group of FES users in the household walker category.
The alternative 10MWT protocol used here was less likely to incur a carry-over effect due to having the non-stimulated walk prior to using stimulation. However, similarly to previous studies, patients are likely to have walked to their follow-up appointment using FES, therefore potentially eliciting a temporary carry over effect despite the new protocol. Further work is therefore required to examine the presence, duration and size of any observed temporary carry-over effects.
FES for foot drop may be associated with a long-term training effect in less impaired stroke patients. Studies designed to optimize rehabilitation potential rather than an orthotic effect, would provide greater clarity on the effectiveness of FES for eliciting long-term changes in walking ability. A potential area for further research is the intensity of FES treatment through using step counters, which enable a daily record of use to be documented. A greater understanding of the temporary carry-over effect may provide greater insight into the mechanism behind any long-term training effects and may enable rehabilitation specialists to enhance the size of the long-term training effect.
The authors would like to acknowledge all past and present clinical staff at Salisbury District Hospital who provided treatment. The treatment was funded by the National Health Service (NHS). A grant was received from the Salisbury Healthcare Charitable Fund to fund the first author in completing the analysis. The second and third authors have affiliations or financial involvement with Odstock Medical Ltd, an organization or entity with a financial interest in the subject matter and materials discussed in the manuscript.


 Click to show fullsize
Click to show fullsize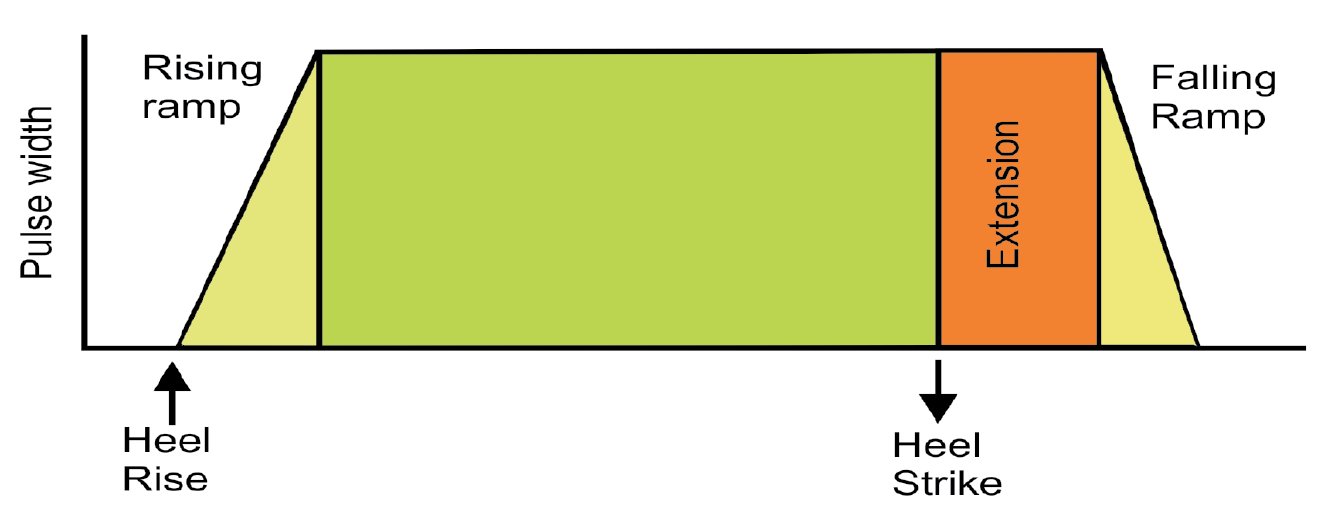 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize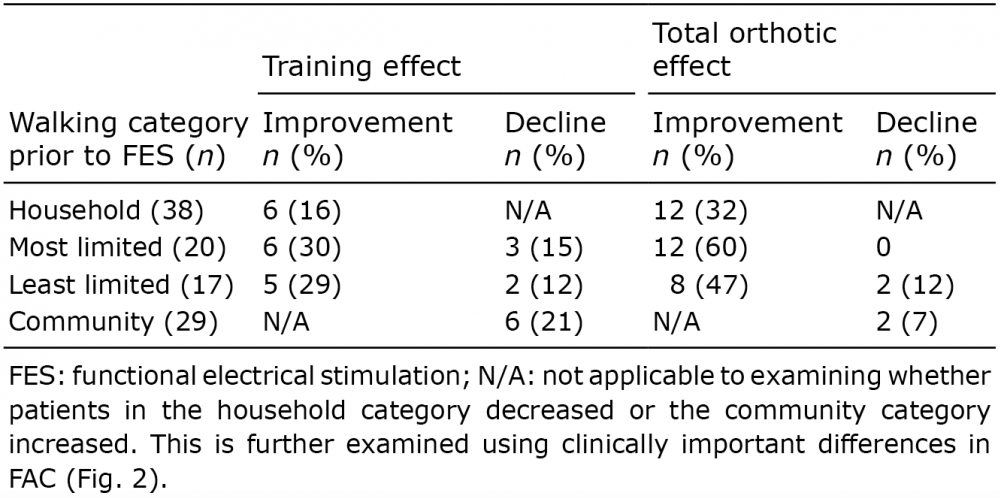 Click to show fullsize
Click to show fullsize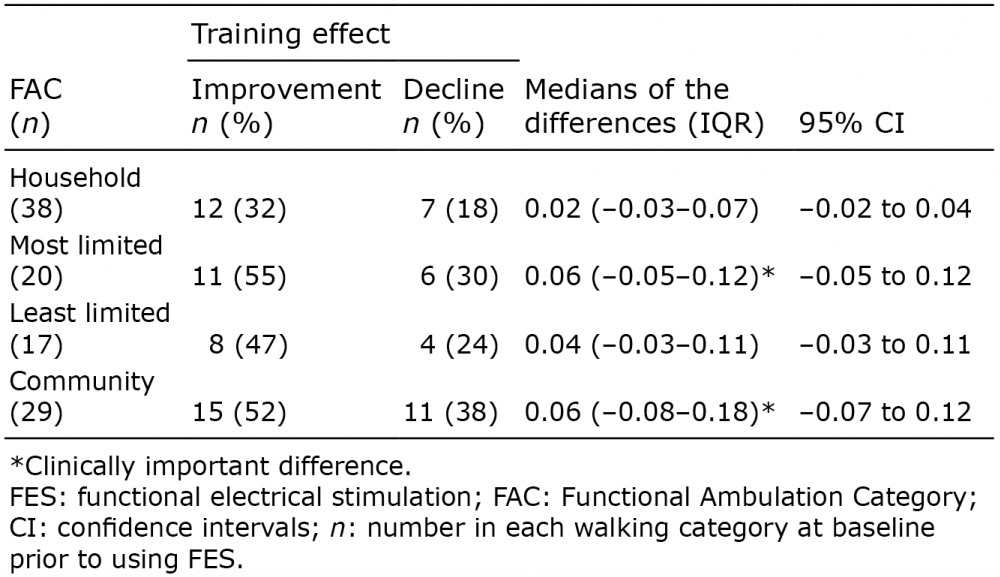 Click to show fullsize
Click to show fullsize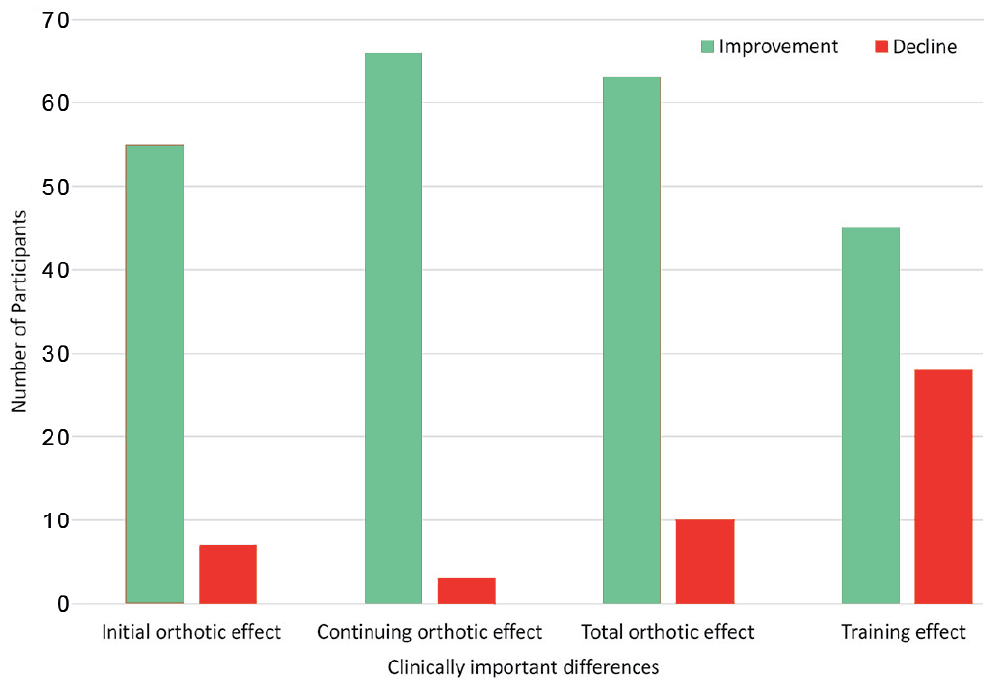 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize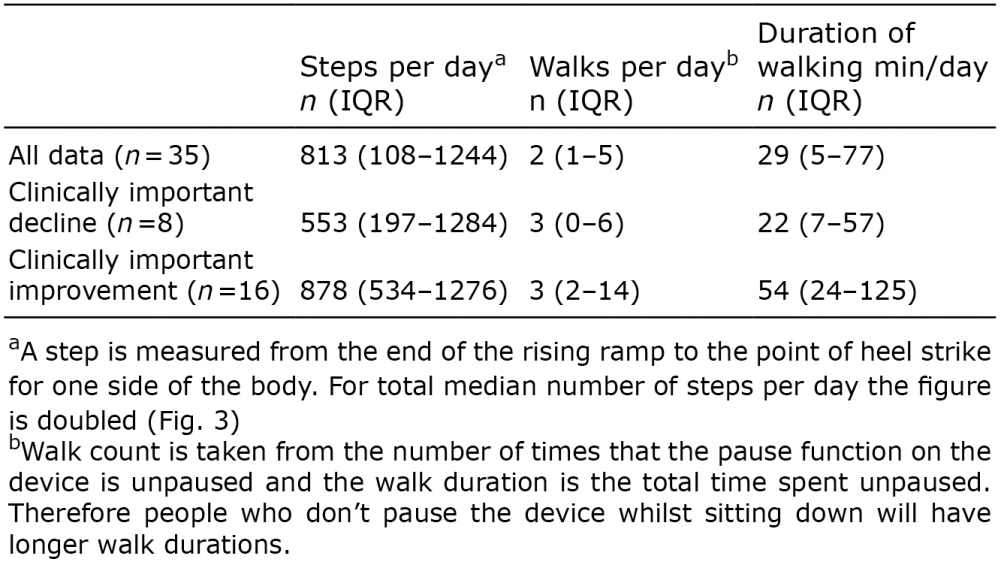 Click to show fullsize
Click to show fullsize