Ruth Wobma, MSc1, Rinske H. M. Nijland1, PhD, Johannes C. F. Ket2 and Gert Kwakkel, PhD1,3,4
From the 1Amsterdam Rehabilitation Research Center, Reade, 2Medical Library, VU University, 3Department of Rehabilitation Medicine, MOVE Research Institute, VU University Medical Center, and 4Department of Rehabilitation Medicine, Neuroscience Campus Amsterdam, VU University Medical Center, Amsterdam, The Netherlands
OBJECTIVE: To systematically review the literature on evidence for the application of peer support in the rehabilitation of persons with acquired brain injury.
DATA SOURCES: PubMed, Embase.com, Ebsco/Cinahl, Ebsco/PsycInfo and Wiley/Cochrane Library were searched from inception up to 19 June 2015.
STUDY SELECTION: Randomized controlled trials were included describing participants with acquired brain injury in a rehabilitation setting and peer supporters who were specifically assigned to this role.
DATA EXTRACTION: Two independent reviewers assessed methodological quality using the PEDro scale. Cohen’s kappa was calculated to assess agreement between the reviewers.
DATA SYNTHESIS: Two randomized controlled trials could be included, both focussing on patients with traumatic brain injury. The randomized controlled trials included a total of 126 participants with traumatic brain injury and 62 caregivers and suggest a positive influence of peer support for traumatic brain injury survivors and their caregivers in areas of social support, coping, behavioural control and physical quality of life.
CONCLUSION: The evidence for peer support is limited and restricted to traumatic brain injury. Randomized controlled trials on peer support for patients with other causes of acquired brain injury are lacking. It is important to gain more insight into the effects of peer support and the influence of patient and peer characteristics and the intervention protocol.
Key words: peer support; rehabilitation; brain injury.
J Rehabil Med 2016; 48: 837–840
Correspondence address: Ruth Wobma, Amsterdam Rehabilitation Research Centre, Reade, PO Box 58271, NL-1040 HG Amsterdam, The Netherlands. E-mail: r.wobma@reade.nl
Accepted Sep 15, 2016; Epub ahead of print Oct 26, 2016
INTRODUCTION
Everyday functioning, societal participation and quality of life can be greatly affected by acquired brain injury (ABI). For most patients changes are permanent and their expectations and future plans have to be adjusted drastically (1, 2). Rehabilitation programmes are designed to support this adjustment as they focus on interventions to: (i) restore impairments, (ii) regain the ability to perform activities of daily living, and (iii) find a new balance in areas such as relationships, work and daily and social life. Healthcare professionals are regularly brought together in a multidisciplinary team in order to meet the diversity of the health issues. However, there is an increasing incorporation of peer support into regular healthcare, as it has been recognized that healthcare professionals alone are often unable to satisfy patients’ needs (3). In literature, different definitions are given for “peer support”, suggesting that this concept may reflect different constructs. For the current review, peer support is defined as social emotional support, offered by persons with experiential knowledge and with characteristics similar to the recipient (3). Experiential knowledge is practical, related to the here-and-now and holistic. In comparison, knowledge provided by regular rehabilitation professionals is theoretical, future oriented and segmental (4). A similarity in characteristics refers to a similar demographic background, marital status, interest and having gone through a comparable stressful situation. It is assumed that the peer supporter is then more likely to be perceived as a positive role model (5, 6).
Nowadays, more rehabilitation settings are interested in the potential of peer support to improve their healthcare. However, descriptions of peer support programmes are heterogeneous and dependent on the type of care setting in which they are applied. Programmes differ from one-on-one visits to group conversations on the internet. Also, different choices are made with regard to the training of peer supporters, matches between the peer supporter and the recipient, frequency of contact and the phase of rehabilitation in which peer support is provided (1, 7, 8). Finally, research displays a variety of study designs and a variety of outcomes that can roughly be categorized into the domains of psychological health, physical health and outcomes that target behaviour (3).
The purpose of the present study was to systematically review the literature on the available evidence for the application of peer support in the rehabilitation process of persons with ABI and its influence on psychological, physical, behavioural well-being and quality of life.
METHODS
Definitions
In this review ABI is a collective term for acute (rapid onset) brain injury of any cause, including:
Peer support is defined as social emotional support, offered by persons with experiential knowledge and with characteristics similar to the recipient (3). In this review, the addition is made that peer supporters are specifically assigned and/or trained for their role.
Rehabilitation is defined as: “the use of all means to minimise the impact of disabling conditions and to assist disabled people to achieve their desired level of autonomy and participation in society” (9).
Study identification
A review protocol was developed based on the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) statement (www.prisma-statement.org). PubMed, Embase.com, Ebsco/Cinahl, Ebsco/PsycInfo and Wiley/Cochrane Library were searched from inception up to 19 June 2015 (by RW and JCFK). The following terms were used (including synonyms and closely related words) as index terms or free-text words: “peer group” and “brain injury” or “cerebrovascular disease” or “stroke” or “paralysis” or “hemiplegia” or “brain tumour” or “aphasia”. The full search strategies for all the databases are available from the corresponding author. Duplicate articles were excluded. All languages were accepted.
Articles were included if they met the following criteria:
Studies were excluded if they reported organized or unorganized contact with other acute survivors of ABI in the hospital or rehabilitation centre. These “peers” are fellow sufferers in the same phase after ABI. They do not have the amount of experiential knowledge (i.e. of the chronic phase after ABI) that a peer supporter has. Studies that described organized peer support, but were not specifically rehabilitation oriented, such as peer support for secondary stroke prevention, were also excluded.
Two authors (RW and RN) independently reviewed the titles of the identified references, selected the relevant studies on the basis of title and abstract and subsequently checked independently whether the selected studies satisfied the inclusion criteria. If a study did not provide conclusive information in the abstract, the full text was retrieved and reviewed. Disagreements were resolved by consensus, and a third review author (GK) was consulted when disagreements persisted.
Methodological quality
Two independent reviewers (RN and RW) assessed the methodological quality of each RCT by using the PEDro scale (11). PEDro is a valid and reliable scale, used for studies on rehabilitation (12), consisting of 11 items. Ten items assess the internal validity of a clinical trial, 1 item relates to the external validity. When the criterion of the items is satisfied, 1 point is given, with a maximum of 10 points (the first item is not included in the total score). The higher the score, the better the quality of the study. Before consensus was reached, a Cohen’s kappa was calculated to assess agreement between the 2 independent reviewers.
RESULTS
Study identification
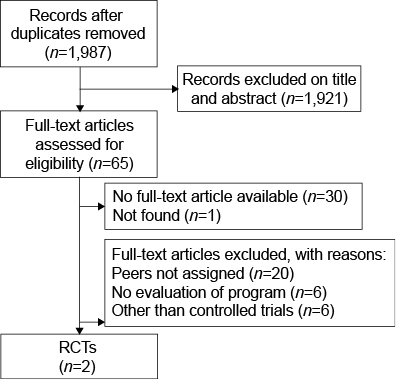
The search strategy revealed 1,987 studies. Fig. 1 shows the flowchart of identified studies that were considered for inclusion. The results of the electronic search strategy in different databases are available from the corresponding author. After selection based on title and abstract, 1,921 studies were excluded. Reasons for exclusion were that studies had been conducted in a different patient population or that the intervention was different from peer support as defined. Of the 65 articles that remained, 19 involved brain trauma, 29 vascular accidents, 1 encephalitis and 16 described a general ABI population, of which 4 articles specifically addressed patients with aphasia. One citation was not found and 30 were not available in full text. Most of these were poster presentations, for others several attempts were made to contact the authors, without success (n = 6). Of the remaining 34 full-text articles, 32 studies were excluded for several reasons, as shown in Fig. 1. Screening of references did not yield any further studies.
Fig.1. Identified studies. RCT: randomized controlled trial.
Identified studies
A total of 2 RCTs, reflecting 126 participants with traumatic brain injury (TBI) and 62 caregivers, met the criteria and were included in further analyses (8, 13). Before consensus was reached, a Cohen’s kappa of 0.8 was calculated to assess agreement between the 2 independent reviewers. Table I shows the PEDro scores of the 2 studies.
|
Table I. Characteristics of studies included in this review |
|||||||
|
Source |
Setting |
n (E/C) |
Age, years Range |
Inclusion criteria |
Intervention |
Main outcome measures |
Authors conclusions |
|
Hanks et al., 2012 (13) |
Rehabilitation unit |
96 persons with TBI (47/49) 62 caregivers (31/31) |
TBI 17–86 caregiver 21–76 |
Cleared from post-traumatic confusion, >16 years, received inpatient rehabilitation, Glasgow Coma Scale 13–15 |
Mentoring up to 2 years after discharge: weekly contact first month, biweekly next 2–3 months, monthly for remainder of first year |
Peer Mentoring Questionnaire; Brief Symptom Inventory–18; Family Assessment Device; Coping Inventory for Stressful Situations; Short Michigan Alcohol Screening Test; Medical Outcomes Study 12-Item Short-Form Health Survey; Community Integration Measure. |
Mentoring can be an effective way to benefit mood and healthy coping after TBI, and it can help to prevent maladaptive behaviours, such as substance abuse and behavioural dyscontrol, in the living situation. |
|
Struchen et al., 2011 (8) |
Community |
30 persons with TBI (12/18) |
21–68 |
Medically documented TBI, community dwelling, >18 years, no longer in rehabilitation programme |
Phone contacts and joint participation in social events: 3-month period |
Social Activity interview; Center for Epidemiological Studies Depression Scale; UCLA Loneliness Scale; Satisfaction with Life Scale; Interpersonal Support evaluation list; Weekly social activity data; Satisfaction survey |
Satisfaction ratings for Social Peer Mentoring programme were uniformly high and selected positive findings encourage further investigation of social mentoring as an intervention to effect improvements in social integration. Small sample size and reduced “dosage” of mentor interactions were limitations of this study. |
|
TBI: traumatic brain injury; E/C: Experimental group/Control group. |
|||||||
The main characteristics of the 2 studies are shown in Table II. Struchen et al. (8) describe a trial in which 12 community-dwelling survivors of TBI were matched with peer supporters with TBI and the outcomes were compared with 18 participants in a waiting list control group. They report significant improvement in perceived social support and a positive change with regard to social integration, social network size and participation in highly valued activities. Alongside the positive outcomes, the authors also report a significant increase in depressive symptoms in the supported group (8, 13). Hanks et al. (13) included participants immediately after discharge from a rehabilitation unit. In this randomized trial, the outcomes of a peer supported intervention group with 47 TBI survivors and 31 caregivers (family or friends) were compared with a control group of 49 TBI survivors and 31 caregivers. This study reports significant positive changes in behavioural control and less chaos in the home environment, less alcohol use, less emotion-focused and avoidance-oriented coping and a good physical quality of life compared with those who were not supported by a peer. At the same time, the peer-supported caregivers group showed less community integration and there was a tendency toward greater family dysfunction and anxiety compared with the control group.
|
Table II. Methodological quality of the included trials |
||||||||||||
|
Source |
Eligibility criteria specified |
Random allocation |
Concealed allocation |
Comparable at baseline |
Blind subjects |
Blind therapists |
Blind assessors |
Measures key outcome for >85% |
Intention to treat analysis |
Between group comparisons |
Point estimates and variability |
PEDro total score |
|
Hanks et al. (13) |
Yes |
1 |
0 |
1 |
0 |
0 |
0 |
0 |
1 |
1 |
1 |
5 |
|
Struchen et al. (8) |
Yes |
1 |
0 |
1 |
0 |
0 |
0 |
0 |
1 |
1 |
1 |
5 |
DISCUSSION
The aim of this study was to systematically review the literature on the available evidence for the application of peer support in the rehabilitation of persons with ABI. Although peer support has already been part of healthcare since the early 1990s (4), evidence is limited, resulting in only 2 proof-of-concept trials that could be included, both focussing on patients with TBI. The RCTs included a total of 126 participants with TBI and 62 caregivers, and suggest a positive influence of peer support for TBI survivors and their caregivers in areas of social support, coping, behavioural control and physical quality of life. RCTs on peer support for patients with other causes of ABI are lacking. However, 5 out of 6 excluded studies (see Fig. 1) did evaluate peer support programmes for stroke survivors (1, 4), caregivers of stroke survivors (4, 14), people with aphasia (15) and young adults after ABI (2). These studies did not use a control group, but their evaluations are positive about the use of peer support for patients with other forms of ABI. High-quality RCTs should be conducted to confirm these favorable findings.
Although support by a trained peer was generally found to be effective, both RCTs also report negative effects. Patients supported by a peer in Struchen’s study show an increase in depressive symptoms (8). In the other RCT negative effects were reported in the peer supported caregivers’ group. This group perceived less social support and community integration compared with the control group. Furthermore, there was a tendency towards more anxiety and family dysfunction (13). In both studies, the authors hypothesize that this might be due to an increased awareness of problems after TBI. In order to explore whether, in time, the control group would become as aware of these problems as the patients supported by a peer, future research should include a longer follow-up period. Furthermore, it is necessary to get a better understanding of what lies behind the unfavourable outcomes, in order to eliminate these as much as possible. Peer support could, for instance, be offered in a too-early stage of rehabilitation (1), selection of peers could be of influence (3), and one could argue that too little is known about the “perfect” match between the recipient and peer supporter.
The intervention protocols in the studies of peer support show a great heterogeneity. With regard to the means by which peer support is offered, phone contacts appear to be an efficient means of communication between the peer supporter and the patient or caregivers in both RCTs. However, other media, such as face-to-face visits (1), group conversations (15) or contact via the internet (16), were also considered. From the 2 RCTs, Hanks et al. (13) reported a higher dosage of peer support and a longer length of contact than Struchen et al. (8), but both showed improvement in comparison with the control group. Unfortunately, comparing the results of these studies and subsequently pooling of their findings is not possible since they used different outcome measures. Optimal dosage, length of peer support and means of communication should therefore be investigated further. The timing of initiation of peer support after TBI also differed between the 2 RCTs. In Hanks’ study peer support was provided immediately after discharge from the rehabilitation unit, whereas the participants in Struchen’s study were community dwelling and no longer participant in any rehabilitation programme. The fact that both RCTs show a positive effect of peer support suggests that peer support is broadly deployable; however, the phase of rehabilitation in which peer support is most effective remains unknown.
A limitation of the current review is that the results of the RCTs could not be compared or pooled, since different outcome measures were used. Consensus should be reached on how to measure the effect of peer support on the domains that it might affect, such as social support, coping, behavioural control and (physical) quality of life. Overall, it seems to be important to first gain more insight into the characteristics of the patients (e.g. time after injury) and the intervention protocol (e.g. number of contacts) before a well-founded RCT can be conducted. The broad possibilities that peer support encompasses do not make it easy to investigate, although the influence on patients with ABI in rehabilitation seems promising. Currently, a prospective cohort study is in progress in the rehabilitation centre, Reade in Amsterdam, the Netherlands, in which patients who receive peer support are followed during inpatient rehabilitation (Dutch Trial register number 4315). At discharge, patients are asked if they perceived their contact with the peer supporter as meaningful. Determinants that might influence a positive outcome of peer support are being investigated.
ACKNOWLEDGEMENT
This study was funded by an award from the Duyvensz-Nagel Foundation.
REFERENCES

