Lotte Nygaard Andersen, PhD1,2, Birgit Juul-Kristensen, PhD2,3, Thomas Lund Sørensen, MD4, Lene Gram Herborg, OT5, Kirsten Kaya Roessler, PhD1 and Karen Søgaard, PhD2
From the 1Department of Psychology, and 2Department of Sports Science and Clinical Biomechanics, University of Southern Denmark, Odense, Denmark, 3Institute of Occupational Therapy, Physiotherapy and Radiography, Bergen University College, Bergen, Norway, 4Medical Department, Hospital of Southern Jutland, Region of Southern Denmark and 5Senior Citizen and Health Department, Municipality of Sønderborg, Sønderborg, Denmark
OBJECTIVE: To evaluate the longer term efficacy of the interventions Tailored Physical Activity (TPA) and Chronic Pain Self-management Program (CPSMP) against a reference group on return-to-work for sick-listed subjects with pain in the back or upper body.
DESIGN: A randomized controlled trial.
SUBJECTS: A total of 141 sick-listed subjects with pain in the back or upper body.
METHODS: All participants received health guidance for 1.5 h and were randomly assigned to TPA (n = 47), CPSMP (n = 47) or a reference group (n = 47). The primary end-point was the proportion of participants returning to work and the co-primary end-point was the duration of the sickness absence period retrieved 11 months after the first day on sick leave. Secondary outcomes were pain level, body mass index, aerobic capacity, work ability and kinesiophobia.
RESULTS: TPA and CPSMP were no more effective than the reference group as regards return-to-work. Compared with the reference group no other benefits of TPA and CPSMP were evident regarding pain, work ability, kinesiophobia or physical capacity.
CONCLUSION: After 11 months TPA, the reference group, and CPSMP show similar patterns of facilitating return-to-work. This is additional knowledge, compared with the 3-month findings reported previously, showing that TPA seems to facilitate a faster return-to-work.
Key words: Chronic Pain; return to work; exercise therapy; patient education; rehabilitation; intervention study; musculoskeletal pain.
J Rehabil Med 2016; 48: 887–892
Correspondence address: Lotte Nygaard Andersen, Department of Psychology, University of Southern Denmark, Campusvej 55, DK-5230 Odense M, Denmark. E-mail: lonygaard@health.sdu.dk
Accepted Aug 29, 2016; Epub ahead of print Oct 26, 2016
INTRODUCTION
Musculoskeletal disorders often include complex and diffuse bodily and mental symptoms that, over time, can result in chronicity and loss of function (1). For subjects sick-listed due to musculoskeletal disorders, it is vital to prevent or reduce their pain, or at least to assist them in learning to cope with it (2). The complexity of dealing with their symptoms is aggravated by the interaction necessitated by their situation, between sick-listed individuals, their employers and the municipality, and this, too, has a bearing on their chances of returning to work (3, 4). In Denmark, municipalities are responsible for managing patient-oriented rehabilitation for individuals with work disability, and the task constitutes a major public health challenge for them. Unfortunately, a systematic review of community-based and workplace-based interventions designed to reduce musculoskeletal-related sickness absence concluded that no single intervention is more effective than any other (5).
However, physical activity interventions targeting individual elements through specific exercises have proved effective in reducing pain and improving muscular strength (6, 7) and increasing functional capacity, as measured by cardiorespiratory fitness, which is related to increased productivity (8). In addition, a systematic review (9) of the relationship between physical activity and reduction in sickness absence suggests a correlation, although, due to the poor quality of the studies included, the evidence is not convincing. More research is required into the effects of physical activity as a health promotion activity. Indeed, a positive effect of this physical activity intervention on return-to-work was found in the short-term perspective of 3 months. Our study of the short-term effect of physical activity as an intervention showed that the proportion of participants who returned to work after 3 months was significantly higher in Tailored Physical Activity (TPA) (n = 23 (50%) 95% confidence interval (95% CI) 0.38–0.62) compared with the reference group (REF) (n = 17 (36.2%) 95% CI 0.25–0.48), while the proportion of participants in the Chronic Pain Self-Management Program (CPSMP) (n = 22 (46.8%) 95% CI 0.35–0.59) was not significantly higher (10). In this study an active comparator arm was used, in the form of a patient education programme. This is known as the CPSMP and was designed to enhance the ability to cope with pain and offers the participants new skills in order to manage initiatives for promoting their health and to help them keep active in their daily life (11). The programme was already widely implemented in municipalities across Denmark (12) despite the lack of knowledge on the advisability of implementation given the current level of scientific knowledge (13). The present manuscript is an evaluation of the longer term (11-month follow-up) effects of the interventions.
The aim of the present study was to evaluate the longer term efficacy of TPA or CPSMP against a REF, by taking a group of sick-listed subjects with pain in the back or upper body and comparing them regarding return-to-work and duration of sickness absence. A further aim was to evaluate the efficacy of TPA or CPSMP vs REF on self-reported pain.
METHODS
Design and settings
This study was a parallel randomized controlled trial conducted in Sønderborg Municipality, Denmark, between 2011 and 2014. The complete study protocol is published in 2013 by Andersen et al. (14). The protocol was approved by the Regional Scientific Ethics Committee for Southern Denmark (project-ID S-20110040) and The Danish Data Protection Agency. The trial is registered in the ClinicalTrials.gov, number NCT01356784. In the present paper the longer term results, i.e. 8 months after termination of TPA, corresponding to 11 months after inclusion for primary outcome and selected secondary outcomes, reflected the effect of participating in TPA. The results from a short-term perspective have also been reported in 2015 by Andersen et al. (10).
All interventions, tests and measurements were performed at the Healthcare Centre in Sonderborg Municipality.
Study population, recruitment and randomization
The participants, all sick-listed subjects, were recruited from lists of potential participants, which were generated from a database and provided every second month by the Department of Financial Security in Sonderborg Municipality. The municipality has several categories listing subjects’ primary reasons for sick-listing. This categorization is based on self-reported primary disorders. Participants were recruited from the 2 main categories of sick-listed subjects with disorders in: (i) the shoulder/arm/hand; and (ii) the back/hip/neck. Subjects with hip problems were excluded at first telephone contact. If the subjects had been diagnosed with an illness, such as cancer or cardiac or neurological diseases, they were not included in the 2 selected categories.
All eligible participants received written information, including an invitation to an information meeting. After the meeting, the participants gave written informed consent if they agreed to enrol in the study. The sick-listed subjects from Sonderborg Municipality were recruited regardless of any previous history of being sick-listed, and both employed and unemployed subjects were recruited.
Inclusion criteria were that participants should have been sick-listed for a maximum period of 9 weeks at the time of inclusion due to pain in the back or the upper body (i.e. back/neck/shoulder/arm/hand). The study aimed to include all sick-listed subjects who fulfilled these criteria. However, certain exclusion criteria concerning medical safety came to be applied. For example, those with, e.g. recent surgery and other medical diagnoses constraining physical activity, were regarded as ineligible for the study.
During the intervention some participants were prevented from full participation due to part- or full-time return-to-work or engagement in rehabilitation in another sector. This might be due to their undergoing a test for work ability decided by their social worker. In some situations participants were offered flexible working hours, which meant that they were offered the opportunity to continue participation in interventions. Unfortunately, not all workplaces offered such an opportunity.
Participants were recruited in 11 time sequences, coordinated so that all sick-listed subjects were offered participation and none was lost between 2 sequences of recruitment. The recruited participants were randomized into permuted blocks of 3 and 6, according to computer-generated random numbers, to participate in TPA, CPSMP or REF. Participant flow was registered as recommended by the CONSORT (15).
Interventions
All participants received individual health guidance. The REF group received health guidance only, while the 2 intervention groups were offered 2 types of add-on health promotion activities.
Health guidance
Health guidance was a 1.5-h dialogue with a health supervisor, centred around the participants’ lifestyle, motivation, resources and power to act. The participant was offered the chance to prepare a health plan, and the health supervisor provided ideas and support for increasing well-being in everyday life. Add-on health promotion activities started 1 week after baseline evaluation, health guidance and randomization.
Tailored Physical Activity group
In addition to health guidance, this group received tailored physical activity in teams of up to 10 participants (14). TPA included a standardized combination of aerobic fitness and strength training for 50 min, 3 times per week, over 10 weeks, supervised by physiotherapists. It started with a 5-min warm-up, followed by aerobic fitness training for 20 min. After that the participants were referred to 1 of 3 standardized strength training programmes based on their primary region of musculoskeletal problems (neck and shoulder pain; arm and/or hand pain; lower back pain). During the following weeks, training was tailored to the participant’s current training status and pain problems (16). Progression was tailored to the participant’s current status and pain problems (16). The physiotherapists used their professional judgement to match demands in individual programmes, based on the response of musculoskeletal condition.
Chronic Pain Self-Management Program group
This active comparator group received CPSMP in addition to health guidance (14). CPSMP is a standardized programme of 2.5 h in a weekly workshop lasting 6 weeks. Group sizes were between 12 and 18, designed for people with primary or secondary diagnosis of chronic pain. Workshops were led by 2 trained facilitators (non-health professionals) who had chronic pain. Topics covered in the teaching sessions included techniques to deal with problems, such as fatigue, exercises, the use of medications and communication tools. Classes built the participants’ confidence to manage their own health and to help them stay active in their daily lives (11, 17).
Outcomes
The primary end-point was the participants’ sick-listed status (yes/no) 11 months after their first day of sick leave. The co-primary end-point (11 months) was the duration of the sickness absence period, as registered by the Department of Financial Security in Sønderborg Municipality. The choice of timing of primary end-point measurement at 11 months was to avoid data being influenced by a compulsory censoring in register status as not sick-listed after 12 months. A secondary outcome measurement was performed at baseline and repeated in the short term after 3 months (10) and in the longer term as reported in this paper.
Self-reported secondary outcomes were collected from questionnaires and from health-related, anthropometrical and physical capacity measurements (14). The latter are specified below and more detailed background for outcome measures is published in Andersen et al. (14). Height and body weight were measured without shoes and wearing light clothes. Aerobic capacity was estimated with the Aastrand Rhyming Test and performed by trained physiotherapists (18).
The questionnaire used as a basis for findings in the present paper consisted mainly of standardized and validated scales (14). Pain was measured on a visual analogue scale (VAS) using a 100-mm VAS (20). Work ability was assessed with a single-item measure that was originally part of the widely used Work Ability Index (19). However, recent studies have shown that the single-item question is a reliable and easy tool with validity comparable with the full index (20). The question was “Imagine that your work ability is worth 10 points when it is at its best. How many points would you give your present work ability?” A numerical rating scale was used, in which 0 represents “not able to work” and 10 represents “the highest work ability” (21). Kinesiophobia, the subjects’ dysfunctional beliefs about their physical activity was assessed with Tampa Scale for Kinesiophobia. Avoidance behaviour can be one mechanism in sustaining chronic pain disability (22, 23), and this is assessed with a 17-item questionnaire about fear of (re)injury due to movement.
Blinding
Healthcare professionals and participants were blinded to the results of baseline assessment and healthcare professionals who were outcome assessors were blinded to participants’ allocation.
Statistical analysis
A power calculation was carried out based on the assumption that 70% or more of the participants in the TPA group and 43% of the participants in the REF group would return-to-work during the period. A sample size of 46 individuals in each group was required to achieve greater than 80% statistical power (2-sided, alpha = 0.05) necessary for detecting a relevant difference on the primary outcome (10, 14).
Differences in baseline characteristics were tested with Pearson’s χ2 for distribution of categorical variables, and continuous variables were tested with one-way analysis of variance (ANOVA). As the primary outcome was change in the proportion of not sick-listed participants, the differences between the groups were analysed using a χ2 test (1-sided 95% CI). Time on sick-leave across the groups was estimated with Kaplan–Meier, and a Cox proportional hazard model was used to measure effectiveness of TPA and CPSMP relative to REF, as hazard ratio ((HR) (95% CI)).
When comparing groups from baseline to follow-up, a paired-samples t-test was used for analysis of continuous variables within groups, and Dunnett’s test was used for comparison between groups. TPA and CPSMP were compared with REF and the p-values for the multiple comparisons are reported for each secondary outcome. All analyses were in accordance with the intention-to-treat principle, i.e. all randomized participants are included in the analysis, missing values being substituted by carried forward or backward measured values leaving a null delta-value.
Microsoft Excel 2010 was used for analysis of primary outcome and all other analyses made use of IBM SPSS Statistics for Windows, Version 21.0. (IBM Corp., Armonk, NY, USA).
RESULTS
A total of 141 sick-listed subjects were included as participants in this randomized controlled trial. The flow of participants’ progress is shown in Fig. 1. After randomization, one participant withdrew informed consent from the trial, and data relating to this person was removed from all analysis, leaving 140 participants in the primary analyses.
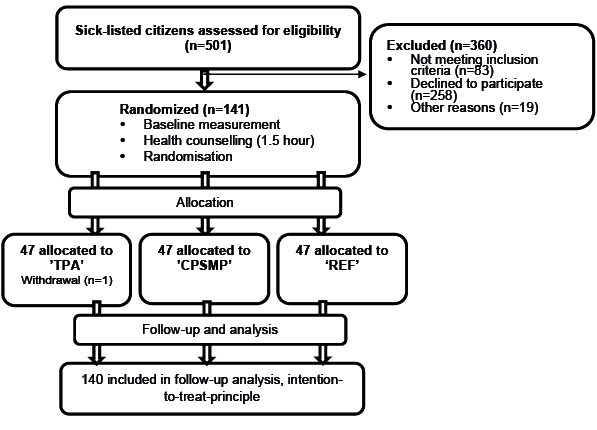
Fig. 1. Flow of participants through the trial until long-term follow-up. TPA: Tailored Physical Activity group; CPSMP: Chronic Pain Self-management Program group; REF: reference group.
Baseline characteristics were collected from a questionnaire and these were similar across the 3 groups.
The mean age of the participants were 45.2 years (SD 10.5 years), 25 participants had no further education, 70 had minimal further education, 32 had taken short/medium courses/higher education and 8 had higher educations. Their mean BMI was 28.3 (SD 5.3). Among participants 55.3% had previous sickness absence caused by present issues.
The proportion of participants who had returned to work after 11 months was not significantly different in TPA (n = 28 (61%), 95% CI 0.47–0.75, p = 0.38) or CPSMP (n = 28 (60%), 95% CI 0.46–0.74, p = 0.34) compared with REF (n = 30 (64%), 95% CI 0.50–0.78). The HR for time until return-to-work did not suggest a significantly higher rate for return-to-work for TPA (HR = 0.99; 95% CI 0.59–1.66) or for CPSMP (HR = 0.90; 95% CI 0.54–1.51).
The Kaplan–Meier method was used for analysis of duration of sick-leave from the first day of sick-leave. In Fig. 2 the survival curve for TPA and REF intersect. Thus differences between curves are not significant.
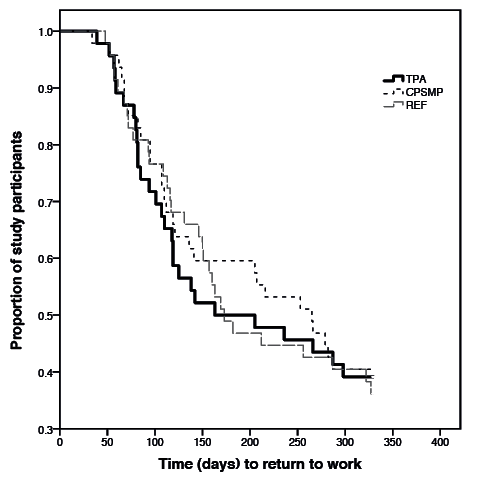
Fig. 2. Reduction in proportion of study participants due to return to work from the first day of sick-leave throughout the follow-up period. For example, after 150 days approximately 48% of participants in TPA and 40% in CPSMP and REF have returned to work. TPA: Tailored Physical Activity group; CPSMP: Chronic Pain Self-Management Program group; REF: reference group.
For pain, BMI, aerobic capacity, work ability and kinesiophobia non-significant changes were found between groups (Table I). At long-term follow-up pain decreased significantly from baseline to follow-up within all groups, and work ability and kinesiophobia also showed significant improvements within all groups. Aerobic capacity improved significantly within CPSMP and REF, but, for TPA, the improvement was non-significant.
|
Table I. Secondary outcomes (mean (standard deviation; SD)) at longer term follow-up |
||||||||||||||
|
TPA (n = 46) |
CPSMP (n = 47) |
REF (n = 47) |
p-value ΔTPA or ΔCPSMP/ΔREF |
|||||||||||
|
Baseline |
Long-term follow-up |
p-value |
Baseline |
Long-term follow-up |
p-value |
Baseline |
Long-term follow-up |
p-value |
||||||
|
Mean (SD) |
Mean (SD) |
Mean (SD) |
Mean (SD) |
Mean (SD) |
Mean (SD) |
|||||||||
|
Pain, VAS 0–100 (mm)* |
62.5 (26.5) |
41.5 (29.9) |
< 0.01 |
64.7 (19.7) |
53.8 (29.9) |
0.02 |
62.1 (24.7) |
51.6 (31.9) |
0.03 |
0.11 |
||||
|
BMI (kg/m2)* |
28.4 (5.1) |
28.5 (4.6) |
0.83 |
28.5 (5.1) |
28.2 (5.1) |
0.06 |
28.1 (5.3) |
27.8 (5.0) |
0.13 |
0.42 |
||||
|
Aerobic capacity (ml/min/kg)* |
26.5 (5.4) |
28.1 (7.5) |
0.09 |
25.2 (8.8) |
27.4 (8.8) |
0.01 |
26.4 (6.0) |
28.4 (6.0) |
0.01 |
0.85 |
||||
|
Work ability, 0–10 (score)* |
3.1 (2.7) |
5.0 (3.1) |
< 0.01 |
2.5 (3.4) |
4.8 (3.4) |
< 0.01 |
2.9 (2.8) |
4.8 (2.9) |
< 0.01 |
0.66 |
||||
|
Kinesiophobia, TSK-17, 17–68 (score)* |
34.2 (8.5) |
30.0 (7.8) |
< 0.01 |
36.6 (9.2) |
32.2 (9.2) |
< 0.01 |
36.4 (9.2) |
32.8 (9.7) |
< 0.01 |
0.88 |
||||
|
*n = 41–47; TPA: Tailored Physical Activity group; CPSMP: Chronic Pain Self-management Program group; REF: reference group; VAS: visual analogue scale; BMI: body mass index; SD: standard deviation; Δ: delta/change from baseline to follow-up. |
||||||||||||||
DISCUSSION
Recently, another return-to-work study (24) in Denmark showed that effects can differ substantially between municipalities. For 2 of 3 municipalities in that study, results on return-to-work are in line with the present study in Sønderborg Municipality. They indicate that the lack of effect may be influenced by contextual factors and that variety in length of sickness absence causes variety in effect. This explanation may be relevant for our study, in which more than half of participants had previously been sick-listed because of present health issues. However, we do not know the length or number of periods of previous sickness absence. A trend was visible indicating a faster return-to-work for TPA at the beginning of the intervention period, and at 3 months a significantly higher proportion had come off sick-leave (10), but this effect subsequently decreased, and after 180 days the effect was neutralized and only non-significant differences were seen. Nor were significant group differences found for health- and work-related secondary outcomes. Results show that participants, in general, had a BMI consistent with overweight, that work ability increased and kinesiophobia decreased with time, but also that pain decreased from 62.5 to 41.5 mm in TPA, i.e. twice as much as in REF and CPSMP, but this difference was non-significant.
On the other hand, in the longer term effects of TPA and CPSMP may not be expected to be maintained, because interventions terminated 8 months before this follow-up, and participants have not been in any kind of continued intervention until this follow-up. A systematic review (25) emphasized the lack of studies systematically describing interventions and settings and evaluating longer term benefits from return-to-work programmes. The present trial meets the requested requirements, but still confirms the conclusion of the systematic review showing important effects in the shorter term but no long-term effects on return-to-work. In line with this, another study (26) of a physical exercise programme for increasing return-to-work also showed a lack of effects. In contrast, a coordinated and tailored work rehabilitation programme carried out by interdisciplinary teams did show a longer term effect on sickness absence (27). This indicates that a multifaceted intervention involving the workplace may be needed for a longer term effect.
A qualitative study (28) related to this trial was based on interviews with participants. It indicated that TPA was a means of progression, e.g. of return-to-work, but that the learning aspect was questionable. Compared with the results from this longer term follow-up, it is evident that participants did not improve their own competencies for physical activity. Nor did they learn to maintain progression after the termination of the established interventions, as it was felt to be a here-and-now experience of physical activity. On the other hand, CPSMP had the potential for learning to make progression in everyday life (28), even though we could not show any effect of CPSMP on the longer term in this trial. An explanation of the lack of effect of CPSMP may be related to the diversity in attitudes among participants towards a patient education programme. Even though some participants took advantage of and, in general, appreciated talking with “others in the same boat”, it was also clear that there were differences between participants as regards their willingness to share the trials demanded by their ill health. A study by Emslie et al. (29) showed that the main attraction in a health-related intervention was the active part rather than the part with focus on sharing of burden of illness. This highlights the complexity of designing return-to-work interventions that are effective in the longer term. This complexity is, in part, a result of the diversity of personal needs and of acceptance of the employment situation (30). To progress here, in future studies it will be relevant to investigate how a multidisciplinary, coordinated and tailored return-to-work intervention works and how effects can be maintained. Aust et al. (31) also concluded that a better understanding of challenges is needed when implementing recommended return-to-work programmes. Seen in the context of the conclusion of a systematic review by van Vilsteren et al. (32), showing that intense physical rehabilitation programmes had minimal effect on reducing sick leave at 12 months follow-up, it is even more evident that it is important to investigate the significance of follow-up of interventions aimed at improving participants’ continued levels of physical activity. This is underlined by the positive influence exerted by the physical activity intervention in the present study on the proportion of sick-listed subjects who returned to work in the short term.
One limitation of this study is that some of the eligible participants declined to participate. They had a number of different reasons, for example their return-to-work was already scheduled, transportation was too expensive, they lacked the energy to participate or, their illness was not sufficiently severe to make it a legal requirement for them to participate, even though they could not manage to go to work. A further limitation is that when participants did return to work and were successful in relation to our primary outcome, their compliance regarding intervention often decreased due to the time demands of their job and this was often a barrier for participation in intervention activities.
The strengths of the study are that primary outcome data are obtained directly from the municipality’s registration. This means that we have complete data on follow-up, data were not self-reported and are therefore not prone to information bias. The intention-to-treat principle with carrying forward and backward of missing values was applied on secondary outcomes. This principle may have underestimated intervention effects on secondary outcomes. A further strength is that we assessed the effect of the interventions in a real municipality setting. This increases the external validity of the study, and reduces the difficulty of extending generalizations to other interventions.
In conclusion, on the longer term, after 11 months TPA, REF and CPSMP show similar patterns of facilitating return-to-work. This is new and additional knowledge, compared with the 3-month findings reported previously (10), showing that TPA seems to facilitate a faster return to work.
ACKNOWLEDGEMENT
The study was funded by the Sønderborg Municipality to evaluate and improve initiatives for subjects. The municipality has received funding from the Ministry of Interior and Health to carry out an intensified initiative to assist people with chronic illness.
The authors declare no conflicts of interest.
REFERENCES

