Shamay S. M. Ng, PhD1, Kat K. C. Au, BSc (Hons)1, Emily L. W. Chan, BSc (Hons)1, Daisy O. M. Chan, BSc (Hons)1, Ginger M. Y. Keung, BSc (Hons)1, Joanna K. Y. Lee, BSc (Hons)1, Patrick W. H. Kwong, MSc1, Eric W. C. Tam, PhD2 and Shirley S. M. Fong, PhD3
From the 1Department of Rehabilitation Sciences, Faculty of Health and Social Sciences, 2Interdisciplinary Division of Biomedical Engineering, Faculty of Engineering, The Hong Kong Polytechnic University and 3School of Public Health, Li Ka Shing Faculty of Medicine, The University of Hong Kong, Hong Kong (SAR), China
OBJECTIVE: To examine the effect of acceleration and deceleration distance (0, 1, 2 and 3 m) on the comfortable and maximum walking speeds in: (i) the 5-m walk test (5mWT); and (ii) the 10-m walk test (10mWT) in people with chronic stroke.
DESIGN: Cross-sectional study.
SETTING: University-based rehabilitation centre.
SUBJECTS: Thirty individuals with chronic stroke.
METHODS: Timed walking at comfortable and maximum walking speeds in the 5mWT and 10mWT with different acceleration and deceleration distances (0, 1, 2 and 3 m).
RESULTS: The comfortable walking speed in the 5mWT with 0 m acceleration and deceleration distance was significantly slower than that with 1, 2 or 3 m acceleration and deceleration distances (p < 0.0083), but there was no significant difference among 1, 2 and 3 m acceleration and deceleration distances. No significant difference was found in the maximum walking speed in the 5mWT, or in the comfortable and maximum walking speeds of the 10mWT.
CONCLUSION: Adoption of 1 m acceleration and deceleration distance is recommended when measuring the comfortable walking speed in the 5mWT in people with stroke. Neither acceleration nor deceleration distance is needed when measuring the maximum walking speed in the 5mWT, the comfortable walking speed or the maximum walking speed in the 10mWT.
Key words: acceleration; deceleration; walking; stroke; rehabilitation.
J Rehabil Med 2016; 48: 666–670
Correspondence address: Shamay S. M. Ng, Department of Rehabilitation Sciences, The Hong Kong Polytechnic University, Hong Kong (SAR), China. E-mail: Shamay.Ng@polyu.edu.hk
Accepted Jun 1, 2016; Epub ahead of print Aug 18, 2016
INTRODUCTION
Stroke is a common and worldwide cause of long-term disability, and walking was commonly impaired in people with stroke (1, 2). Although some people with stroke can walk independently, many walk with compensating strategies that significantly reduce their walking speed and endurance (3, 4). Among different walking tests, walking speed has been shown to be the strongest independent predictor of self-reported motor function in people with stroke (5).
The 10-m walk test (10mWT) was developed 20 years ago to measure walking speed (6). It is now widely used to measure the walking speed of healthy adults (5, 7) as well as patients with neurological disorders (8), including people with stroke (1, 4, 8–15). It involves walking for 10 m at comfortable and maximum speeds, which is timed and walking speed is calculated. In recent decades, the 5-m walk test (5mWT) has also evolved in response to the reduced walking endurance of patients and limited clinical space (4, 14, 15, 16). Both the 5mWT and the 10mWT have shown good reliability in assessing the walking speed in people with stroke (intraclass correlation coefficient (ICC) of the 5mWT = 0.86; and the 10mWT at a comfortable speed = 0.90–0.97; 10mWT at maximum speed = 0.95–0.98) (2, 15). The good validity of these measures is reflected by their excellent correlation with functional activities, including balance and mobility (9). In addition, the 10mWT is sensitive to a clinical improvement (standard error of measurement at comfortable speed = 7.9%; maximum speed = 5.7%) (2).
Reaching a steady walking speed in the 5mWT and 10mWT involves acceleration and deceleration distance (17). The total walkway length has a significant influence on walking speed (16). However, the acceleration and deceleration distance adopted in previous studies using the 5mWT and 10mWT was not standardized. Various studies have adopted acceleration and deceleration distances of 0 m (1, 5, 11), 0.5 m (13), 1.5 m (14) and 2 m (2, 7, 8, 10, 12, 15), or even not mentioned it (3, 9). To our knowledge, no published study has examined the effect of acceleration and deceleration distance on comfortable and maximum walking speeds in either the 5mWT or the 10mWT in people with stroke.
The aim of this study is to examine the effect of acceleration and deceleration distance (0, 1, 2 and 3 m) on comfortable and maximum walking speeds in (i) 5mWT and (ii) 10mWT in people with chronic stroke.
METHODS
Participants
This was a cross-sectional study. Participants were included if they: (i) had been diagnosed with stroke for more than 1 year, (ii) were at least 50 years old, (iii) were able to walk at least 16 m with or without walking aids, but without any manual assistance, (iv) could follow instructions in Cantonese or English, (v) scored at least 7 on the Abbreviated Mental Test (18), and had a stable general medical condition that would allow them to participate in the test.
Participants were excluded if they had: (i) co-morbid neurological disorders other than stroke, for example, Parkinson’s disease, (ii) unstable medical or orthopaedic conditions that might affect their walking performance.
Calculated via G* Power 3.1.9.2, a sample size of ≥ 29 is required to achieve a statistically significant difference for an effect size of difference f = 0.1, setting the level of statistical significance at α = 0.05 and the power at 80% (β = 0.2). Thirty participants (21 men, 9 women with mean age and standard deviation (SD) 61.23 (SD 6.65)) with a mean post-stroke duration of 10.09 (SD 4.66) years were recruited from a local self-help group in Hong Kong (Table I).
|
Table I. Descriptive characteristics of the participants (n = 30) |
||
|
Variables |
n |
% |
|
Sex (male/female) |
21/9 |
70/30 |
|
Type of stroke (ischaemic/haemorrhagic) |
18/12 |
60/40 |
|
Side of hemiplegia (left/right) |
11/19 |
36.7/63.3 |
|
Number of stroke attacks (once/twice) |
29/1 |
96.7/3.3 |
|
Mobility status (unaided/stick/quadripod) |
19/8/3 |
63.3/26.7/10 |
|
Ankle-foot-orthosis (yes/no) |
2/28 |
6.7/93.3 |
|
Number of falls within 1 year (0/1/2/3) |
25/3/1/1 |
83.3/10.0/3.3/3.3 |
|
|
Mean (SD) [range] |
|
|
Age (years) |
61.23 (6.65) [50–73] |
|
|
Body weight (kg) |
66.63 (11.48) [48.3–98.3] |
|
|
Height (m) |
1.63 (0.07) [1.48–1.79] |
|
|
BMI (kg/m2) |
25.10 (3.17) [19.35–32.84] |
|
|
Duration of stroke (years) |
10.09 (4.66) [4.67–23.00] |
|
|
BMI: body mass index; SD: standard deviation. |
||
The study was approved by the ethics committee of the local institution and conducted according to the Declaration of Helsinki for human experiments. Clear explanation was given and written consent was obtained from all of the participants before the assessment.
Outcome measures
Comfortable and maximum walking speeds in the 5mWT and 10mWT were measured. They were conducted in a corridor over a walkway marked with coloured lines at 2 ends according to conditions with different acceleration and deceleration distances (0, 1, 2 and 3 m). There were 16 conditions in total; 8 for comfortable walking speed and 8 for maximum walking speed (Table II). The participants were timed walking along the 5 m and 10 m walkway length using a digital stopwatch. The standardized instructions “walk at your most comfortable speed” and “walk as quickly and safely as you can” were given for comfortable walking and maximum walking speeds, respectively.
|
Table II. Conditions with different combinations of walk test (5mWT and 10mWT) and acceleration and deceleration distances (0, 1, 2 and 3 m) |
|||||
|
Walk test |
Walking strategy |
Acceleration and deceleration distance |
|||
|
0 m |
1 m |
2 m |
3 m |
||
|
5mWT |
Comfortable speed |
COND 1 |
COND 3 |
COND 5 |
COND 7 |
|
|
Maximum speed |
COND 2 |
COND 4 |
COND 6 |
COND 8 |
|
10mWT |
Comfortable speed |
COND 9 |
COND 11 |
COND 13 |
COND 15 |
|
|
Maximum speed |
COND 10 |
COND 12 |
COND 14 |
COND 16 |
|
COND: condition; 5mWT: 5-m walk test; 10mWT: 10-m walk test. |
|||||
Each participant completed 16 conditions, for which the sequence was randomized by drawing lots. They were required to complete 3 trials for each condition. At least 30 s of rest was given between trials to avoid fatigue. Mean speed (m/s) was calculated by averaging the speed in the 3 trials.
Statistical analysis
Table I shows the descriptive statistics of the demographic characteristics of our participants. The effect of acceleration and deceleration distance on walking speed was analysed by one-way repeated measures analysis of variance (ANOVA). The acceleration and deceleration distances were the only factors with 4 levels (0, 1, 2 and 3 m). Walking speed was measured repeatedly and the mean walking speed was used for statistical analysis. The analysis was conducted via the Statistical Package for the Social Sciences (SPSS) software. The level of statistical significance is set at α = 0.05. A post-hoc paired t-test with the Bonferroni correction was run if a statistical significance is shown in the one-way repeated measures ANOVA, with p-value < 0.0083 sconsidered as statistically significant. Correlations between walking speed and factors including age, duration of stroke, number of stroke and number of falls were examined by Pearson’s r.
RESULTS
Both comfortable and maximum walking speeds of both the 5mWT and the 10wMT were summarized in Table III.
|
Table III. Comfortable and maximum walking speed measured in 5mWT and 10mWT with 0, 1, 2 and 3 m acceleration and deceleration distances |
|||||||
|
Walk test |
Walking speed, m/s |
pa |
|||||
|
Walking strategy |
0 m Mean (SD) |
1 m Mean (SD) |
2 m Mean (SD) |
3 m Mean (SD) |
Overall Mean (SD) |
||
|
5mWT |
Comfortable speed |
0.69 (0.17) |
0.73 (0.18) |
0.74 (0.20) |
0.74 (0.18) |
0.73 (0.18) |
0.001* |
|
Maximum speed |
0.91 (0.28) |
0.93 (0.27 |
0.92 (0.26) |
0.94 (0.28) |
0.93 (0.27) |
0.122 |
|
|
10mWT |
Comfortable speed |
0.75 (0.19) |
0.76 (0.20) |
0.76 (0.18) |
0.78 (0.20) |
0.76 (0.19) |
0.225 |
|
Maximum speed |
0.93 (0.28) |
0.96 (0.30) |
0.96 (0.30) |
0.96 (0.30) |
0.95 (0.29) |
0.052 |
|
|
aEffect of acceleration and deceleration distance with each walking strategy was analysed using one-way repeated analysis of variance (ANOVA). *Statistically significant difference in mean walking speed among 4 conditions with 0, 1, 2 and 3 m acceleration and deceleration distances. 5mWT: 5-m walk test; 10mWT: 10-m walk test; SD: standard deviation. |
|||||||
5mWT
One-way repeated measures ANOVA showed a significant difference in the comfortable walking speed among the 4 conditions with 0, 1, 2 and 3 m acceleration and deceleration distances (p = 0.001). A post-hoc paired t-test with the Bonferroni correction was run, with p-value < 0.0083 considered as statistically significant. The post-hoc result indicated that the comfortable walking speed with 0 m acceleration and deceleration distance was significantly different from that with 1, 2 and 3 m acceleration and deceleration distances (p < 0.0083), while there was no significant difference in the comfortable walking speed among 1, 2 and 3 m acceleration and deceleration distances (Fig. 1). At the maximum walking speed, there was no significant difference among the 4 conditions.
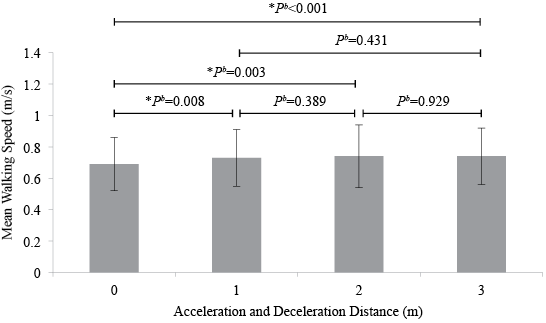
Fig 1. Mean comfortable walking speed measured in 5mWT with 0, 1, 2 and 3 m acceleration and deceleration distances. Pb; P value of post-hoc analysis. *Statistically significant difference in mean comfortable walking speed between two groups (p < 0.0083).
10mWT
No significant difference in the comfortable or maximum walking speeds was shown among the 4 conditions with 0, 1, 2 and 3 m acceleration and deceleration distances.
DISCUSSION
This is the first study to systematically investigate the effect of acceleration and deceleration distance on walking speed in people with chronic stroke.
Walking performance in people with stroke
Comfortable walking speed is intended to reflect the way people walk comfortably and naturally most of the time (4). The maximum walking speed reflects the ability of people to manage daily tasks requiring fast walking speed, such as crossing the road (5, 7). In the 5mWT, the comfortable walking speed of our participants was 0.73 m/s, whereas the maximum walking speed was 0.93 m/s. In the 10mWT, their comfortable walking speed was 0.78 m/s, whereas the maximum walking speed was 0.95 m/s.
Compared with previous studies on the walking speed in people with stroke, our results in both comfortable and maximum walking speeds in the 5mWT were consistent with Ng et al.’s study (comfortable walking speed = 0.76 m/s, maximum walking speed = 0.99 m/s) (4). In our 10mWT, a consistent comfortable walking speed (0.79–0.94 m/s) and a comparable maximum walking speed (1.00–1.4 m/s) were also shown (2, 4, 12). According to the study of Taylor-Piliae and colleagues (19), the comfortable walking speed of our participants in the 10mWT was considered as limited community walker (0.4–0.8 m/s), meaning they can be independent in at least one moderate community activity, such as having meal in restaurant, but cannot walk in crowds or on uneven terrains (11).
The slightly slower walking speed among our participants compared with people with stroke in previous studies (5, 20, 21) can probably be explained by their demographic characteristics. First, the mean age of our participants is 61.23 years, which is higher than previous studies (2, 4, 12). Secondly, 70% of our participants are males and it is less than those in previous studies (2, 4, 12). Since males are more able to produce rapid lower extremity muscle torques than females, they are known to have faster comfortable and maximum walking speeds (20).
Compared with the walking speed of older adults without stroke from past studies, our participants had a slower comfortable and maximum walking speeds (5, 7). Among older adults without stroke, the comfortable and maximum walking speeds were 1.22 and 1.79 m/s, respectively, in the 5mWT (7), while the comfortable and maximum walking speeds ranged from 1.07 to 1.43 m/s and 1.66 to 1.94 m/s, respectively, in the 10mWT (5, 7).
As for the ability to increase to the maximum walking speed beyond comfortable walking speed, our participants could increase their walking speed by 25.0–27.4%, which is consistent with that reported by Dobkin and colleagues (22). It had been reported that people with chronic stroke who were independent walkers and over 60 years of age can only increase their walking speed by approximately 25%, while older adults without stroke can increase their walking speed by 25–50% (22).
Stroke-specific impairments significantly affect the walking speed in people with stroke (5, 20, 21). Spasticity, deficits in sensation and perception, and muscle weakness are all common characteristics of stroke (21). Altered motor neuron pool activation and recruitment patterns, reduced motor unit discharge rate (23), slow modulation of firing rates (24) and gross atrophy (25) all contribute to the deficits in muscle strength and control in people with stroke (23). Indeed, muscle weakness over the lower extremities is associated with a slower walking speed (10).
Effect of acceleration and deceleration distance
In this study, the only significant effect was found at comfortable walking speed in the 5mWT. The comfortable walking speed in the 5mWT with 0 m acceleration and deceleration distance was significantly slower than that with 1, 2 or 3 m acceleration and deceleration distances. People with stroke apparently require a certain distance to reach a steady, comfortable walking speed and to terminate their walking. They may start the walk slowly to lower the fall risk by reducing the acceleration of the upper body (3). Without acceleration and deceleration distance, the walking speed measured tends to be an average one instead of a steady one.
Macfarlane & Looney’s study (17) on older adults without walking impairment, found that a mean of 2.17 m acceleration distance and 1.80 m deceleration distance was required to reach a steady comfortable walking speed over a 15-m walkway. Yet, the acceleration and deceleration distance required may be shorter for people with stroke, as they may adopt a different walking strategy. Based on our results, therefore, 1 m acceleration and deceleration distance is suggested to be sufficient for people with stroke for reaching their steady, comfortable speed in the 5mWT.
No significant difference was found at comfortable walking speed in 10mWT with different acceleration and deceleration distances (0, 1, 2 and 3 m). It implies that no acceleration and deceleration distance is needed when assessing comfortable walking speed in the 10mWT. Ng et al. (4) compared comfortable walking speed in the 5mWT and 10mWT in people with stroke, both with 2 m acceleration and deceleration distance. The results showed that there was no significant difference in the walking speed. Combining with our results, it appears that there is only a significant change at the comfortable walking speed when the total walkway length is between 5 (0+5+0) m and 7 (1+5+1) m. One of the possible reasons is that when the total walkway length exceeds 7 m, the effect of acceleration and deceleration distance on walking speed is diminished and its effect becomes insignificant.
Apart from the effect of acceleration and deceleration distance, the significant difference in the walking speed may be due to the change in walking strategy. It has been reported that older adults without stroke adopt different walking strategies depending on the walkway length (26). A long walkway length (> 20 m) elicits a higher stride velocity and a shorter gait cycle, compared with a shorter walkway length (< 10 m) in healthy older adults (26). Whether people with stroke adopt similar strategy as older adults is unknown. However, it should be noted that the definition of both “long” and “short” walkways would probably be shorter to people with stroke, because of their compromised walking endurance (27).
It is surprising to note that no significant difference was found in maximum walking speed in either 5mWT or 10mWT, with any acceleration and deceleration distance (0, 1, 2 and 3 m). It implies that no acceleration or deceleration distance is needed when measuring the maximum walking speed in 5mWT or 10mWT. A potential explanation is that participants were instructed to walk as quickly and safely as they could before the assessment as standardized instruction. Acceleration and deceleration, therefore, took place in a much more rapid manner, compared with when walking at the comfortable speed. It has been reported that acceleration and deceleration distance in maximum walking is shorter than that in comfortable walking (17). The effect of acceleration and deceleration, which is further diminished at maximum walking speed, becomes insignificant.
Study limitations
Several limitations were noted in this study. This study focused only on walking speed and therefore, gait quality was not observed. Further studies could be conducted to investigate the effect of acceleration and deceleration distance with other gait parameters, such as step length, cadence and gait pattern. In addition, the sample size (n = 30) of this study might be too small to detect any significant effect in all conditions. Also, our participants were community dwelling people with chronic stroke. Thus, our results could only be generalized to people with stroke who fulfil similar inclusion criteria. Further studies are required to investigate the effect of acceleration and deceleration distance on walking speed of people with acute or subacute stroke who have poorer walking capacities.
Our results could only be applied to similar environments either, i.e. indoor with a flat surface and no obstacles. There might be a different result when the study is done in an outdoor environment. The walking speed of participants might be affected as the investigator had to walk behind them closely during the test to ensure safety. There might also be learning and fatigue effects, since participants were required to walk in all 16 conditions with 3 trials each. In order to minimize the learning and fatigue effect, the testing sequence was randomized and at least 30 s of resting was allowed.
The study was designed to identify any effect of acceleration and deceleration distance on walking speed in the 5mWT and 10mWT. Thus, the optimal acceleration and deceleration distance required was not found. Only 0, 1, 2 and 3 m acceleration and deceleration distances were adopted in our study. The effect of acceleration and deceleration distance was only significant at comfortable walking speed in the 5mWT between 0 m and 1 m acceleration and deceleration distance, which means that the optimal acceleration and deceleration distance could be within this range. Further studies are needed to identify the optimal acceleration and deceleration distance required for measuring the comfortable walking speed in the 5mWT in people with stroke.
We also assumed that the same acceleration and deceleration distance were required. However, people with stroke may need different combinations of acceleration and deceleration distance in reaching their steady walking speed. Hence, different combinations of acceleration and deceleration distance in further study can delineate the exact distance required in the 5mWT.
Conclusion
This is the first study to examine the effect of acceleration and deceleration distance on the comfortable and maximum walking speeds in the 5mWT and 10mWT in people with chronic stroke. Based on our results, in people with stroke, the 5mWT with maximum walking speed and 10mWT with comfortable or maximum walking speeds do not require any additional distance for acceleration and deceleration. On the other hand, the 5mWT with comfortable walking speed requires at least 1 m for acceleration and deceleration. This poses a significant impact on current practice, as a shorter walkway can minimize potential fatigue in people with stroke and it is also beneficial to clinical settings with limited space.
ACKNOWLEDGEMENT
This study was supported by General Research Grant 562413 from Hong Kong’s Research Grants Council to Dr Shamay S. Ng and her team.
REFERENCES

