Stefan Salminger, MD1,2, Aidan D. Roche, PhD2,5, Agnes Sturma, MSc2,4, Laura A. Hruby, MD2,3 and Oskar C. Aszmann, PhD1,2
From the 1Division of Plastic and Reconstructive Surgery, 2Christian Doppler Laboratory for Restoration of Extremity Function, 3Department of Physical Medicine and Rehabilitation, Medical University of Vienna, 4University of Applied Sciences FH Campus Wien, Vienna, Austria and 5Department of Plastic Surgery, Southmead Hospital, North Bristol NHS Trust, UK
OBJECTIVE: In patients with severe bilateral congenital arm deficiencies, even simple activities of daily living, such as feeding, may be major challenges. We report here a case of a patient with arthrogryposis multiplex congenita affecting all 4 extremities, who underwent prosthetic replacement after elective transhumeral amputation of his right functionless arm.
CASE REPORT: A 22-year-old man with arthrogryposis multiplex congenita had severe deficits of his upper limbs. Previous surgeries for upper and lower limbs had enabled this patient to walk without aids; however, his upper limbs remained severely impaired. After prosthetic rehabilitation, including nerve and muscle transfers, a carefully planned elective amputation, signal processing and a comprehensive rehabilitation programme, the patient was able to independently conduct normal activities of daily living that had hitherto been impossible. The Disabilities of the Arm, Shoulder and Hand measure improved from 73.3 to 44.2, the Action Research Arm Test improved from 10 to 18 out of 57 points and the Southampton Hand Assessment Procedure improved from 8 to 23 after prosthetic replacement.
CONCLUSION: Prosthetic replacement can improve upper limb function in patients with severe congenital limb deficiencies. In the case reported here, functional rehabilitation had a positive impact on the patient’s quality of life and self-confidence, as he integrated the prosthesis into his body image.
Key words: arthrogryposis multiplex congenita; amputation; prosthetic replacement; functional outcome.
J Rehabil Med 2016; 48: 725–728
Correspondence address: Oskar C. Aszmann, Division of Plastic and Reconstructive Surgery, Department of Surgery, Medical University of Vienna, Währinger Gürtel 18–20, AT-1090 Vienna, Austria. E-mail: oskar.aszmann@meduniwien.ac.at
Accepted Jun 1, 2016; Epub ahead of print Aug 18, 2016
INTRODUCTION
Arthrogryposis multiplex congenita (AMC) represents a rare condition of 1 in 3000–4000 births. Diminution in size and degeneration of the anterior horn cells in the spinal cord result in contractures usually affecting all limbs at birth, induced by a combination of decreased foetal movements, increase in connective tissue, muscle atrophy and abnormal joint surfaces (1–3). This leads to a condition characterized by multiple joint contractures of both upper and lower limbs at birth. Different conservative and surgical concepts for the rehabilitation of such deficits have been introduced, although with poor outcomes in some severe cases.
We report here a patient who experienced continuing very severe upper limb deficiencies after extensive rehabilitation and multiple surgical procedures both for his upper and lower limbs.
CASE REPORT
A 22-year-old man with AMC underwent prosthetic replacement after elective amputation of his right functionless arm. Previous surgeries for both upper and lower limbs enabled the patient to walk without aids; however, his upper limbs remained severely impaired. The patient was able to perform mass-movements emanating from the thoracoscapular joint with limited function of the shoulder girdle muscles. However, there was neither active nor passive range of motion in the shoulder and elbow joints. As is typical for AMC, the patient had internal rotation contractures of the shoulder joint, flexion and extension deformities of the elbow joint, thumb-in-palm deformity and ulnar deviation of the wrist (4) (Fig. 1). Even after bilateral wrist arthrodeses, the hands remained deviated in 45° of flexion. His right index finger revealed flicker movements (M2 according to the Medical Research Council (MRC) scale), but no useful muscle activity of his entire right arm. His left hand also showed dismal function, with minimal ability of pinching (M3) objects between the thumb and index finger, which provided the patient limited assistance in some activities of daily living (ADL) (Video 11). This necessitated 24-h care from his parents with assistance for the most essential tasks.

The success of prosthetic limb replacement has been demonstrated recently in patients with functionless hands after brachial plexus injuries. However, it has not yet been applied in patients with congenital extremity defects, as demonstrated in this case (5).
METHODS
Clinical evaluation
The patient provided written informed consent to take part in this study. Initial suitability was assessed in the specialist upper limb clinic including neurological and musculoskeletal examination of upper limb function. Prosthetic replacement will only be applicable in patients with a very severe manifestation of arthrogryposis resulting in a functionless hand and arm beyond any biological reconstructive techniques to improve remaining function. Furthermore, hybrid arm fitting demonstrates the prospective benefit to both physicians and the patient and thus supports decision-making. Psychological evaluation (structured clinical interview and Freiburger assessment to assess adequate coping strategies) was performed by a qualified psychologist both before and after intervention.
Identification/establishment of electromyography (EMG) signals for prosthetic control
Myoelectric prosthetic arm replacement necessitates at least 2 cognitively separate electromyography (EMG) signals. As described above, no useful movement could be identified in the right hand, despite the fact that some intrinsic muscle function could be detected. Hypothesizing the presence of motor fibres in the ulnar and median nerve, new functional muscle tissue was transplanted using a combined gracilis and adductor longus muscle transplant with 1 arterial pedicle, but 2 separate nerve branches. As the elbow joint was non-functional, the muscles were transplanted into the upper arm with the plan of creating intuitive intrinsic muscle activity to control a myoelectric upper arm prosthesis. The motor branch of the adductor longus was coapted to the median and ulnar nerve and the motor branch of the gracilis muscle to the radial nerve. Although both muscles showed perfect vascularization on ultrasound investigation, they did not show signs of voluntary control and were unable to produce any surface or needle EMG signal, even when measured 2 years after surgical intervention. However, as a consequence of described nerve transfers, the patient only showed protective sensation of his right arm, with a static 2-point discrimination of more than 8 mm. As the creation of new muscle activity was not successful in this patient, other potential EMG sites were investigated for prosthetic control. An EMG matrix over the shoulder revealed faint signals in the pectoralis major and latissimus dorsi muscles. Hence, these 2 muscle signals were trained for further prosthetic rehabilitation.
Rehabilitation programme
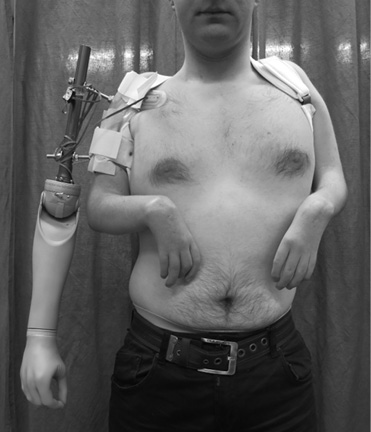
Once the appropriate surface-EMG (sEMG) sites were determined, cognitive training was initiated via rehabilitation using visual feedback. As the patient had been unable to control hand or arm movements since birth, cognitive control was very poor and motor learning had to be supported in multiple sEMG feedback sessions. To allow the patient to gain control over the amount of muscular activity needed and the selective activation of the muscles, visualization with online EMG recordings was used in the beginning (6). In addition, short and strong co-contractions of the 2 muscles were trained to switch between the different prosthetic joints of the myoelectric arm. As soon as the patient showed adequate control, the PAULA Software (Otto Bock Health Care Products GmbH, Vienna, Austria) was used to control a virtual prosthesis. The use of virtual rehabilitation encouraged the patient by demonstrating his ability to control meaningful hand and arm movements with his myosignals, while the non-functioning arm was still in place. As a next step, a real prosthesis was mounted on a desk (“table-top prosthesis”) and controlled by the patient’s sEMG signals. Finally, he was fitted with a “hybrid arm”, whereby a prosthetic arm was attached to a splint-like device fixed to the remaining arm (Fig. 2). This setting provided direct proof for the patient that arm/hand function could indeed be achieved by prosthetic replacement. The described rehabilitation protocol prior to amputation was performed within 2 weeks of intense training (2–4 h/day). An experienced physical therapist guided the whole process.
Amputation for prosthetic fitting
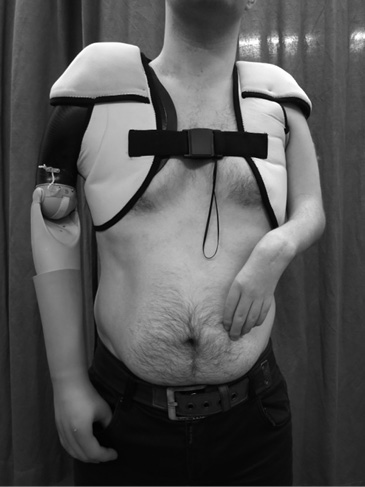
To achieve maximum independence and allow the patient to mount the prosthesis himself, a short transhumeral amputation of his right arm was performed. He was then fitted with a shoulder/arm socket and a conventional myoelectric prosthetic arm (Fig. 3). Early after amputation a compressive garment was applied for oedema control. Prosthetic training and fitting then could be performed as early as 6 weeks post-amputation.
Outcome assessment
Global upper extremity function was evaluated both pre- and post-interventional with the Action Research Arm Test (ARAT), Southampton Hand Assessment Procedure (SHAP) and the Disabilities of the Arm, Shoulder and Hand measure (DASH) questionnaire, which monitor hand and upper extremity function closely related to ADL. The ARAT is an observational test and consists of 4 sections with different tasks and a maximum of 57 points (7). The SHAP is a clinically validated hand function test originally developed to assess the effectiveness of upper-limb prostheses, and has also been applied for the assessment of musculoskeletal and neurological conditions (8). It is made up of 8 abstract objects and 14 activities close to daily life, with each task timed by the participants themselves. Normal hand function is regarded as 100 points (8). Quality of life was measured with the Short Form 36 (SF-36) Health Survey (English Version, 4-week recall) and the short-form World Health Organization Quality of Life (WHOQOL-BREF) questionnaire (English Version). While the SF-36 contains 36 items that are scored in 1 of 8 domains, the WHOQOL-BREF contains 26 items with 4 domains; namely: physical health, psychological, social relationships and environment.
RESULTS
Pre-interventional testing revealed dismal hand function (Video 11). Post-interventional testing took place 12 months after prosthetic fitting. Functional outcomes are demonstrated in Video 11. The DASH score improved from 73.3 to 44.2. The ARAT score improved from 10 to 18 out of 57 points and the SHAP score improved from 8 to 23. The patient is wearing his prosthesis for up to 16 h a day. Due to the uncomfortable nature of the hybrid fitting, the additional weight and the socket impairing the vascular supply of the remaining arm, functional evaluation with the hybrid hand could not be completed. Only a few tasks could be performed (Video 11).
The SF-36 revealed a physical component sum scale of 57.6 before and 44.9 after prosthetic replacement. The mental component sum scale increased from 39.9 to 62.2. The detailed 8-item profile of functional health and well-being scores are demonstrated in Table I. The patient showed improved scores in the scales “physical functioning”, “bodily pain”, “general health perception”, “emotional and social role functioning” and “mental health”. As shown in Table II, the WHOQOL-BREF domain “physical health” also improved, from 38 to 63 (in the 100-point transformed scale). No phantom limb or neuroma pain occurred within the first 24 months after amputation.
|
Table I. Quality of life Assessment (Short-Form 36; SF-36), 8-item profile pre and post-prosthetic fitting |
||
|
|
Pre- |
Post- |
|
Physical functioning |
65 |
80 |
|
Physical role functioning |
100 |
25 |
|
Bodily pain |
100 |
80 |
|
General health |
77 |
100 |
|
Vitality |
80 |
80 |
|
Social role functioning |
75 |
100 |
|
Emotional role functioning |
33.3 |
100 |
|
Mental health |
56 |
88 |
|
Physical component summary scale |
57.6 |
44.9 |
|
Mental component summary scale |
39.9 |
62.2 |
|
Table II. Quality of Life Assessment with short-form World Health Organization Quality of Life (WHOQOL-BREF) questionnaire (transformed scores from 0 to 100; with 100 as the best outcome) before and after prosthetic fitting |
||
|
|
Pre- |
Post- |
|
Physical health |
38 |
63 |
|
Psychological |
69 |
63 |
|
Social relationships |
69 |
69 |
|
Environment |
63 |
75 |
DISCUSSION
AMC represents a severely disabling disorder, resulting in a lack of independence in daily routine. The patient presented here was unable to feed himself or to manage simple tasks of daily life. Latissimus dorsi transfers, bilateral wrist arthrodesis, different joint arthrolysis, as well as extensive rehabilitation regarding his upper limbs were performed elsewhere, but did not result in useful hand and arm function for this patient. Elective amputation and replacement with a prosthesis enabled the patient to carry out simple, but essential, ADL, such as feeding himself, opening a bottle of water, or carrying household objects, thus allowing a certain degree of independence and improved quality of life.
For myoelectic prosthesis control to be successful, usable EMG signals must be available. The primary goal of the initial surgery was to create intuitive EMG signals by using free functioning muscle transplants coapted to median, ulnar and radial nerves hypothesizing that fresh muscle could provide more useful EMG signals at a more proximal level. However, this was not successful, although both transplanted muscles showed perfect vascular supply in ultrasound investigations 3 months after surgery. Abnormalities in motor-neuronal development in arthrogryposis may explain this failure (1, 3). Using the faint EMG activity of the latissimus dorsi and pectoralis major muscles to control the prosthetic device was difficult at the beginning; however, as time progressed and rehabilitation training increased, the patient was able to control these muscles more naturally.
As has been learnt from targeted muscle reinnervation (TMR) in high level amputees, the more neuromuscular units that can be established, the better the prosthetic control (9). Due to the nature of this disease, creation of additional myoelectric sites was not possible. Although prosthetic fitting in transhumeral amputees is challenging and results in high rates of abandonment, prosthetic replacement in this patient resulted in relevant improvements of hand and arm function as well as quality of life. Even though only 2 myosignals were available to control a 3-degree of freedom myoelectric arm, an appropriate algorithm was installed to change between the different prosthetic joints.
The use of virtual rehabilitation and biofeedback systems in combination with the hybrid arm fitting represents a key part in the concept of the rehabilitation process. After hybrid fitting, the benefits and limitations of the prosthesis were clear to the patient and his entire family. Still, an amputation represents an irreversible step that has to be made with careful consideration. Prosthetic fitting also showed beneficial influence with regards to self-confident appearance, as the prosthetic arm is in a more natural position and the patient regained enjoyment of human interaction and social activities, as reflected by the improvement in sub-item scales emotional and social role functioning in the SF-36 (Fig. 4). After having lived with no hand and arm function from birth and consequent dependence on his environment, the patient learnt to feed himself at the age of 22 years after final prosthetic fitting.

Upper-extremity deformities in AMC show great variation, and therefore treatment strategies must be considered carefully and individually. The presented concept of prosthetic replacement will be applicable in patients with a severe manifestation of congenital defects leading to a functionless hand and arm. In such cases, prosthetic replacement can improve hand and arm function to provide independent upper-extremity function to allow ADL, such as self-feeding and best-possible quality of life. Although the prosthesis has greater range of motion and strength, the remaining left hand and arm of this patient is of major importance for manipulating small objects and touchpad-dependent technology. This task distribution allows the patient to handle heavy objects with his prosthetic arm and small object manipulation with his left arm, reflecting a sense of diverse dexterity observed also in many other biologic scenarios (10).
Some patients with AMC are wheelchair users and it is possible that the prosthetic arm could be mounted on the wheelchair instead of directly to the body. With improvements in wireless signal transduction technologies it may become possible to implant myoelectric sensors for exo-prosthetic control without the need for amputation (11, 12).
As shown in this case, prosthetic replacement of an upper limb can establish useful hand and arm function in patients with severe congenital limb deficiencies. Here, prosthetic replacement not only achieves motor function, but also has a positive influence on quality of life as a result of achieved independence (5).
ACKNOWLEDGEMENTS
This study was funded by the Christian Doppler Research Foundation of the Austrian Council for Research and Technology Development and the Austrian Federal Ministry of Science, Research & Economy. The authors acknowledge the time and effort provided by the patient and his family. The authors also thank Professor Eugenijus Kaniusas for his assistance with, and dedication to, this project.

1http://www.medicaljournals.se/jrm/content/?doi=10.2340/16501977-2123
REFERENCES


