
From the 1Westmead Private Physiotherapy Services, Westmead Private Hospital Sydney and 2The Clinical Research Institute, Sydney, 3Department of Physiotherapy, Faculty of Medicine, Dentistry and Health Sciences, The University of Melbourne, Melbourne, Australia and 4University of Jamestown Physical Therapy Program, Fargo, ND, USA and 5School of Science and Technology, University of New England, Armidale, Australia
Objectives: To quantify physiotherapist-supervised and independent physical activity undertaken from the first to the fifth day after cardiac surgery (POD1 to POD5), and to relate the amount of physical activity undertaken with hospital stay and postoperative physiological functional capacity on POD6.
Methods: Physiotherapist-supervised and independent physical activity were monitored in 83 adult patients undergoing cardiac surgery, using a bi-axial accelerometer and skin sensors that measured, galvanic skin response and body temperature. Patients completed a 6-min walk test (6MWT) on POD6. Step count and physical activity intensity (METs; metbolic equivalents) were the main outcome measures.
Results: Males exhibited significantly higher physiotherapist-supervised and independent physical activity step counts and time ≥ 3 METS (p < 0.0001). The 6MWT distance on POD6 was greater in men (mean 393 m, standard deviation (SD) 108 m) than women (mean 300 m, SD 121 m) (p = 0.005). Mean length of stay in hospital was 9 days (SD 3 days) and was negatively correlated with overall physiotherapist-supervised (R = –0.70), independent physical activity step counts (R = –0.62), and combined physiotherapist-supervised (R = –0.65) and independent (R = –0.43) physical activity time ≥ 3 METs.
Conclusion: Physiotherapist-supervised activity fosters improvements in postoperative physiological functional capacity and reduces length of stay in hospital following cardiac surgery.
Key words: Early rehabilitation; cardiac surgery; physiotherapy; telemonitoring; physical activity.
Accepted Sep 13, 2016; Epub ahead of print Dec 8, 2016
J Rehabil Med 2017; 49: 71–77
Correspondence address: Sean Mungovan, Westmead Private Physiotherapy Services, The Clinical Research Institute, Suite 6, 16-18 Mons Road, Westmead, NSW 2145, Australia. E-mail: smungovan@crinstitute.com.au
Prescribed supervised exercise and independent physical activity programmes are important determinants of patient outcomes following cardiac surgery (1–6). Participation in postoperative independent physical activity and prescribed exercise programmes (phase I cardiac rehabilitation) reduces postoperative complications, e.g. venous thromboembolism and pulmonary complications (PPCs), (7) improves postoperative physiological functional capacity (PPFC) (2, 3), wound healing and autonomic tone (8). Early participation in prescribed postoperative exercise programmes is an integral component of rapid recovery protocols leading to optimal surgical outcomes (9–11).
Physiotherapists routinely assess and treat patients before and after cardiac surgery (12–14). During the first 5 days following cardiac surgery physiotherapy treatment has traditionally focused on respiratory techniques to minimize PPCs (15, 16). Due to a reduction in the incidence of PPCs after cardiac surgery and increasing evidence for the importance of appropriate exercise, there has been a shift in focus of physiotherapy management to the prescription of supervised exercise programmes, e.g. walking or stationary cycling (17). Appropriately prescribed exercise following cardiac surgery can improve PPFC at hospital discharge (2, 3), accelerate achievement of functional milestones (6) and reduce length of stay (LOS) in hospital (2). Research has shown, however, that males respond better than females to physical rehabilitation after cardiac surgery (18).
Guidelines for in-hospital rehabilitation after cardiac surgery suggest that a major role of prescribed supervised exercise is to facilitate a return to independent physical activity (1). However, the relationship between physiotherapist (PT)-supervised exercise and independent physical activity in the first 5 days after cardiac surgery has not been investigated previously. The current study was based on the hypotheses that PT-supervised exercise after cardiac surgery could result in an increase in the amount of independent physical activity, and that men would respond better than woman to physical activity after cardiac surgery.
The aims of the present study were therefore: (i) to determine the amount of PT-supervised and independent physical activity undertaken by men and woman from the first to the fifth postoperative day (POD1–POD5) following cardiac surgery; (ii) to examine the correlations between the amount of PT-supervised exercise and independent physical activity during POD1– POD5, PPFC at POD6, and LOS in hospital; and (iii) to examine which factors, including sex, that predict the amount of PT-supervised and independent physical activity during POD1–POD5.
The study was conducted at Westmead Private Hospital, Sydney, NSW, Australia. Ethical approval was obtained from the Western Sydney Local Health District Human Research Ethics Committee and written informed consent was obtained from patients prior to participation.
Consecutive patients awaiting cardiac surgery via a median sternotomy were identified and assessed for study eligibility. Exclusion criteria were: emergency surgery; non-English-speaking; age < 18 years; and musculoskeletal, neurological or peripheral vascular impairment precluding unaided mobility.
Patients undergoing cardiac surgery via median sternotomy at Westmead Private Hospital, follow a standard clinical care pathway, as described previously (3). Patients were assessed by the treating physiotherapist in the pre-admission clinic and on the day prior to cardiac surgery. Physiotherapy management was commenced on POD1 and included twice-daily sessions of PT-supervised: (i) respiratory techniques, (ii) active musculoskeletal movements for the prevention of musculoskeletal complications and to improve the range of motion of the upper limbs and trunk, and (iii) walking exercise of up to 10 min per session, as determined by the patient’s clinical status (3). Standard cardiac monitoring of patients via telemetry on POD1 was used in the intensive care unit (ICU). Discharge from the ICU typically occurred on POD2, after which independent physical activity was verbally encouraged, but not mandated or formally prescribed.
Height, body mass and vital capacity (VC) were measured on the day before cardiac surgery by the treating physiotherapist. VC was measured according to American Thoracic Society guidelines (19) and was measured to assess pre- vs post-operative change in lung function. Body mass index (BMI) (kg/m2) was calculated. Disease severity was classified according to the New York Heart Association (NYHA) functional classification (class I–IV).
Operation time, cardiopulmonary bypass (CPB) time, aortic cross-clamp time and postoperative ventilation time were obtained retrospectively from patients’ medical records.
equivalents) were measured using a SenseWear Pro 3 Armband (BodyMedia, Inc., Pittsburgh, PA, USA). The SenseWear Pro 3 Armband is a lightweight (< 100 g) battery-operated physical activity monitor that is secured with an elastic strap over the right triceps brachii muscle. The SenseWear monitor incorporates a bi-axial accelerometer and skin sensors that continuously measure heat flux, galvanic skin response, skin temperature and near-body ambient temperature. Data from the accelerometers and sensors are combined with anthropometric data to measure step count and physical activity intensity (METs) using established algorithms (20). The duration of exercise > 3 METS was measured, as this gives an indication that patients have retained or achieved physical independence post-surgery. Patients were fitted with the SenseWear Armband at 08.00 h on POD1 and were instructed to wear it continuously until 08.00 h on POD6. The armband has a “time-stamp” button, for the physiotherapist to mark the beginning and end of each individual treatment session. The time stamp allowed the identification of physical activity undertaken within the physiotherapy treatment period (PT-supervised exercise) and that undertaken outside of the physiotherapy treatment period (independent physical activity). The armbands were removed for showering, and for 5 min each day to enable the previous day’s physical activity data to be extracted using SenseWear Professional Software (version 6.1). Data were imported to a Microsoft Excel spreadsheet, combined sequentially, and separated into 24-h periods commencing at 08.00 h on POD1 and finishing at 08.00 h on POD6. Patient compliance with wearing the armband continuously was defined as the percentage of time it was worn over a 24-h period. The minimum compliance for analysis of the physical activity data was set at 90% of each POD (> 21.6 h).
A 6-min walk test (6MWT) was used to measure PPFC on POD6 (3). Patients were instructed to walk lengths of a 43.5-m corridor for 6 min, walking as far as possible while maintaining a rating of perceived exertion (RPE) of 3–4 on the Borg CR-10® Scale (21). 6MWT distance was measured to the nearest 0.5 m.
One-way analysis of variance and independent samples t-tests were used to compare PT-supervised vs independent physical activity and male:female participant groups with regard to demographic and anthropometric data. Repeated-measures analysis of variance was used to compare operation type and male:female participant groups with regard to postoperative physical activity levels (combined PT-supervised exercise and independent physical activity), and to investigate changes in physical activity levels (step count, time ≥ 3 METs) over the postoperative period POD1–POD5. The Pearson product-moment correlation coefficient was used to assess the presence and strength of correlations between PT-supervised exercise and independent physical activity, and combined PT-supervised and independent physical activity levels and PPFC (6MWT distance). Stepwise multiple regressions were conducted to predict daily and overall PT-supervised exercise and independent physical activity step count and time ≥ 3 METS for all patients with sex, age, BMI, VC, operation time and post-operative ventilation time used as co-variates. Spearman’s rank correlation coefficient was used to assess correlations between PT-supervised exercise and independent physical activity step count and time ≥ 3 METs and postoperative length of stay (LOS) in hospital. Data analysis was carried out with statistical package SPSS Statistics 17.0 for Mac. Two-tailed tests with a 5% significance level were used throughout. Sample size calculations indicated that 64 patients would provide sufficient power to detect correlations of R2 ≥ 0.7 between PPFC (6MWT distance) and measures of overall postoperative physical activity. To account for a potential 15% dropout rate approximately 74 patients were required to be recruited for the study.
A total of 106 patients presented for cardiac surgery via median sternotomy over the study period. Four patients meeting the study criteria declined to participate. Eight patients were excluded: 3 were non-English speaking; 2 were < 18 years of age; 2 due to emergency surgery; and 1 due to musculoskeletal impairment. One patient withdrew from the study after POD1, citing intolerance to the SenseWear Pro 3 Armband. Six patients required postoperative ventilation > 24 h and were therefore unable to follow the standard clinical care pathway and were excluded. Patients who underwent cardiac surgery via median sternotomy for management of congenital abnormalities were excluded from the group analysis because of insufficient numbers in this operation category (n = 4).
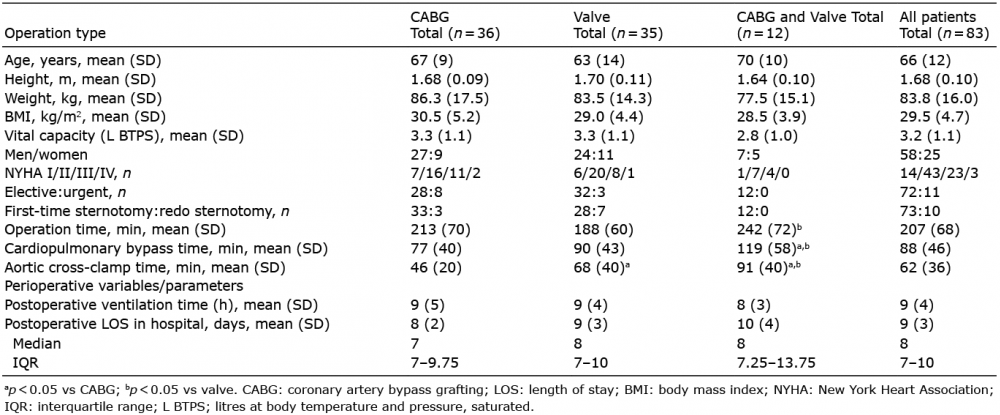
Anthropometric data, clinical characteristics and operation variables for 83 patients are presented in 3 groups according to operation type (Table I). There were significant differences in operation time, cardiopulmonary bypass time and aortic cross-clamp time among the 3 groups. The group who underwent combined coronary artery bypass grafting (CABG) and valve surgery had the longest operation time, cardiopulmonary bypass time and aortic cross-clamp time (p < 0.05) (Table I).
Table I. Anthropometric data, clinical characteristics and selected perioperative parameters for the 83 study patients
The step count of PT-supervised exercise completed by patients was similar to the step count of independent physical activity from POD2 to POD5 (Table II). There was a significant increase in the step count and physical activity time ≥ 3 METs from POD1 to POD5 for PT-supervised exercise, independent physical activity, and combined PT-supervised exercise and independent physical activity (p < 0.001) (Table II). Both PT-supervised exercise and independent physical activity were significantly correlated with overall step count from POD2 to POD5 (r = 0.72, p < 0.001) and time ≥ 3 METs from POD2 to POD5 (r = 0.58, p < 0.001).
Table II. SenseWear Armband compliance and physical activity data/results for the 83 included study patients
Woman were significantly older than men (mean age 72 (SD 11) vs 63 (SD 11) years, p = 0.002). Age was used as a covariate when investigating the effects of sex, time (POD) and supervision (PT-supervised exercise vs independent physical activity) on the duration of physical activity undertaken from POD1 to POD5.
There was a significant increase in both the PT-supervised and independent physical activity step counts at POD 5 compared with POD1 for males and females (p < 0.0001). There was a significant increase in both the PT-supervised and independent physical activity time METS ≥ 3 at POD5 compared with POD1 for males and females (p < 0.0001). Men exhibited significantly higher PT-supervised exercise and physical activity independent step counts and time ≥ 3 METS at POD5 compared with women.
There was a significant difference between males and females in the rate of increase in combined total step counts and time ≥ 3 METs from POD1 to POD5 (Table III) . From POD1 to POD5, men increased PT-supervised exercise step counts by 312 steps/day and independent physical activity step counts by 392 steps/day, PT-supervised exercise time ≥ 3 METs by 3 min/day and independent physical activity time ≥ 3 METs by 4 min/day. Over the same period women increased PT-supervised exercise step counts by 207 steps/day and independent physical activity step counts by 199 steps/day, PT-supervised exercise time ≥ 3 METs by 2 min/day and independent physical activity time ≥ 3 METs by 1 min/day. The type of surgery did not predict PT-supervised or independent physical activity step counts or time spent (PT-supervised or independently) exercising ≥ 3 MET
Table III. SenseWear Armband compliance and physical activity data for men and women
Men performed 53% (SD 18) of the total step count and 54% (SD 29) of the total time ≥ 3 METs within physiotherapy sessions.
Out of a total of 83 patients, 69 (53 men, 16 women) completed a postoperative 6MWT on POD6, the other 14 were either discharged prior to the assessment or underwent a secondary procedure and were thus unable to complete the postoperative 6MWT. There was a significant difference in the postoperative 6MWT distance between men (n =3) 393 m (SD 108) and women 300 m (SD 121) (p = 0.005). There were significant correlations (p < 0.001) between the 6MWT distance and the total step count (summed steps POD1-POD5) for i) PT-supervised (r = 0.76), ii) independent physical activity (r = 0.68), and iii) combined PT- supervised and independent physical activity (r = 0.80). There were significant correlations (p < 0.001) between the 6MWT distance and the total time ≥ 3 METs (r = 81, p < 0.0001).
There were significant moderate negative correlations (p < 0.001) between: (i) LOS in hospital and overall PT-supervised (R = –0.70) and independent physical activity step counts (R = –0.62); and (ii) LOS in hospital and overall PT-supervised (R = 0.65) and independent physical activity (R = – 0.43) time ≥ 3 METs.
VC (higher was better) and operation time (less was better) were predictors of daily and overall (summed POD1-POD5) PT-supervised and independent physical activity step counts. Together these 2 variables accounted for 34% of the variance in overall PT-supervised exercise step count. The regression equation was: (overall PT-supervised step count = 1,435+1,034 *VC (litres at body temperature and pressure, saturated (L BTPS)) –9.1*operation time (min)
Sex (being male was better) and age (younger age was better) were significantly related to independent physical activity time ≥ 3 METs, together accounting for 17% of the variance in overall independent physical activity time ≥ 3 METs. The regression equation can be represented as: (overall independent physical activity time ≥ 3 METs = 88.3–20.7* sex (male = 0, female = 1)–0.58*age (years)).
This study is the first to compare PT-supervised exercise and independent physical activity levels in patients during hospitalization after cardiac surgery. Physical activity levels increased progressively with postoperative time from POD1 to POD5. On average, patients performed more than half of their physical activity (step count and time ≥ 3 METs) from POD1 to POD5 within PT-supervised exercise sessions, despite these sessions accounting for approximately 3% of the total postoperative time spent in physical activity (approximately 3 h over 5 days). Thus, the more physical activity patients performed during physiotherapy treatment sessions, the more physical activity they performed independently.
There are limited published data on physical activity levels during hospitalization after cardiac surgery. In a trial investigating the effects of bedside television on physical activity after cardiac surgery, Papaspyros et al. (4) reported median step counts of 945 step/day (no television group) and 336 step/ day (television group) on POD5, considerably less than those observed in the present study. All patients in the present study had bedside television. Izawa et al. (22) reported an 8-day mean of 4,588 steps/day (SD 2,056) in patients during phase I (in-hospital) cardiac rehabilitation of 22 days (SD 4). It was not stated on which of the 22 days measurements were taken. In the present study it is possible that the Hawthorne Effect increased physical activity levels, as pedometer/accelerometer use/self-monitoring have been reported to increase levels of physical activity (22, 23). Alternative methods for recording 24-h physical activity levels, e.g. covert observation and cameras, were impractical (24). To minimize the Hawthorne Effect we provided no formal feedback to patients on physical activity levels until after POD6.
We anticipated a complex relationship between PT-supervised and independent physical activity levels; intuitively they might be correlated. Equally, patients “working harder” in PT-supervised exercise sessions (more steps and more time ≥ 3 METs) might prefer to “rest” than engage in additional independent physical activity outside the PT-supervised exercise periods. The significant and strong correlation between overall PT-supervised exercise and independent physical activity step counts suggests that supervised physical activity in cardiac surgery patients fosters more independent physical activity. Put simply, for each step taken within physiotherapy sessions, patients took one additional independent step. Further research is needed, focussing on this hypothesis.
It is difficult to make inferences from the observed sex differences in postoperative physical activity levels, given the significant male:female differences in age and VC. It has been reported that females undergoing cardiac surgery in Australia are older than their male counterparts (25); the impact of sex on short-term postoperative outcomes, independent of age, remains controversial. In the present study, age was a significant, albeit weak, predictor of independent step count among men. Women may therefore benefit most from phase I PT-supervised exercise; however, it is unclear whether this is due to their age or sex. Our data suggests that older females are likely to achieve more steps and, by inference, better 6MWT performance, if they receive PT-supervised exercise. VC was the sole significant predictor of independent physical activity levels for all patients, suggesting that patients with poorer preoperative lung function may require/benefit from increased duration of PT-supervised exercise and a period of preoperative inspiratory muscle training to optimize respiratory function prior to and following surgery (14).
For both men and women there were significant correlations between physical activity levels and: both (i) PPFC on POD6, and (ii) postoperative LOS. The strong relationship between PT-supervised physical activity levels (step count) and functional capacity (6MWT distance) is intuitive. In essence, PT-supervised walking exercise on POD4 and POD5 constituted bi-daily 10-min walk tests, and overall PT-supervised step counts were heavily weighted to POD4 and POD5. The significant and moderate relationship between independent physical activity levels and PPFC is perhaps more interesting, as this independent physical activity was not time-constrained, and therefore not cadence-dependent. While the PPFC benefits of PT-supervised exercise after cardiac surgery have been reported (2, 3, 6), our finding that patients may obtain increased benefit from additional, independent physical activity is intuitive, but not commonly reported. Significant correlations between physical activity levels across POD1 to POD5 and LOS are also of clinical relevance. Previous research has reported that higher frequency exercise therapy/physiotherapy after cardiac surgery hastens the achievement of functional milestones (6). A systematic review of “extra” physiotherapy found LOS benefits across a range of acute/sub-acute hospital presentations (26). That we found a significant, moderate correlation between independent physical activity levels and LOS, even excluding those patients who were unable to complete a 6MWT on POD6, suggests the stimulus provided by the PT-supervised exercise to increase independent physical activity may be as important as the physiotherapy itself. Ensuring the inclusion of PT-supervised exercise in clinical care pathways is indicated in order to maximize PPFC. Surgeons leading multidisciplinary surgical teams may also justify this inclusion through the benefits associated with a reduction in LOS in hospital. We do, however, acknowledge that patient age, complexity of surgical procedure, ventilation time and other factors may influence LOS.
The accuracy of the SenseWear Pro 3 Armband (version 6.1 software) in estimating energy expenditure has been tested against indirect calorimetry in healthy individuals. While accurate for most activities ≤ 3 METs, SenseWear may overestimate (by 4–9%) for walking activities, particularly those ≥4 METs (27). It is possible that the time spent undertaking physical activity ≥ 3 METs in the present study may be an overestimate, but not to the extent that the findings are altered for either distance or time spent > 3 METS. The accuracy of step count data in cardiac surgery patients, in whom arm-swing may be reduced, has not been established. While waist-worn pedometers can be accurate at slow walking speeds (28), we anticipated that 24-h compliance with such pedometers might be relatively poor, given that our patients typically wear (and regularly change) hospital gowns.
Treating physiotherapists were not blinded to physical activity data, which may have influenced the advice/encouragement they gave to patients regarding independent activity. Clinical experience suggests, however, that such advice/encouragement would be preferentially given to patients with “lower” supervised physical activity levels. Differences in independent physical activity levels between “high” and “low” physical activity individuals would thus only be mitigated, not exacerbated.
The limited number of female patients in the current study precluded sex-specific regression analysis of their independent physical activity levels. The male:female ratio in the present study is similar to that observed in the Australian cardiac surgery population (25).
In the early postoperative period after cardiac surgery PT-supervised physical activity accounts for approximately 50% of overall physical activity. PT-supervised physical activity foster improvements in PPFC and reduces LOS in hospital. Further research into the barriers to independent physical activity after cardiac surgery and interventions to promote independent physical activity in a larger cohort of males and females, is warranted.
The authors acknowledge support from Ramsay Health Care with the design and development of the study and data collection procedures, and from our medical, nursing and physiotherapy colleagues at Westmead Private Hospital. We also acknowledge the statistical advice received from Dr Roger Adams and technical assistance from Dr Zoe McKeough. This paper is dedicated to the memory of Paul Ramsay AO, founder of Ramsay Health Care.


 Click to show fullsize
Click to show fullsize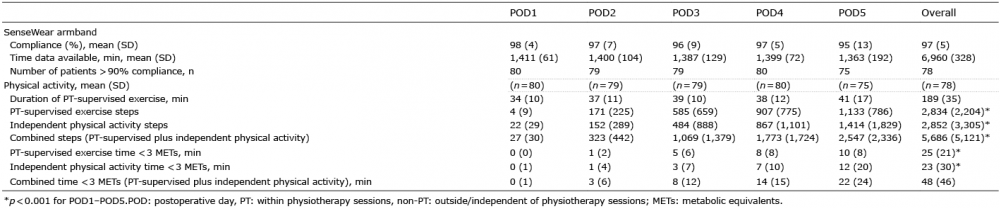 Click to show fullsize
Click to show fullsize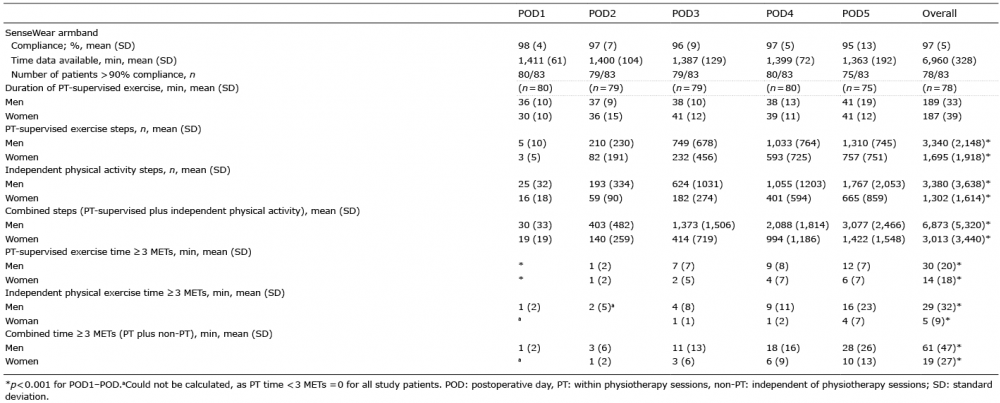 Click to show fullsize
Click to show fullsize