PREVALENCE OF COMORBID DEPRESSIVE SYMPTOMS IN REHABILITATION: A CROSS-INDICATION, NATIONWIDE OBSERVATIONAL STUDY
Martin Brünger, MPH, and Karla Spyra, PhD
From the Institute for Medical Sociology and Rehabilitation Science, Charité - Universitätsmedizin Berlin, Berlin, Germany
OBJECTIVE: Patients in rehabilitation with comorbid depressive disorders display increased morbidity, mortality and inability to work. The aim of this study is to determine the prevalence of comorbid depressive symptoms in rehabilitation.
METHODS: A total of 6,000 patients were contacted by post at the same time as receiving approval for their medical rehabilitation from German Federal Pension Insurance. Depressive symptoms were assessed using the Patient Health Questionnaire (PHQ-2). Results were compared with prevalences in the general population by analysing the German Health Interview and Examination Survey for Adults (DEGS).
RESULTS: A total of 2,152 out of 5,891 patients participated in the study (response rate: 36.5%). The prevalence of self-reported depressive symptoms was 33.1% (women 34.1%, men 31.3%). In contrast, 7.8% of the German general population reported depressive symptoms (women 9.4%, men 6.2%). The highest prevalences were found in neurological (36.4%) and orthopaedic (35.6%) rehabilitation, the lowest in cancer rehabilitation (23.0%). Depressive symptoms were significantly associated with higher comorbidity and impairment due to pain, with lower social support and self-efficacy and with specific work-related problems.
CONCLUSION: A short routine screening yielded a positive test result for depressive symptoms in a third of rehabilitation patients, thus approximately four times higher than in the general population. This is valuable information in order to better adjust treatment to patient needs.
Key words: comorbidity; depression; self-assessment; rehabilitation; screening; cross-sectional studies.
J Rehabil Med 2016; 00: 00–00
Correspondence address: Martin Brünger, Institute for Medical Sociology and Rehabilitation Science, Charité - Universitätsmedizin Berlin, Luisenstraße 13a, DE-10117 Berlin, Germany. E-mail: martin.bruenger@charite.de
Accepted Aug 23, 2016; Epub ahead of print Oct 13, 2016
INTRODUCTION
Medical rehabilitation follows a multidisciplinary approach based on the International Classification of Functioning, Disability and Health (ICF) and its bio-psycho-social model of illness. Rehabilitation should tackle the patient’s possible multimorbidity. In this context, comorbid mental disorders play a decisive role. An adverse effect of comorbid depressive disorders on the individual’s health and the social security system has been shown in numerous studies. Depressive comorbidity is associated with lower quality of life (1), increased utilization of healthcare benefits, and higher rates of long term sick-leave (2). The number of additional diseases is higher in the presence of depressive comorbidity, and mortality risk is increased (3).
Cancer, cardiac and diabetic patients are hospitalized for a prolonged period of time if they additionally have mental comorbidity (3). Depressive comorbidity is also associated with increased costs of medical care (4), an increased issuing of medical certificates (5), and a higher rate of disability pensions (6).
Numerous prevalence studies of mental disorders were conducted within the general population, many of them under the umbrella of the World Mental Health Survey Initiative (7). Other studies deal with the epidemiology of depressive disorders as a comorbidity of different somatic diseases, such as arthritis (8), chronic back pain (9), heart disease (10), diabetes (11) and multiple sclerosis (12). Reported odds ratios range from 1.4 to 2.3 for major depression and 1.3 to 2.8 for dysthymia compared with healthy individuals. These study participants were not, however, recruited in rehabilitation settings but from the general population.
The comorbidity of depression within different fields of rehabilitation, such as cardiology and oncology, remains uncertain. This is surprising, since depression is widespread within the general population and its adverse health effects are well known. A prevalence estimation of depressive comorbidity could facilitate a more precise planning of requirements in rehabilitation facilities, and thus improve the therapy and recovery of patients. Härter et al. reported a point prevalence of 12.3% for depressive symptoms in rehabilitation. This study was, however, performed in non-randomly selected single inpatient facilities within only one region in Germany (13). Therefore, these results cannot be considered as representative on a nationwide level.
For these reasons, the aim of this work is to determine the prevalence of comorbid depressive symptoms in rehabilitation patients across all major disease groups in a nationwide study in Germany. In addition, it aims to examine the association of self-reported depressive symptoms with other impairments and resources relevant for rehabilitation. A comparison with the German general population will be provided based on analyses of the German Health Interview and Examination Survey for Adults (DEGS).
METHODS
Study design
A nationwide observational study was conducted in Germany. A total of 6,000 persons insured with the Deutsche Rentenversicherung Bund (German Federal Pension Insurance) were contacted by post and asked to complete a questionnaire at the same time as they received approval for their medical rehabilitation (between September and November 2011). Patients were included in the study based on approval for their medical rehabilitation according to §15 SGB VI (German social security code). These are rehabilitations with the aim of securing or restoring the ability to work. In Germany, rehabilitation follows a multidisciplinary and multimodal approach that usually lasts 3 weeks in full-time care, although an optional additional week can be requested. Rehabilitation patients are treated in specialized inpatient or outpatient facilities that focus on 1 or more fields of rehabilitation defined by disease groups. Patients who were treated in the 6 most common disease groups were included in the study. These disease groups are: musculoskeletal diseases (admission diagnosis according to the International Classification of Diseases ICD-10: M00–M99), diseases of the circulatory system (I00–I99), gastrointestinal, endocrine, nutritional and metabolic diseases (E00–E90, K00–K93), diseases of the respiratory system (J00–J99), neoplasms (C00–D48), and diseases of the nervous system (G00–G99). The questionnaire had to be completed prior to the start of rehabilitation to rule out effects of the medical rehabilitation on the response.
To allow separate evaluations according to disease groups, random sampling was conducted in combination with stratification according to disease groups of 1,000 insured people each. Within these 6 disease groups the most common diseases include chronic back pain (M50–M54), stroke (I61–I64), coronary heart disease (I20–I25), hypertension (I10–I15), diabetes (E10–E14), asthma (J45), breast cancer (C50) and multiple sclerosis (G35) (14). The chosen sample size allows us to determine the prevalence of depressive symptoms with a confidence level of ±5 percentage points at the level of single disease groups and of ±2 percentage points for the combined sample, assuming a response rate of 32% and a prevalence of 30%.
Data collection and instruments
Depressive symptoms were measured using the short version of the Patient Health Questionnaire (PHQ-2) (15). The PHQ-2 is based on the 2 key diagnostic criteria for depressive disorders according to Diagnostic and Statistical Manual (DSM-IV). It allows us to assess both “little interest or pleasure in doing things” and “feeling down, depressed, or hopeless”, on 4-point Likert scales referring to a period of the 2 previous weeks. Depressive symptomatology is defined as a total PHQ-2 score of at least 3 points, while the instrument ranges between 0 and 6 points (15).
To include additional impairments and resources relevant for rehabilitation, further instruments were used (16): comorbidity was examined using the Self-Administered Comorbidity Questionnaire (SCQ) (17), impairment due to pain using the Pain Disability Index (PDI) (18), social support with a scale composed of the Indicators of Rehabilitation Status Questionnaire (IRES) (19), self-efficacy using the General Self-Efficacy Scale (GSE) (20), and specific work-related problems using the short version of the Screening Instrument for Detecting the Need of Work-Related Medical Rehabilitation (SIMBO) (21). For 90.8% of the participants we could link the assessment data with sociodemographic variables and medical history data concerning the rehabilitation (by using data from their insurance account). Whatever the reasons, we assume that a large part of the remaining 9.2% of participants did not start their granted medical rehabilitation (22).
Approval was obtained from the ethics committee of the Charité – Universitätsmedizin Berlin for these analyses. All participants gave written informed consent to participate in the study.
Data analyses
As the rate of missing data across all the scales was as low as 7.4%, only participants providing a complete record in terms of the assessment data were included. At first, the non-responses were analysed for essential sociodemographic variables on the basis of χ2 and Mann-Whitney U tests. We established weighting factors to improve the accuracy of the prevalence estimation. These weights account for the varying willingness to participate between men and women and for deviations in the drawn sample that occurred when compared with the sex distribution in rehabilitation in 2011. Due to the stratified sampling, cross-indication analyses were additionally weighted according to the distribution of disease groups in 2011 (14).
Prevalences of self-reported depressive symptoms and their 95% confidence intervals (95% CI) are reported for all rehabilitation patients, and stratified for sex, age and disease groups. Three age categories of approximately equal size were established (20–44, 45–54 and 55–65 years) and a χ2 test was performed to assess a linear trend.
To examine the association of depressive symptoms with other impairments and resources relevant for rehabilitation we built a logistic regression model with controls for sex, age, and their interaction. The binary dependent variable was depressive symptomatology, the other reported instruments served as continuous independent variables. The SIMBO was factored in as binary independent variable (specific work-related problem present vs not present). The significance level was defined as α = 0.05. The analyses were computed with the SPSS version 23 (IBM Corp.).
Additional analyses
To compare prevalences of depression in rehabilitation with the prevalence in the general population, the public use file of the DEGS was also analysed according to the PHQ-2 (23). The study design, response, weighting, and core characteristics of the sample are described elsewhere (24).
RESULTS
Prevalence of comorbid depressive symptoms in rehabilitation patients
Table I characterizes the study population. Of the 5,891 individuals who were successfully contacted and who met the inclusion criteria, 2,152 participated in the study (response rate 36.5%) (Fig. 1). In the complete case analyses there were 305–365 patients per disease group, and 1,992 participants overall.
|
Table I. Description and comparison of included study participants and the remaining sample |
|||||||
|
Sociodemographic characteristics and rehabilitation details |
Included study participants |
Remaining sample |
U-test/χ2-test p-value |
||||
|
n |
Mean (SD)/ |
n |
Mean (SD)/ |
||||
|
Age, years, mean (SD) |
1,992 |
50.4 (8.3) |
3,899 |
49.6 (9.5) |
0.069 |
||
|
Sex, % Men |
1,313 679 |
65.9 34.1 |
2,480 1,419 |
63.6 36.4 |
0.080 |
||
|
Settlement structurea, % Urban regions Regions with urbanization Rural regions |
885 635 472 |
44.4 31.9 23.7 |
1,811 1,214 873 |
46.5 31.1 22.4 |
0.303 |
||
|
Unemployed, % |
73 |
4.0 |
171 |
4.9 |
0.141 |
||
|
Inability to work 12 months prior to rehabilitation, % 6–12 months 3 to under 6 months Under 3 months None Not working |
303 188 871 362 85 |
16.7 10.4 48.1 20.0 4.7 |
612 336 1,474 688 187 |
18.6 10.2 44.7 20.9 5.7 |
0.104 |
||
|
Disease groups (weighting factorsb), % Musculoskeletal diseases (3.67) Diseases of the circulatory system (0.47) Gastrointestinal and endocrine diseases (0.33) Diseases of the respiratory system (0.44) Neoplasms (0.69) Diseases of the nervous system (0.38) |
332 305 340 340 365 310 |
16.7 15.3 17.1 17.1 18.3 15.6 |
648 691 649 647 614 670 |
16.6 17.2 16.6 16.6 15.7 17.2 |
0.061 |
||
|
Approved duration of rehabilitation, days, mean (SD) |
1,962 |
22.0 (3.1) |
3,713 |
21.9 (3.5) |
0.060 |
||
|
De facto duration of rehabilitation, days, mean (SD) |
1,809 |
25.1 (5.6) |
3,298 |
25.0 (6.2) |
0.170 |
||
|
aClassification according to the German Federal Institute for Research on Building, Urban Affairs and Spatial Development. bWeighting factors for distribution of sex and disease groups in medical treatment rehabilitations provided by the German Federal Pension Insurance 2011 (14). SD: standard deviation. |
|||||||
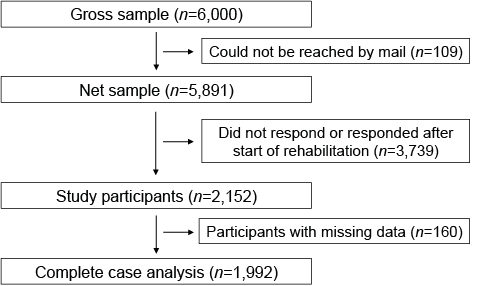
Fig. 1. Study participants.
The mean age of all participants was 50.4 years (standard deviation (SD) 8.3) (range 20–65 years). Almost two-thirds were women. Twenty percent of participants had no periods of inability to work, and the remaining participants had been unable to work for less than 3 months (48.1%), 3 to under 6 months (10.4%), or at least 6 months (16.7%) during the 12 months prior to rehabilitation. Of all participants, 4.7% registered as unemployed.
The de facto duration of rehabilitation was on mean 3 days longer than approved duration of rehabilitation (25.1 (SD 5.6) vs. 22.0 days (SD 3.1)). The non-response analyses did not reveal any significant differences between the included participants and the remaining sample in terms of all examined sociodemographic variables and rehabilitation details (Table I).
The prevalence of comorbid self-reported depressive symptoms was 33.1% (95% confidence interval (95% CI): 31.1–35.2). In women, the proportion was 34.1% (95% CI: 31.6–36.6), and thus numerically, but not significantly, higher than in men (31.3%; 95% CI: 27.7–35.1). The stratification according to age categories indicated a significant gradient (p = 0.038). The highest prevalence of depressive symptoms was found among rehabilitation patients under 45 years of age, revealing a proportion of 37.8% (95% CI: 33.0–42.6). Patients aged 55–65 years formed the group with the lowest proportion of depressive symptoms (31.2% (95% CI: 27.8–34.6)) (Fig. 2).
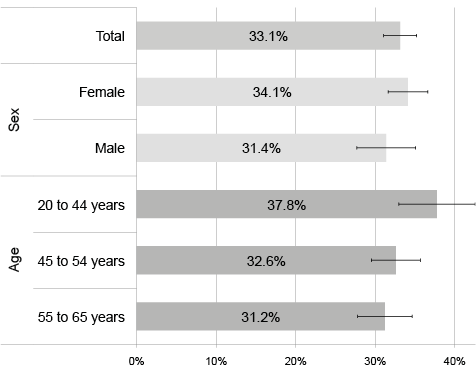
Fig. 2. Prevalence of comorbid depressive symptoms in rehabilitation patients stratified by sex and age (with 95% confidence intervals, n = 1,992). Weighted for disease groups in medical treatment rehabilitations provided by the German Federal Pension Insurance 2011, cross-gender analyses additionally weighted for distribution of sex (14).
Analyses according to disease groups showed the lowest prevalence of depressive symptomatology in cancer rehabilitation (23.0%; 95% CI: 18.7–27.3). The percentages were highest in neurological (36.4%; 95% CI: 31.1–41.8) and orthopaedic rehabilitation (35.6%; 95% CI: 30.4–40.7). In rehabilitation of patients with diseases of the circulatory or respiratory system and with gastrointestinal, endocrine, nutritional or metabolic diseases, the mean prevalences ranged from 29.6% to 33.1% (Fig. 3).
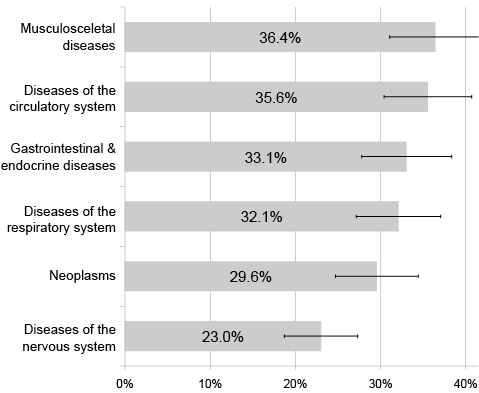
Fig. 3. Prevalence of comorbid depressive symptoms in rehabilitation patients stratified by disease groups (with 95% confidence intervals, n = 1,992). Weighted for distribution of sex in medical treatment rehabilitations provided by the German Federal Pension Insurance 2011 (14).
The regression model showed that depressive symptoms are significantly associated with higher comorbidity (OR = 1.09; 95% CI: 1.06–1.12) and higher impairment due to pain (OR = 1.05; 95% CI: 1.04–1.06), lower social support (OR = 0.94; 95% CI: 0.92–0.96), lower expectations of self-efficacy (OR = 0.91; 95% CI: 0.87–0.95) as well as with the presence of specific work-related problems (OR = 1.36; 95% CI: 1.08–1.71) (Table II).
|
Table II. Association of depressive symptoms and other impairments and resources relevant for rehabilitation |
||
|
Instruments (range) |
OR (95% CI) |
p-value |
|
Constant |
0.32 |
0.066 |
|
Comorbidity SCQ (0–39) |
1.09 (1.06–1.12) |
< 0.001 |
|
Impairment due to pain PDI (0–70) |
1.05 (1.04–1.06) |
< 0.001 |
|
Self-efficacy GSE (10–40) |
0.94 (0.92–0.96) |
< 0.001 |
|
Social support IRES (0–10) |
0.91 (0.87–0.95) |
< 0.001 |
|
Specific work-related problems SIMBO (yes/no) |
1.36 (1.08–1.71) |
0.009 |
|
Multivariate binary logistic regression adjusted for age, sex and its interaction; reciprocally adjusted effects of stated impairments and resources (n = 1,992). Corrected r2=0.293. Weighted for distribution of sex and disease groups in medical treatment rehabilitations provided by the German Federal Pension Insurance 2011 (14). 95% CI: 95% confidence interval; GSE: General Self-Efficacy Scale; IRES: Indicators of Rehabilitation Status Questionnaire; OR: odds ratio; PDI: Pain Disability Index; SCQ: Self-Administered Comorbidity Questionnaire; SIMBO: Screening Instrument for Detecting the Need of Work-Related Medical Rehabilitation. |
||
Prevalence of depressive symptoms in the general population
Out of 5,938 persons aged 18–64 years who are enlisted in the DEGS, those 98% with complete PHQ-2 data-sets were included in the analyses of the public use file. Overall, the prevalence of self-reported depressive symptoms was 7.8% (95% CI: 7.0–8.7). Women had a significantly elevated prevalence of 9.4% (95% CI: 8.2–10.8) compared with the men’s prevalence of 6.2% (95% CI: 5.3–7.3).
Mean prevalences were approximately 7% or 8% for each of the age groups; 8.0% for 18–44-year-old individuals (95% CI: 6.9–9.4), 7.3% for 45–54-year-olds (95% CI: 5.8–9.2), and 7.7% for 55–64-year-olds (95% CI: 5.8–10.1).
DISCUSSION
Approximately one-third of patients in rehabilitation were assessed as having depressive symptoms according to the PHQ-2. Therefore, the proportion of people with depressive symptoms is increased by a factor of approximately 4 in rehabilitation compared with the prevalence in the general population. A prevalence of 8.1% with depressive symptoms in the general population was ascertained in the DEGS (25). A marginally lower prevalence of 7.8% was found in our analyses of self-reported depressive symptoms within the DEGS by using the short version of the PHQ-2 instead of its original instrument PHQ-9. This is in accordance with a study comparing different instruments measuring depression, including PHQ-2 and PHQ-9 (26).
Gender differences were not statistically significant in rehabilitation despite the fact that in the general population women have a higher risk of depression than men (9.4% of women vs 6.2% of men show depressive symptoms). Higher rates of depressive symptoms in women and in younger patients are in accordance with other surveys (25).
The particularly high prevalences in orthopaedic and neurological rehabilitation seem plausible. In fact, the most frequent diagnoses in these areas of rehabilitation are chronic back pain and multiple sclerosis (14). For these 2 diagnoses, a high prevalence of depressive comorbidity has been described in epidemiological population-based studies (9, 12). The significant correlation between depressive symptoms and other examined impairments and resources confirms preliminary studies (27–31). In this study, the prevalence of self-reported depressive symptoms in rehabilitation was examined for the first time based on a nationwide data collection. Another German study was conducted in single rehabilitation hospitals between 1998 and 2004, reporting a point prevalence of 12.3% for depressive symptoms (13). Due to the selective sampling in single inpatient facilities confined to a certain region only, the results cannot, however, be considered as representative. Moreover, they used different instruments from the ones in our study. It therefore remains uncertain whether the identified differences in prevalences are due only to methodological reasons or reflect reality.
Strengths and limitations of the study
In our study, we depict medical rehabilitation throughout Germany across all essential disease groups. Inpatient, as well as outpatient, rehabilitation settings were included. The 6 disease groups that were included represent a total of 95.7% of all rehabilitation measures realized by the German Federal Pension Insurance (excluding rehabilitation due to mental disorders) (14). The stratified study design allowed additional evaluations for single disease groups. The response rate of 36.5% is comparable with other epidemiological studies (32). Due to the limited time between approval and start of rehabilitation it was not possible to send out follow-up letters. The extensive non-response analyses based on sociodemographic data and duration of rehabilitation did not provide an indication for a relevant selection bias (Table I). For the cross-gender analyses, the slight variation in willingness to participate between men and women was factored in correspondingly. Additional analyses, which compare participants with the remaining sample with regard to rehabilitation variables that are significantly related to the presence of depressive symptoms, also did not show any significant differences (data not shown). This includes the amount of psychotherapeutic therapy during the rehabilitation, reduced psychological resilience, and the recommendation for a psychological counselling or treatment after rehabilitation by the responsible physician or psychologist at the end of rehabilitation. Selection bias cannot be ruled out completely, but there is no evidence for substantial selection bias. Nevertheless, both a higher as well as a lower prevalence of depressive symptoms is possible.
In terms of generalizability it must be considered that the results cannot necessarily be transferred to so-called follow-up rehabilitation into which patients are moved directly from a hospital. Follow-up rehabilitation may be applied, for example, in patients having had an implantation of an endoprosthesis or chemotherapeutic treatment. The limitation of this study to conventional medical rehabilitations might also explain why the prevalence of depressive symptoms was less elevated in cancer rehabilitation compared with the other disease groups. We believe that this is because usually approximately one year passes from the time when cancer was diagnosed until one enters a non-follow-up rehabilitation, which is a considerable period of time for adapting to normal life. The exclusion of follow-up rehabilitations resulted from the differing application procedure and the insurants’ accessibility via the post (14).
We are aware of the limitations of this study, which arise due to the method of recruitment of patients. The German Federal Pension Insurance is by far the largest payer of medical rehabilitation; it insures approximately 34 million people (out of a total of 81 million citizens in Germany) and realizes approximately 450,000 medical rehabilitations per year (14). Nonetheless, the results cannot be transferred unconditionally to rehabilitation patients sponsored by other payers. This applies in particular to the statutory health insurance, which is primarily responsible for rehabilitations realized at post-working age, while the German Pension Insurance focuses on rehabilitation for the working-age population.
Another limitation could be that our measurement is a scale of self-reported depressive symptoms. It has to be emphasized that PHQ-2 does not deliver a diagnosis of clinical depression. According to a validation study, PHQ-2 provides a sensitivity of depressive disorders of 79% and a specificity of 86% (15). PHQ-2 has a similar diagnostic accuracy as other self-evaluation instruments, such as PHQ-9 and the Hospital Anxiety and Depression Scale (HADS) (33, 34). PHQ-2 can be applied as a first-stage screening instrument, but further diagnostic steps should follow.
Conclusion
The prevalence of comorbid depressive symptoms in rehabilitation is 33.1%; approximately 4 times higher than in the German general population. A significant association of depressive symptoms with impairment due to pain, specific work-related problems, a higher comorbidity score, lower self-efficacy and lower social support was observed. Thus, a routine depression screening of all rehabilitation patients seems appropriate, since depressive impairments in rehabilitation seem to have a substantial prevalence. Patients could benefit if treated appropriately, since mental comorbidity can have adverse effects on rehabilitation outcomes (35). The German Pension Insurance developed recommendations for a screening of mental comorbidity in rehabilitation facilities (36). A corresponding screening for psychological symptoms implemented already into the application process for medical rehabilitation could improve the future distribution to suitable rehabilitation facilities offering specific and well-structured treatment concepts customized to patients with mental comorbidity. In some orthopaedic and cardiac rehabilitation facilities in particular, these structured and prolonged (4 weeks in full-time) behavioural-medical rehabilitation programmes have already been established (37). In addition, there are practical recommendations for psychological interventions in multidisciplinary rehabilitation concerning various somatic diseases (38, 39). The concept of medical rehabilitation in Germany is based on the ICF and its bio-psycho-social model. It offers a solid general framework of integrated rehabilitation care for somatic and mental impairment. Systematic reviews support that multidisciplinary rehabilitation including psychological interventions improves patient outcomes, e.g. concerning chronic low back pain (40).
In Germany, the payer is responsible both for the approval of a medical rehabilitation and for selecting an appropriate inpatient or outpatient rehabilitation facility (based on application documents). Unlike, for example, for work-related impairments, self-evaluation instruments for the assessment of depressive symptoms, such as the Patient Health Questionnaire, have not yet been implemented routinely into the application documents. A screening for mental comorbidities could provide the payer with information about a potential comorbid mental impairment when a suitable rehabilitation facility is needed. An economic screening instrument is available with, for example, the PHQ-2 (33). A more differentiated allocation to rehabilitation facilities corresponding to the patient’s impairment situation could potentially lead to a more needs-oriented care in medical rehabilitation.
ACKNOWLEDGEMENTS
The authors would like to thank all rehabilitation patients for their willingness to participate in this study, as well as the associates from the German Federal Pension Insurance and the Charité – Universitätsmedizin Berlin who provided particular support during the process of data gathering and editing.
The manuscript is based on a research project supported by the German Federal Pension Insurance (grant number: 8011-106-31/31.27.16). The authors’ institution received further funding by the German Federal Pension Insurance. The funding agency had no influence of the interpretation of data and the final conclusions drawn.
REFERENCES

