Mohammadreza Shahbazi, PhD1, Mahshid Foroughan, MD2, Mahdi Rahgozar, PhD3 and Reza Salman Roghani, MD4
From the 1Aging Department, 2Iranian Research Center on Aging, Aging Department, 3Biostatistics Department and 4Clinical Science Department, University of Social Welfare and Rehabilitation Sciences, Tehran, Iran
OBJECTIVE: To assess the effects of a rehabilitation service package designed by the State Welfare Organization of Iran for adult day care centres on the disability of older clients.
METHODS: A case-control study, with 46 older participants in the case group and 46 participants, matched for level of disability, in a control group. The World Health Organization Disability Assessment Schedule 2 was used to collect data at 4 time-points: baseline and 2, 4, and 6 months later. Data were analysed using repeated-measures analysis of variation.
RESULTS: The rehabilitation service package had significant effects on the disability scores of older users of day care services. The disability scores significantly changed within the subjects (p = 0.010) and between the 2 groups (p < 0.001). Within-subjects effects in all 6 domains (“understanding and communication” (p = 0.002), “getting around” (p = 0.046), “self-care” (p < 0.001), “getting along with people” (p < 0.001), “life activity” (p < 0.001) and “participation” (p < 0.001)) and between-subjects effects, in all except the “self-care” domain, showed significant differences during the 6-month study period (p = 0.003, p < 0.001, p <0.001, p < 0.001, and p < 0.001, respectively).
CONCLUSION: The adult day care service package may have a positive role in decreasing measures of disability among older persons over a 6-month period.
Key words: ageing; day care; disability evaluation; World Health Organization.
J Rehabil Med 2016; 48: 00–00
Correspondence address: Mahshid Foroughan, Koodakyar St, Velanjak St, Iranian Research Center on Aging, University of Social Welfare & Rehabilitation Sciences, Tehran, Iran. E-mail: m_foroughan@yahoo.com
Accepted Apr 21, 2016; Epub ahead of print Aug 5, 2016
INTRODUCTION
The functional status declines and the risk of being affected by diseases, particularly chronic diseases, increases with age (1, 2). The probability of disability also increases with age (2). Disability typically results in lower life satisfaction and lower quality of life (3–5); it also increases the cost of healthcare and risk of hospitalization, institutionalization, and placement in a nursing home (6–8). According to the International Classification of Functioning, Disability and Health (ICF), “disability” is a multidimensional issue used as an umbrella term for impairment, activity limitations, and participation restrictions (9).
Adult day centres, as their mission dictates, provide: medical, rehabilitation, educational, social, and/or recreational services for older individuals during the daytime. Their aims include: promoting older adults’ participation in society and in group activities, delaying their nursing home placement, decreasing or preventing disability, reducing their feeling of loneliness, and supporting their families.
Research investigating the effects of adult day services on disability, functioning, and frailty of older adults, delayed nursing home placement, and reduction in caregivers’ burden has had varying results, which sometimes conflict. Some studies have demonstrated the positive effects of day care services on quality of life, well-being, mood, and behavioural problems among older individuals (10, 11). Others have reported that it is difficult to demonstrate the benefits of day care services, and have recommended further research (12, 13). Also, studies into the effects of adult day care services on delaying nursing home placement have not revealed any significant effects (14, 15), and one study even found that the risk of nursing home placement increased significantly with the number of days of adult day care attendance (16). In contrast, all studies, except for one (17), assessing the effects of adult day care on caregivers’ burden reported lower levels of overload, depression, anger, and caregiving-related stress (18–21).
Adult day care centres are a new concept in Iran and have mostly been established during the last decade. They work under the direction and supervision of the State Welfare Organization (SWO) of Iran, and their costs are covered by the SWO. There are more than 63 centres providing services for 3500 older individuals across Iran. Recently, the SWO has prepared a service package for empowerment of older adults, including medico-rehabilitative and psycho-social services, based on bio-psychosocial model. It is a comprehensive, as well as flexible and adjustable, package, which considers the needs and interests of the consumers during service delivery. All day care centres in Iran are required to deliver their services according to this package.
The recent establishment of day care services and programmes in Iran and the huge cost this entails, together with the contradictory results in the international literature, prompted us to question the effects of the SWO service package for adult day care on disability and disability trends in older individuals. The main objective of this research was therefore to assess the effects of the SWO service package on the disability of older clients of day care centres in Iran.
MATERIAL AND METHODS
This was a case-control study. The research took place in the Kahrizk adult day centre, which is the only one in Alborz Province. After a public announcement, 46 individuals ≥ 60 years of age volunteered to participate in the study. The aims of the study were described and written consent obtained from each participant. The study was approved by the ethics committee of the University of Social Welfare and Rehabilitation Sciences in accordance with the ethics standards set out in the 1964 Declaration of Helsinki and its later amendments or comparable ethics standards (Ethics Committee Approval Number: USWR.REC.1392.109). The World Health Organization Disability Assessment Scale (WHODAS II) 36-item questionnaire was implemented and the participants’ functional levels were determined. To select the control group, the participants were interviewed and asked to introduce 2 or 3 of their acquaintances whom they thought had similar functional levels to themselves. These individuals were also assessed with the WHODAS II 36-item questionnaire, and the person who gained the score closest to that of the participant was entered into the control group. This selection method enabled us to recruit a control group as socio-economically similar as possible to the case group. The control group was told that they could receive the same services free of charge at the end of the study, if they wished. Exclusion criteria included: severe changes in the participants’ health status due to acute conditions, accidents, or acute life stresses. For the case group, a further exclusion criterion was absence > 30 days.
The WHODAS II 36-item questionnaire assesses disability in 6 domains: “understanding and communication”, “getting around”, “self-care”, “getting along with people”, “life activities” and “participation”. The appropriate psychometric properties of WHODAS II has been shown previously (Cronbach’s alpha = 0.86, intra-class correlation coefficient (ICC) = 0.98) (22). It has been translated and validated in Iranian older adults (Cronbach’s alpha=0.86 and ICC=0.47)1.

1Arjmand M, Kamali M, Zeraati H. Assessing validity and reliability of WHODAS II Questionnaire in Iranian elderly. Tehran: University of Tehran, 2008.
Our assessments were taken at 4 time-points: at baseline, before delivering the service package began (Level 1); 2 months later (Level 2); 4 months later (Level 3); and 6 months later (Level 4).
All testers were trained by the research team before the research began. Those who assessed the case group were different from those who assessed the control group. The inter-rater reliability was tested at several points (ICC = 0.687, ICC = 0.631, ICC = 0.693) to lessen the impact of measurement errors on the results.
The comprehensive day care service package consisted of rehabilitation services including physiotherapy, occupational therapy, and speech therapy (as needed by the consumer and prescribed by the professionals); educational courses including social life skills, healthy lifestyle, and self-care training programmes; nutrition counselling; providing assistive devices (as needed); cognitive enhancement techniques; and psycho-social interventions, such as art therapy, individual and group therapy, and recreational activities (based on the need and/or preference of the consumer). These services were available for all participants in the case group. The quality of services was monitored consistently by the researchers during the study. The control group did not receive any services, but registered as potential candidates for receiving them after the study period.
The members of the case group typically attended the centre from 08.00 h to 14.30 h. Transportation, a small meal at 10.30 h, and lunch at 12.30 h, were ready for them free of charge during the day. During the 6-month period of research, 6 cases of attrition occurred (5 in the case group and 1 in the control group); 2 individuals were absent for > 30 days, 1 moved, 2 dropped-out, and 1 died.
Informed consent was obtained from all individual participants included in the study.
Statistical analysis
SPSS version 16 was used to analyse the data. One sample Kolmogrov- Smirnov was used to test normal distribution of quantitative variables. χ2, independent t, and Mann-Whitney U tests were applied to compare sex, marital status, age, income and disability levels between the 2 groups at baseline; the data related to changes in the disability and its domains analysed by repeated-measure analysis of variance (ANOVA). When Mauchly’s test of sphericity was significant, Greenhous-Geisser epsilon was used to adjust the degrees of freedom. And if Box’s test of equality of covariance matrices was significant the Dunnett’s T3 test was used.
RESULTS
There were 92 participants in 2 groups of 46 (37 (40.2%) men and 55 (59.8%) women). The mean age of the participants was 68.53 (standard deviation (SD) 6.1) years (age range 60–85 years).There were no significant differences between the case and control groups at baseline in terms of age, sex, educational level, and other controlled socio-demographic variables (Table I).
|
Table I. Comparison of sex, marital status, education, age, income and World Health Organization Disability Assessment Scale (WHODAS II) disability scores between case and control groups at the start of the study |
||||||
|
|
Case n = 46 |
Control n = 46 |
Total |
Statistic |
p-value |
|
|
Sex, % (n) |
|
|
|
|
|
|
|
Men |
|
43.3 (19) |
39.1 (18) |
40.2 (37) |
0.045a |
0.832 |
|
Women |
|
58.7 (27) |
60.9 (28) |
59.8 (55) |
||
|
Marital status, % (n) |
|
|
|
|
|
|
|
Married |
|
63 (29) |
60.9 (28) |
62 (57) |
0.046a |
0.830 |
|
Single |
|
37 (17) |
39.1 (18) |
38 (35) |
||
|
Education, % (n) |
|
|
|
|
|
|
|
Illiterate |
|
54.3 (25) |
52.2 (24) |
53.3 (19) |
0.604a |
0.739 |
|
Reading and writing only |
|
26.1 (12) |
32.6 (15) |
29.3 (27) |
||
|
Elementary and more |
|
19.6 (9) |
15.2 (7) |
17.4 (16) |
||
|
Age, years, mean (SD) |
|
69.0 (6.1) |
68.0 (6.2) |
68.5 (6.1) |
0.800b |
0.426 |
|
Incomed, mean (SD) |
|
4.1 (4.4) |
3.2 (3.2) |
3.7 (3.9) |
910.500c |
0.317 |
|
WHODAS II disability scores, mean (SD) |
|
23.08 (12.16) |
21.98 (11.55) |
22.53 (11.81) |
0.433b |
0.659 |
|
aχ2; bt-test; cMann-Whitney U; dIranian currency; Rials (35000 R = 1 USD). |
||||||
At the beginning of study, the disability mean score was 22.6 (SD 11.2) in the case group and 22.0 (SD 11.5) in the control group. The highest disability mean scores among the 6 domains of disability were for “getting around” (35.5 (SD 20.8)) and “life activity” (33.5 (SD 22.7)). After 6 months, the disability mean scores decreased to 17.4 (SD 8.9) and 25.8 (SD 10.8), respectively. The most changes occurred in the domains “getting along with people” and “getting around” (Table II).
|
Table II. World Health Organization Disability Assessment Scale (WHODAS II) scores and its domains at 4 measured time-points (TP) in case and control groups |
|||||||||||||||
|
Domain |
Case |
|
Control |
||||||||||||
|
TP1 |
|
TP2 |
|
TP3 |
|
TP4 |
|
TP1 |
|
TP2 |
|
TP3 |
|
TP4 |
|
|
Mean (SD) |
|
Mean (SD) |
|
Mean (SD) |
|
Mean (SD) |
|
Mean (SD) |
|
Mean (SD) |
|
Mean (SD) |
|
Mean (SD) |
|
|
Understanding & communication |
20.3 (14.8) |
|
17.5 (11.9) |
|
15.8 (11.8) |
|
14.8 (11.7) |
|
20.3 (14.8) |
|
20.5 (13.2) |
|
19.9 (14.7) |
|
20.1 (13.6) |
|
Getting around |
35.5 (20.8) |
|
31.0 (18.9) |
|
28.9 (18.4) |
|
29.1 (17.0) |
|
30.9 (21.2) |
|
34.2 (20.8) |
|
38.3 (21.4) |
|
41.1 (19.6) |
|
Self-care |
7.3 (11.3) |
|
6.7 (11.5) |
|
5.3 (9.6) |
|
6.3 (10.2) |
|
13.6 (16.5) |
|
11.7 (14.4) |
|
10.7 (15.6) |
|
11.8 (15.5) |
|
Getting along |
12.5 (12.4) |
|
10.0 (10.5) |
|
10.9 (11.0) |
|
9.3 (8.8) |
|
13.0 (15.1) |
|
16.8 (15.3) |
|
22.4 (15.6) |
|
24.1 (13.8) |
|
Life activity |
33.5 (22.7) |
|
30.1 (21.6) |
|
25.5 (17.1) |
|
24.4 (15.5) |
|
26.6 (17.4) |
|
26.0 (17.1) |
|
28.5 (14.6) |
|
26.7 (15.0) |
|
Participation |
26.9 (16.1) |
|
22.0 (14.7) |
|
19.4 (12.5) |
|
19.8 (12.5) |
|
27.1 (16.3) |
|
26.1 (15.3) |
|
28.5 (15.7) |
|
30.4 (15.0) |
|
WHODAS II disability scores |
22.6 (11.2) |
|
19.3 (10.6) |
|
17.6 (9.3) |
|
17.4 (8.9) |
|
22.0 (11.5) |
|
22.6 (11.0) |
|
24.7 (11.1) |
|
25.8 (10.8) |
|
SD: standard deviation. |
|||||||||||||||
Repeated measures ANOVA showed that the disability scores within-subjects (p = 0.010) and between-subjects (p < 0.001) changed significantly during the study period, and there were significant interaction effects between disability scores and groups (p < 0.001) (Table III). Pairwise comparisons of disability mean scores at 4 time-points revealed significant differences in the case groups for all 3 pairs (p < 0.001) and in the second and third pairs in the control group (p < 0.001) (Table IV).
|
Table III. Repeated measure analysis of variation (ANOVA) results |
||||||
|
Domains |
Effect |
SS |
df |
MS |
F |
p-value |
|
Understanding & communication |
Time-point |
402.2 |
2.5 |
159.4 |
5.60 |
0.002 |
|
Group |
507.3 |
1 |
507.1 |
5.12 |
0.003 |
|
|
Time-point × Group |
318.7 |
2.5 |
126.3 |
5.25 |
0.001 |
|
|
Getting around |
Time-point |
300.7 |
3 |
102.9 |
2.29 |
0.046 |
|
Group |
1,538.7 |
1 |
1,538.7 |
32.33 |
< 0.001 |
|
|
Time-point × Group |
3,504.5 |
3 |
1,199.7 |
29.34 |
< 0.001 |
|
|
Self-care |
Time-point |
259.4 |
2.4 |
108.7 |
9.18 |
< 0.001 |
|
Group |
658.2 |
1 |
658.8 |
0.55 |
0.650 |
|
|
Time-point × Group |
20.1 |
2.4 |
8.4 |
0.34 |
0.753 |
|
|
Getting along |
Time-point |
1,117.0 |
3 |
403.1 |
11.94 |
< 0.001 |
|
Group |
1,513.7 |
1 |
1,513.7 |
24.21 |
< 0.001 |
|
|
Time-point × Group |
2,456.5 |
3 |
886.6 |
25.76 |
< 0.001 |
|
|
Life activity |
Time-point |
893.6 |
2.2 |
406.9 |
8.01 |
< 0.001 |
|
|
Group |
1,144.7 |
1 |
1,144.7 |
8.99 |
< 0.001 |
|
Time-point × Group |
1,497.4 |
2.2 |
681.8 |
13.02 |
< 0.001 |
|
|
Participation |
Time-point |
510.1 |
3 |
179.4 |
9.41 |
< 0.001 |
|
|
Group |
766.5 |
1 |
766.5 |
22.11 |
< 0.001 |
|
Time-point × Group |
1,435.0 |
3 |
504.7 |
26.92 |
< 0.001 |
|
|
WHODAS II disability scores |
Time-point |
91.2 |
3 |
31.3 |
4.01 |
0.010 |
|
|
Group |
1,144.9 |
1 |
1,144.9 |
36.74 |
< 0.001 |
|
Time-point × group |
1,074.9 |
3 |
368.5 |
43.83 |
< 0.001 |
|
|
SS: sum of squares; df: degree of freedom; MS: mean square. |
||||||
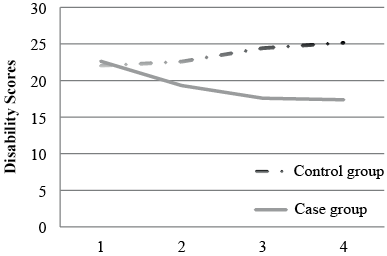
Fig. 1 shows the changes in disability scores in the case and control groups. Disability scores decreased in the case group and increased in the control group during the study period.
Within-subjects factor in 6 domains of disability revealed significant differences in: “understanding and communication” (p = 0.002), “getting around” (p = 0.046), “self-care” (p < 0.001), “getting along with people” (p < 0.001), “life activities” (p < 0.001) and “participation” (p < 0.001). In addition, disability scores between the subjects were significantly different in 5 out of 6 domains: “understanding and communication” (p = 0.003), “getting around” (p < 0.001), “getting along with people” (p < 0.001), “life activities” (p < 0.001) and “participation” (p < 0.001). No significant differences were observed in the “self-care” domain (Table III). In addition, there was significant interaction between disability scores and group in all domains, except the “self-care” domain, including “understanding and communication” (p = 0.001), “getting around” (p < 0.001), “getting along with people” (p < 0.001), “life activities” (p < 0.001) and “participation” (p < 0.001).
Pairwise comparison of level 1 with other levels in the case group indicated significant differences in all 3 pairs of “understanding and communication” (p = 0.004, p < 0.001, p < 0.001), “getting around” (p < 0.001, p < 0.001, p < 0.001), “getting along with people” (p = 0.008, p = 0.022, p = 0.001), “life activity” and “participation” domains (p < 0.001, p < 0.001, p < 0.001). No significant differences were found in the pairs of “self-care” domain. In addition, the comparison in the control group showed no significant differences in all 3 pairs of the “understanding and communication”, “self-care” and “life activity” domains, and in the first and second pairs of the “participation” domain (Table IV).
|
Table IV. Pairwise comparisons time-point 1 with other time-points in case and control groups |
||||||||
|
Domain |
Time-points |
Case |
|
Group |
||||
|
Mean differences |
SE |
p-value |
|
Mean differences |
SE |
p-value |
||
|
Understanding & communication |
TP1 vs TP2 |
2.751 |
0.905 |
0.004 |
|
–0.273 |
0.742 |
0.715 |
|
TP1 vs TP3 |
4.371 |
1.127 |
< 0.001 |
|
0.369 |
0.724 |
0.613 |
|
|
TP1 vs TP4 |
5.388 |
1.382 |
< 0.001 |
|
0.182 |
0.621 |
0.770 |
|
|
Getting around |
TP1 vs TP2 |
4.512 |
1.015 |
< 0.001 |
|
–3.333 |
1.376 |
0.020 |
|
TP1 vs TP3 |
6.585 |
1.412 |
< 0.001 |
|
–7.444 |
1.237 |
< 0.001 |
|
|
TP1 vs TP4 |
6.341 |
1.397 |
< 0.001 |
|
–10.222 |
1.156 |
< 0.001 |
|
|
Self-care |
TP1 vs TP2 |
0.607 |
0.608 |
0.327 |
|
1.942 |
1.087 |
0.081 |
|
TP1 vs TP3 |
1.380 |
0.554 |
0.086 |
|
1.913 |
0.834 |
0.060 |
|
|
TP1 vs TP4 |
1.063 |
0.687 |
0.130 |
|
1.802 |
1.184 |
0.135 |
|
|
Getting along |
TP1 vs TP2 |
2.439 |
0.875 |
0.008 |
|
–3.778 |
1.312 |
0.006 |
|
TP1 vs TP3 |
1.585 |
0.660 |
0.022 |
|
–9.333 |
1.316 |
< 0.001 |
|
|
TP1 vs TP4 |
3.171 |
0.920 |
0.001 |
|
–11.067 |
1.653 |
< 0.001 |
|
|
Life activity |
TP1 vs TP2 |
3.351 |
0.820 |
< 0.001 |
|
0.555 |
0.683 |
0.418 |
|
TP1 vs TP3 |
7.924 |
1.677 |
< 0.001 |
|
–1.944 |
1.189 |
0.109 |
|
|
TP1 vs TP4 |
8.993 |
1.977 |
< 0.001 |
|
–0.133 |
0.921 |
0.886 |
|
|
Participation |
TP1 vs TP2 |
4.929 |
0.858 |
< 0.001 |
|
0.962 |
0.898 |
0.290 |
|
TP1 vs TP3 |
7.444 |
1.192 |
< 0.001 |
|
–1.400 |
0.747 |
0.067 |
|
|
TP1 vs TP4 |
7.068 |
1.109 |
< 0.001 |
|
–3.273 |
0.708 |
< 0.001 |
|
|
WHODAS II disability scores |
TP1 vs TP2 |
3.300 |
0.623 |
<0.001 |
|
–0.580 |
0.550 |
0.297 |
|
TP1 vs TP3 |
4.981 |
0.730 |
< 0.001 |
|
–2.732 |
0.471 |
< 0.001 |
|
|
TP1 vs TP4 |
5.275 |
0.798 |
< 0.001 |
|
–3.800 |
0.553 |
< 0.001 |
|
|
TP: time-point; SE: standard error. |
||||||||
DISCUSSION
This study showed that the use of the SWO service package for adult day care during a 6-month period had significant effects and reduced consumers’ disability. Since the functions of the control group declined (disability scores increased) in the same time period, it can be concluded that the adult day services may not only be efficient in lowering disability, but may also prevent additional functional decline. It can also be suggested that continuing the programme may prevent increasing disability and may play a role in maintaining the functional level achieved.
Some studies assessing the effects of day care services have also shown positive effects or functional improvement in adult day care users (10, 11, 23, 24). However, contradictory results have also been reported. For example, Iecovich & Carmel (12) found no significant differences between users and non-users of day care centres in the level of loneliness, and showed that the attendance at day care centres, as well as length and frequency of use, had no significant association with the loneliness of users. On the other hand, Dabelko & Zimmerman (13) stressed that the psychosocial benefits of adult day services have been under-estimated, and Baumgatten et al. (17) concluded that it is difficult to objectively demonstrate the positive effects of day care interventions as perceived by clients, caregivers and staff.
Overall, the present study showed that the SWO rehabilitation service package for adult day care centres had prominent positive effects on the older persons’ disability scores in all domains, except the “self-care” domain.
In this study, the highest disability score of the 6 domains was observed in “getting around”. Previous studies have also shown similar results (4, 25–27). After a 6-month intervention, “getting around” was the most improved domain in the case group. Lowering the disability scores in this domain may be the result of the medical rehabilitation, including physical and occupational therapy, which may alleviate joint pain and improve muscle strength and balance. Meanwhile, the participants increased their awareness through self-care training programmes and were provided with assistive devices; these also may play a role in decreasing disability in the domain “getting around”.
Lowering disability scores in the domains “understanding and communication”, “getting along with people”, “life activity” and “participation” in the case group, compared with the control group, could be the result of the following: first, attending educational and training programmes, such as social skills training, art classes, and memory reinforcement techniques; group activities may have helped them to have more concentration, learn new tasks, be able to start conversations and find solutions to their problems in day to day life that improved their understanding and communication. Secondly, participation in group activities, life skills training, and group therapy, attending sport and leisure activities helped them to promote their dealing with people, maintaining friendships, making new friends, increasing their social interactions and decreasing their feeling of loneliness, which may have had positive effects in decreasing their disability in the domains “getting along with people”, “life activity” and “participation”. Thirdly, lower disability scores in “life activities” and “participation” could also be secondary to decreasing disability in “getting around” and “getting along with people”, which helped older individuals to perform these activities with more confidence.
Finally, although disability scores in the self-care domain decreased, there were no significant differences between the 2 groups. This finding was expected, because the people who use day services are typically less dependent and can more or less take care of themselves; thus, changes in this domain may not be as prominent as in other domains.
This study has some limitations. The sample size was small because the centre reception capacity was limited and there was only 1 day centre in Alborz province, and we had no other choice but to to increase the sample size. We could not follow the participants for more than 6 months, due to scarce resources, to see whether the positive effects last longer. The results of this study might be affected by these limitations, so more research with randomized design, larger sample and longer periods of time are suggested.
In conclusion, the comprehensive day care rehabilitation service package, issued by the SWO of Iran, may play a positive role in reducing disability and improving older adults functioning. This study also reconfirms the importance of delivering day care services to older adults, and suggests that policy-makers in health and rehabilitation move further toward the development of adult day centres. The authors also suggest further research on this package with more diverse older populations and longer service delivery and follow-up periods.
ACKNOWLEDGEMENTS
The authors would like to thank the Kahrizak Charity Foundation for its support, as well as the older participants who made this study possible. In addition, we are grateful to Dr Shatti for reviewing this article and appreciate his valuable comments.
The authors declare no conflicts of interest.
REFERENCES

