Martin W. G. Brinkhof, PhD1,2, Abdul Al-Khodairy, MD3, Inge Eriks-Hoogland, MD, PhD1,4, Christine Fekete, PhD1, Timo Hinrichs, MD1,5, Margret Hund-Georgiadis, MD6, Sonja Meier, MSc1, Anke Scheel-Sailer, MD2,4, Martin Schubert, MD7 and Jan D. Reinhardt, PhD1,2,8, for the SwiSCI Study Group
From the 1Swiss Paraplegic Research (SPF), Nottwil, 2Department of Health Sciences and Health Policy, University of Lucerne, Lucerne, 3Clinique Romande de Réadaptation, Sion, 4Swiss Paraplegic Center, Nottwil, 5Division of Sports and Exercise Medicine, Department of Sport, Exercise and Health, University of Basel, 6REHAB Basel, Basel, 7Spinal Cord Injury Center, University Hospital Balgrist, Zurich, Switzerland and 8Institute for Disaster Management and Reconstruction, Sichuan University, Chengdu and Hong Kong Polytechnic University, China
BACKGROUND: Health conditions in people with spinal cord injury are major determinants for disability, reduced well-being, and mortality. However, population-based evidence on the prevalence and treatment of health conditions in people with spinal cord injury is scarce.
OBJECTIVE: To investigate health conditions in Swiss residents with spinal cord injury, specifically to analyse their prevalence, severity, co-occurrence, and treatment.
METHODS: Cross-sectional data (n = 1,549) from the community survey of the Swiss Spinal Cord Injury (SwiSCI) cohort study, including Swiss residents with spinal cord injury aged over 16 years, were analysed. Nineteen health conditions and their self-reported treatment were assessed with the spinal cord injury Secondary Conditions Scale and the Self-Administered Comorbidity Questionnaire. Prevalence and severity were compared across demographics and spinal cord injury characteristics. Co-occurrence of health conditions was examined using a binary non-metric dissimilarity measure and multi-dimensional scaling. Treatment rates were also examined.
RESULTS: Number of concurrent health conditions was high (median 7; interquartile range 4–9; most frequent: spasticity, chronic pain, sexual dysfunction). Prevalence of health conditions increased with age and was higher in non-traumatic compared with traumatic spinal cord injury. Spinal cord injury specific conditions co-occurred. Relative frequencies of treatment were low (median 44%, interquartile range 25–64%), even for significant or chronic problems.
Discussion: A high prevalence of multimorbidity was found in community-dwelling persons with spinal cord injury. Treatment for some highly prevalent health conditions was infrequent.
Key words: spinal cord injury; community survey; secondary health conditions; comorbidity; multimorbidity; risk factors; treatment.
J Rehabil Med 2016; 48: 197–209
Correspondence address: Martin Brinkhof, Swiss Paraplegic Research, Guido A. Zäch Strasse 4, CH-6207 Nottwil, Switzerland. E-mail: martin.brinkhof@paraplegie.ch
Accepted Oct 23, 2015; Epub ahead of print Feb 1, 2016
INTRODUCTION
Health conditions (HCs) after spinal cord injury (SCI) are common and are regarded as major determinants for disability, reduced life satisfaction and emotional well-being (1), as well as mortality and diminished life expectancy (2). These HCs comprise a variety of physical or psychological diagnoses and symptoms that are direct or indirect consequences of impairments, activity limitations and participation restrictions and, in that sense, have been referred to as “secondary” HCs (3). Typical and frequent “secondary” HCs include chronic nociceptive and neuropathic pain, spasticity, urinary tract and pulmonary infections, circulatory problems, osteoporosis and related fractures, bowel and bladder regulation problems, sexual dysfunction, and pressure ulcers (4, 5). In addition, people living with SCI may incur a heightened risk of chronic diseases associated with the general ageing process, including cardiovascular disease, diabetes, cancer and depression (5). Yet, the attributable risk for such HCs to SCI, as reflected in the relative risk in comparison with the general population, is poorly documented. Apart from their immediate impact on the daily lives of people with SCI, the occurrence of HCs may induce considerable added economic expense, including direct costs for diagnosis, treatment and hospitalization (6, 7), as well as indirect costs, in particular lost earnings and early retirement, that often exceed direct costs (8).
Prevention measures and appropriate treatment may reduce the incidence and impact of many of these HCs after SCI (9). To inform and optimize health policy programmes aiming at reducing the impact of prevalent morbidity after SCI, there is a need for contemporary evidence on the prevalence and severity of HCs as well as their treatment. To arrive at a comprehensive picture of the prevalence of HC in SCI multiple stakeholder perspectives must be considered. While data on inpatient and outpatient treatments by diagnoses, based on the World Health Organization’s International Classification of Diseases (ICD), provide valuable information from health professionals’ perspective (10), a patient-centred, community-based approach focuses on relevant subjectively experienced HCs. There is currently a lack of community-based studies that could help informed decision-making and planning. In the present paper, data from the community survey of the Swiss Spinal Cord Injury (SwiSCI) Cohort Study (11, 12) were used to investigate HCs experienced by community-dwelling people with SCI in Switzerland. The specific aims of this study were to analyse: (i) the overall and group-specific prevalence of HCs; (ii) their severity; (iii) potential clustering of particular types of HCs; and (iv) their treatment, as reported by survey respondents.
METHODS
Design
Data from the cross-sectional, population-based community survey of the SwiSCI Cohort Study (11) were analysed. The SwiSCI community survey followed a modular structure and is described in detail in an accompanying paper (12). Data were collected by written or online questionnaires, and in special cases, by telephone interviews. The SwiSCI community survey was formally approved by the respective regional medical ethics committees. All participants provided written consent for anonymous use of their responses for the purpose of the study.
Sample
The survey was performed between late 2011 and early 2013 and included Swiss residents with a traumatic or non-traumatic SCI aged 16 years and older. Persons with congenital conditions leading to SCI, SCI in the context of palliative care, neurodegenerative disorders, and Guillain-Barré syndrome were excluded from the study. The SwiSCI population was recruited through the national association for persons with SCI (Swiss Paraplegic Association), 3 specialized SCI-rehabilitation centres, and a SCI-specific home care institution (11). In an accompanying paper in this issue we have provided a detailed description of the study protocol, the procedures for recruiting participants, characteristics of the study population, non-response bias and data quality of the SwiSCI community survey 2012 (12). This descriptive analysis shows that the design was efficient in recruiting 1,549 persons for the 2 core modules of the survey (Starter and Basic modules), which represented 49.3% of the sampled population. Response bias with respect to available person and SCI characteristics was limited and had minor impact on a variety of survey results. Self-reported demographics (gender; age) and SCI characteristics (year of SCI; lesion level; lesion severity) further showed good consistency with available medical record data. For this paper, data from the Starter Module and the Basic Module were used (12).
Measures
Demographic information included gender, age at the time of the questionnaire (in years), duration of formal education (in years), and language of response to the questionnaire (German, French or Italian). Adhering to International Spinal Cord Society (ISCoS) recommendations (13, 14), the following age groups were derived: 16–30, 31–45, 46–60, 61–75, and 76 years or older. To overcome issues of small cell counts in stratified analysis, the highest age groups were combined into a single age group comprising those aged 61 years or older.
Lesion characteristics included SCI aetiology, lesion group, and time since SCI diagnosis (in years). SCI aetiology was classified as traumatic or non-traumatic. Lesion group combined information on level and completeness of the lesion into the following 4 injury classes: incomplete paraplegia, complete paraplegia, incomplete tetraplegia, and complete tetraplegia. In deriving groups by time since injury, we considered using the cut-offs recommended by ISCoS (13, 14), but due to the small numbers of participants in some categories, we recombined and created the following groups for use in stratified analysis (in years): less than 6, 6–15, 16– 25, and 26 years or more.
Nineteen HCs and their treatment were assessed. Specific conditions that are commonly encountered by people living with SCI were included, as well as HCs that are highly prevalent in the general population (referred to as general HCs from here on) The Spinal Cord Injury Secondary Conditions Scale (SCI-SCS) (15) and the Brief International Classification of Functioning, Disability and Health (ICF) Core Sets for SCI (16, 17) were used as reference for the SCI-specific HCs. The SCI-SCS provides a reliable and valid scale for the assessment of specific HCs associated with SCI that directly and indirectly impact health and physical functioning (15). Assessment of impact refers to the past 3 months and is made on a 4-point Likert scale, with ordinal levels “not existing or insignificant”; “mild or infrequent”; “moderate or occasional”; and “significant or chronic”. A selection of 15 HCs and their severity was evaluated, including chronic pain; sexual dysfunction; spasticity; circulatory problems; bladder dysfunction; bowel dysfunction; contractures; urinary tract infections; autonomic dysreflexia; postural hypotension; injury caused by loss of sensation; respiratory problems; pressure ulcers; heterotopic ossification; and sleep disorders. Sleep disorders were added based on the Brief ICF Core Sets for SCI. To promote accurate reporting, participants were provided with descriptions of the distinctive symptoms and signs of a given HC. These descriptions were based on the original SCI-SCS, but simplified, shortened or disregarded, where judged appropriate, to shorten the questionnaire. A detailed description of the HCs used in SwiSCI compared with the SCI-SCS is provided in Appendix I. In addition, the presence of 4 general HCs, including heart disease, depression, diabetes and cancer was evaluated. Those conditions were evaluated on a binary scale using the Self-Administered Comorbidity Questionnaire (SCQ), posing the question “Do you have ‘…’?” for each of the general HCs with response options “Yes” and “No”. The SCQ is an efficient method with good reliability and validity for the assessment of comorbid conditions in the absence of medical records (18). Participants who indicated having a diagnosis (SCQ items) or a relevant HC (SCI-SCS items) were further asked whether they received treatment for it (“yes”/”no”).
Statistical analyses
Statistical analysis was performed using statistical packages Stata, version 13.1, and R, version 3.1.0.
Basic statistical procedures were used to describe the study population as well as the distribution of HCs. Using univariable analysis (variation of outcome by 1 explanatory variable), we further evaluated the prevalence of existing or significant HCs by participant characteristics. For that purpose, HCs that were evaluated with the SCI-SCS 4-point Likert scale were dichotomized into “not existing or insignificant” (i.e. the lowest level of the Likert scale) and “existing and relevant” (i.e. the 3 upper levels of the Likert scale). In case of participant characteristics with multiple levels, including age at time of the survey (4 groups), lesion group (4 groups) and time since injury (4 groups) we used post-hoc analysis, featuring contrasts with Bonferroni correction for multiple comparisons, to decompose overall associations in prevalence for a given HC into meaningful subgroups. For selected HCs that are characteristically reliant on self-report (e.g. chronic pain or sleep problems) multivariable analysis with distinct primary determinants, mediators and moderators to evaluate adjusted associations are in progress for later publication.
For the selection of 15 HCs that are considered specific to SCI we evaluated multimorbidity as the summary score (range 0–15). Unadjusted and adjusted incidence rate ratios were estimated for demographic variables (gender, age) and lesion characteristics (lesion class, lesion type, time since injury) using negative binomial regression modelling in order to account for overdispersion in the count data. A graphical evaluation of the co-occurrence of reported HCs was performed. For that purpose, the similarity of all pairs of current HCs was computed using a binary count of their simultaneous or separate occurrence. The resulting similarity measure for each person was then transformed into a single measure of mutual relationship between pairs of current HCs using the binary Lance-Williams non-metric dissimilarity measure (19). The Lance-Williams method is appropriate for the descriptive analysis of multimorbidity in people with SCI, which presumably arises from multiple sequels of the primary condition, implying a hierarchical algorithm. The Lance-Williams algorithm provides a flexible method to conserve the original space between clusters of HCs as much as possible (20). To facilitate 2-dimensional graphical display the similarity matrix was mapped onto a 2-dimensional coordinate system using multidimensional scaling (21). Using a bubble plot, the likelihood of the co-occurrence of any HC is indicated by the spatial position on the chart, relative to the respective position of all other HCs, while the bubble size proportionally indicates the overall prevalence of the HC.
Finally, the proportion of persons who indicated not receiving treatment for a relevant (SCI-SCS) or existing (SCQ) HC was assessed. For items that were evaluated according to the SCI-SCS, the proportion (with binomial 95% confidence interval) of persons receiving treatment was further evaluated separately for the group indicating a significant or chronic HC.
While all basic descriptive analysis were performed on the complete case data, ignoring missing data, we statistically accounted for both unit non-response as well as item non-response in all uni-variable analyses (22). Selective unit non-response, implying differential non-participation of persons with certain demographic or lesion characteristics who were contacted for participation, was handled through the use of inverse probability weights derived from the propensity scores for survey participation. The range of the inverse probability weights used in weighted analyses, which indicates the span in sampling weight for persons most over-represented and most under-represented, was 0.65–1.80 (12). Item non-response, implying missing values in explanatory variables or outcomes, was handled using a random forest imputation technique (R-package missForest (23)).
RESULTS
Table I shows descriptive characteristics of the 1549 study participants. The majority of the sample was male and the median age was 52 years. The youngest (16–30 years) and the oldest (76 years or older) age groups made up 8.3% and 6.1% of participants, respectively. The median length of education was 13 years, signifying upper secondary education including additional education after SCI as part of an adapted vocational reintegration programme. German was the predominant language of response; the relative size of the language groups is reflective of the Swiss general population. More than three-quarters (78.4%) of the participants reported a traumatic SCI aetiology. Overall, 69.2% of the participants were classified as having paraplegia, with 58.0% having incomplete lesions. The median time since injury was 14 years, with approximately one-quarter of participants reporting living with SCI for more than 25 years. The extent of missing information was between 0% (complete reporting; for gender, age, and language (by default) and 2.1% (for years of education)).
|
Table I. Characteristics of study participants (n = 1549) |
|
|
Characteristic [n missing] |
|
|
Gender, n (%) |
|
|
Male |
1,107 (71.5) |
|
Female |
442 (28.5) |
|
Age, years, median (IQR) |
52 (42–63) |
|
16–30 years |
129 (8.3) |
|
31–45 years |
377 (24.3) |
|
46–60 years |
571 (36.9) |
|
61–75 years |
378 (24.4) |
|
≥ 76 years |
94 (6.1) |
|
Years of education [32], median (IQR) |
13 (12–15) |
|
Language, n (%) |
|
|
German |
1,105 71.3) |
|
French |
376 (24.3) |
|
Italian |
68 (4.4) |
|
Aetiology [15], n (%) |
|
|
Traumatic |
1,202 (78.4) |
|
Non-traumatic |
332 (21.6) |
|
Lesion characteristics [12], n (%) |
|
|
Paraplegia, incomplete |
577 (37.5) |
|
Paraplegia, complete |
486 (31.6) |
|
Tetraplegia, incomplete |
314 (20.4) |
|
Tetraplegia, complete |
160 (10.4) |
|
Time since injury, years, [27], median (IQR) |
14 (6–25) |
|
< 1 years |
24 (1.6) |
|
1–5 years |
284 (18.7) |
|
6–10 years |
263 (17.3) |
|
11–15 years |
230 (15.1) |
|
16–20 years |
173 (11.4) |
|
21–25 years |
159 (10.4) |
|
26–30 years |
133 (8.7) |
|
31–35 years |
93 (6.1) |
|
≥ 36 years |
163 (10.7) |
|
Health conditions (HC) [25], median (IQR) |
|
|
Number of HCs reported on (maximum = 19) |
19 (19–19) |
|
Number of HCs, overall |
7 (4–9) |
|
Number of HCs, in sample reporting on all |
7 (5–9) |
Approximately 75% (n = 1,166) of participants provided a complete report on the severity of all of the 19 HCs posed in the questionnaire. Additional proportions, of 15.4% (n = 238) and 7.7% (n = 120), reported 15–18 and 1–14 HCs, respectively. The remaining 1.6% (n = 25) of participants did not provide any information. The median number of HCs that were at least of second-level severity (i.e. at least “mild severity” or “infrequent occurrence”) was 7, and this estimate was not affected by the overall completeness of reporting on HCs (Table I).
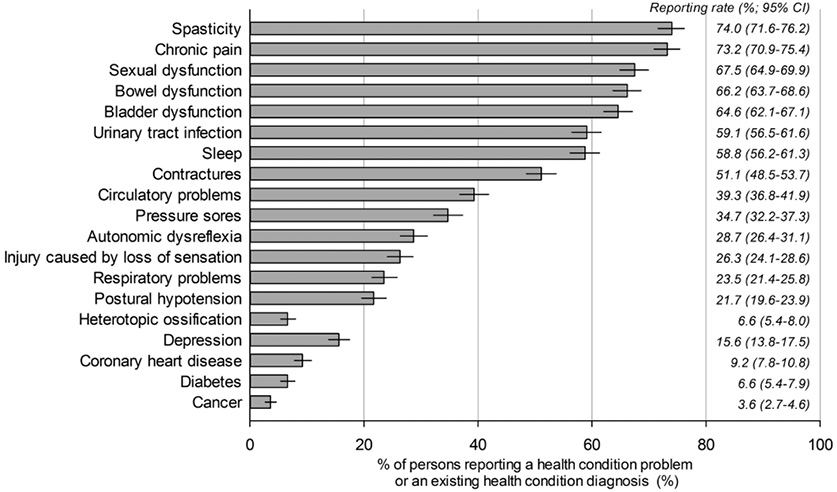
Fig. 1 shows the combined prevalence of HCs that were reported by the study population as mild or infrequent, moderate or occasional, or significant or chronic. The leading HCs included spasticity (74%), chronic pain (73.2%), and sexual dysfunction (67.5%). Cancer (3.6%), diabetes (6.6%) and heterotopic ossification (6.6%) were the least-often reported HCs. Sexual dysfunction was the HC most often reported as significant or chronic (43.6%), followed by chronic pain (36.6%), bladder dysfunction (26.3%) and spasticity (24%) (Table II). Although many individuals reported issues with bowel dysfunction (66.2%), the largest proportion reported having mild or infrequent issues (24.0%) compared with moderate or occasional (21.6%) and significant or chronic issues (20.6%).
|
Table II. Prevalence and severity of reported health conditions |
|||||
|
Health condition |
Severity of a health condition problem |
||||
|
n [missing] |
Not existing or insignificant n (%) |
Mild or infrequent n (%) |
Moderate or occasional n (%) |
Significant or chronic n (%) |
|
|
Spasticity |
1,436 [113] |
374 (26.0) |
319 (22.2) |
399 (27.8) |
344 (24.0) |
|
Chronic pain |
1,445 [104] |
387 (26.8) |
224 (15.5) |
305 (21.1) |
529 (36.6) |
|
Sexual dysfunction |
1,374 [175] |
447 (32.5) |
140 (10.2) |
188 (13.7) |
599 (43.6) |
|
Bowel dysfunction |
1,444 [105] |
488 (33.8) |
347 (24.0) |
312 (21.6) |
297 (20.6) |
|
Bladder dysfunction |
1,427 [122] |
505 (35.4) |
298 (20.9) |
248 (17.4) |
376 (26.3) |
|
Urinary tract infection |
1,423 [126] |
582 (40.9) |
262 (18.4) |
327 (23.0) |
252 (17.7) |
|
Sleep disorders |
1,456 [93] |
600 (41.2) |
303 (20.8) |
341 (23.4) |
212 (14.6) |
|
Contractures |
1,440 [109] |
704 (48.9) |
227 (15.8) |
251 (17.4) |
258 (17.9) |
|
Circulatory problems |
1,421 [128] |
862 (60.6) |
278 (19.6) |
169 (11.9) |
112 (7.9) |
|
Pressure sores |
1,386 [163] |
905 (65.3) |
218 (15.7) |
148 (10.7) |
115 (8.3) |
|
Autonomic dysreflexia |
1,417 [132] |
1,010 (71.3) |
206 (14.5) |
139 (9.8) |
62 (4.4) |
|
Injury caused by loss of sensation |
1,434 [115] |
1,057 (73.7) |
228 (15.9) |
111 (7.7) |
38 (2.7) |
|
Respiratory problems |
1,447 [102] |
1,107 (76.5) |
171 (11.8) |
103 (7.1) |
66 (4.6) |
|
Postural hypotension |
1,412 [137] |
1,106 (78.3) |
184 (13.0) |
93 (6.6) |
29 (2.1) |
|
Heterotopic ossification |
1,396 [153] |
1,304 (93.4) |
49 (3.5) |
23 (1.7) |
20 (1.4) |
|
|
Existing health condition diagnosis? |
||||
|
n [missing] |
No n (%) |
Yes n (%) |
|
|
|
|
Depression |
1,474 [75] |
1,244 (84.4) |
230 (15.6) |
|
|
|
Coronary heart disease |
1,488 [61] |
1,351 (90.8) |
137 (9.2) |
|
|
|
Diabetes |
1,495 [54] |
1,397 (93.4) |
98 (6.6) |
|
|
|
Cancer |
1,488 [61] |
1,435 (96.4) |
53 (3.6) |
|
|
Demographic characteristics
Many HCs varied according to demographic characteristics (Table III). Regarding gender, the largest contrasts with higher prevalence of health problems in females were found for bladder dysfunction, circulatory problems and depression. Males more often reported sexual dysfunction, pressure ulcers and diabetes. The variation by age group was even more pronounced, with significant contrasts for 10 out of 19 HCs. The prevalence of reported health issues was lower in the youngest age group (16–30 years) than in the oldest age group (61 years or older) for chronic pain, contractures, circulatory problems, respiratory problems, heart disease, diabetes and cancer. Depending on the HC, intermediate age groups were more similar to the highest age group (e.g. chronic pain) or the lowest age group (e.g. respiratory problems, heart disease). The age group 46–60 years reported a higher prevalence of issues with sexual dysfunction and sleep than the younger or older age groups, while the high rate of issues regarding postural hypotension in the youngest age group significantly contrasted with the lower rates in all older age groups.
|
Table III. Relative frequency of reported health condition problems and diagnoses stratified by demographic characteristics of participants |
|||||||||
|
Health condition |
Gender |
|
Age at time of questionnaire |
||||||
|
Male % (95% CI) |
Female % (95% CI) |
p |
|
16–30 years % (95% CI) |
31–45 years % (95% CI) |
46–60 years % (95% CI) |
≥ 61 years % (95% CI) |
p |
|
|
Spasticity |
71.2 (68.4–73.9) |
72.2 (67.7–76.3) |
0.70 |
|
76.0 (67.5–82.8) |
70.6 (65.7–75.1) |
68.7 (64.6–72.5) |
74.1 (69.8–78.0) |
0.19 |
|
Chronic pain |
70.5 (67.7–73.2) |
74.1 (69.7–78.0) |
0.17 |
|
53.9 (45.2–62.5) |
69.5 (64.6–74.1) |
74.6 (70.7–78.1) |
74.0 (69.8–77.9) |
< 0.001 |
|
Sexual dysfunction |
69.4 (66.5–72.1) |
50.8 (46.0–55.6) |
< 0.001 |
|
60.5 (51.6–68.7) |
59.5 (54.3–64.5) |
69.9 (65.9–73.7) |
61.6 (56.9–66.0) |
0.005 |
|
Bowel dysfunction |
61.5 (58.5–64.4) |
67.2 (62.5–71.5) |
0.043 |
|
67.2 (58.5–74.8) |
61.6 (56.4–66.5) |
64.6 (60.5–68.6) |
61.9 (57.3–66.3) |
0.57 |
|
Bladder dysfunction |
59.3 (56.2–62.2) |
67.4 (62.7–71.8) |
0.004 |
|
57.2 (48.3–65.6) |
58.6 (53.4–63.6) |
62.9 (58.7–66.9) |
63.8 (59.2–68.1) |
0.31 |
|
Urinary tract infection |
53.7 (50.6–56.7) |
58.5 (53.7–63.1) |
0.10 |
|
60.7 (51.8–69.0) |
55.7 (50.5–60.8) |
56.6 (52.3–60.7) |
51.6 (46.9–56.2) |
0.23 |
|
Sleep |
55.5 (52.5–58.5) |
60.9 (56.1–65.4) |
0.062 |
|
51.6 (42.8–60.2) |
52.3 (47.2–57.4) |
62.0 (57.9–66.0) |
56.7 (52.0–61.2) |
0.016 |
|
Contractures |
50.5 (47.4–53.5) |
52.7 (48.0–57.5) |
0.43 |
|
42.1 (33.7–51.0) |
41.4 (36.5–46.6) |
51.9 (47.7–56.1) |
60.0 (55.4–64.5) |
< 0.001 |
|
Circulatory problems |
34.1 (31.3–37.0) |
46.4 (41.6–51.1) |
< 0.001 |
|
25.9 (18.9–34.3) |
30.6 (26.1–35.4) |
39.8 (35.7–43.9) |
43.9 (39.4–48.6) |
< 0.001 |
|
Pressure sores |
34.1 (31.3–37.0) |
28.8 (24.7–33.3) |
0.053 |
|
29.1 (21.8–37.6) |
30.0 (25.6–34.9) |
32.9 (29.1–37.0) |
34.9 (30.5–39.4) |
0.42 |
|
Autonomic dysreflexia |
27.4 (24.7–30.1) |
28.1 (24.0–32.6) |
0.77 |
|
29.2 (21.9–37.8) |
26.6 (22.3–31.4) |
31.1 (27.3–35.1) |
24.1 (20.4–28.3) |
0.10 |
|
Injury caused by loss of sensation |
25.0 (22.5–27.7) |
23.3 (19.5–27.5) |
0.49 |
|
24.8 (18.1–33.0) |
26.4 (22.1–31.1) |
26.8 (23.2–30.7) |
20.4 (17.0–24.4) |
0.10 |
|
Respiratory problems |
23.3 (20.8–25.9) |
21.8 (18.1–26.0) |
0.53 |
|
19.1 (13.0–27.3) |
17.0 (13.5–21.2) |
21.0 (17.7–24.6) |
30.4 (26.3–34.8) |
< 0.001 |
|
Postural hypotension |
19.6 (17.3–22.1) |
23.3 (19.5–27.6) |
0.12 |
|
30.7 (23.3–39.4) |
19.9 (16.0–24.3) |
18.9 (15.8–22.4) |
20.9 (17.4–25.0) |
0.033 |
|
Heterotopic ossification |
6.6 (5.2–8.3) |
4.7 (3.0–7.2) |
0.18 |
|
2.7 (1.0–7.1) |
5.4 (3.5–8.4) |
6.0 (4.3–8.4) |
7.3 (5.2–10.0) |
0.26 |
|
Depression |
13.1 (11.2–15.3) |
23.4 (19.5–27.8) |
< 0.001 |
|
11.5 (6.8–18.6) |
16.6 (13.1–20.8) |
15.3 (12.5–18.7) |
17.8 (14.4–21.7) |
0.39 |
|
Coronary heart disease |
9.4 (7.7–11.3) |
9.0 (6.6–12.2) |
0.85 |
|
5.7 (2.8–11.5) |
5.0 (3.2–7.8) |
7.6 (5.6–10.2) |
15.3 (12.2–19.0) |
< 0.001 |
|
Diabetes |
7.6 (6.1–9.5) |
4.6 (2.9–7.0) |
0.039 |
|
0 (–) |
2.6 (1.3–5.0) |
5.3 (3.7–7.5) |
13.1 (10.3–16.7) |
< 0.001 |
|
Cancer |
3.1 (2.2–4.3) |
4.2 (2.7–6.5) |
0.28 |
|
0 (–) |
1.3 (0.4–3.1) |
3.2 (1.9–4.9) |
6.4 (4.3–8.9) |
< 0.001 |
|
95% CI: 95% confidence interval. |
|||||||||
Lesion characteristics
Reporting of many HCs also varied by lesion characteristics, with notable contrasts in 12 out of 19 HCs (Table IV). Post-hoc analysis of contrasts indicated differences due to lesion level, but not lesion completeness for sexual dysfunction and bladder dysfunction, with higher prevalence of health problems following paraplegia than tetraplegia. Likewise, yet conversely, circulatory problems, autonomic dysreflexia, respiratory problems and postural hypotension were more prevalent in people with tetraplegia than in those with paraplegia. Other HCs, such as urinary tract infection and pressure ulcers, differed by lesion severity rather than lesion level, with higher overall prevalence of HCs in complete than incomplete lesions. Similarly, yet conversely, reporting of contractures and depression was more frequent in the group with incomplete lesions. Contrasts in the reporting of spasticity and chronic pain were due to the combined effect of level and completeness of the lesion. The tetraplegia-incomplete group reported markedly higher prevalence of spasticity, while the tetraplegia-complete group reported lower levels of chronic pain than the other 3 groups.
Aetiology
With respect to aetiology of SCI, there were 9 out of 19 statistically significant contrasts, which, in all cases, signified a higher prevalence of HCs in the group with non-traumatic SCI (Table IV). Finally, contrast analyses revealed systematic variation in the reporting of problems with time since injury. The reporting of issues with spasticity was more frequent in the group with the shortest time since injury (≤ 5 years) than in any of the groups with longer time since injury (at least 6 years). Similarly, the higher reporting of depression in the groups with shortest time since injury (< 5 and 6–15 years) contrasted with the lower reporting in the groups with longest time since injury (16–25 and 26 years or more). Reporting of injury due to loss of sensation was less frequent in the group with the shortest duration since SCI only while it was elevated in the 3 other groups with longer time since injury (6–15, 16–25, and 26 years or more). Finally, the prevalence of circulatory problems in the group with shortest time since SCI was lower than in the group with the longest time since injury, while the other groups showed an intermediate level.
|
Table IV. Relative frequency (percentage with 95% confidence interval) of reported health condition problems or diagnoses stratified by lesion characteristics of participants |
||||||||||||||||
|
Health condition |
Paraplegia |
|
Tetraplegia |
|
|
Aetiology |
|
|
Time since SCI |
|
||||||
|
Incomplete % (95% CI) |
Complete % (95% CI) |
|
Incomplete % (95% CI) |
Complete % (95% CI) |
p |
|
TSCI % (95% CI) |
NTSCI % (95% CI) |
p |
|
≥ 5 years % (95% CI) |
6–15 years % (95% CI) |
16–25 years % (95% CI) |
≥ 26 years % (95% CI) |
p |
|
|
Spasticity |
67.1 (63.1–70.9) |
71.0 (66.7–75.0) |
|
80.4 (75.3–84.6) |
71.3 (63.7–77.9) |
< 0.001 |
|
69.8 (67.1–72.4) |
77.0 (72.0–81.3) |
0.014 |
|
78.6 (73.6–82.9) |
72.4 (68.2–76.2) |
67.1 (61.9–71.9) |
69.2 (64.3–73.6) |
0.009 |
|
Chronic pain |
71.8 (67.9–75.4) |
74.6 (70.5–78.4) |
|
72.1 (66.8–76.9) |
60.3 (52.4–67.7) |
0.009 |
|
70.6 (68.0–73.2) |
74.6 (69.5–79.1) |
0.17 |
|
70.7 (65.3–75.6) |
72.7 (68.7–76.5) |
70.4 (65.3–75.1) |
71.6 (66.9–76.0) |
0.88 |
|
Sexual dysfunction |
62.1 (58.0–66.1) |
71.2 (66.9–75.2) |
|
59.3 (53.6–64.8) |
59.7 (51.7–67.2) |
0.002 |
|
63.8 (60.9–66.6) |
64.2 (58.8–69.3) |
0.89 |
|
64.8 (59.1–70.0) |
63.5 (59.1–67.7) |
60.2 (54.8–65.3) |
68.8 (63.9–73.4) |
0.12 |
|
Bowel dysfunction |
63.4 (59.3–67.4) |
65.4 (61.0–69.6) |
|
61.9 (56.2–67.3) |
58.5 (50.5–66.0) |
0.44 |
|
61.1 (58.2–63.9) |
70.3 (65.0–75.1) |
0.003 |
|
58.8 (53.1–64.2) |
63.0 (58.6–67.2) |
64.7 (59.4–69.6) |
65.6 (60.6–70.2) |
0.29 |
|
Bladder dysfunction |
61.8 (57.6–65.8) |
67.5 (63.1–71.7) |
|
56.2 (50.5–61.8) |
55.7 (47.8–63.4) |
0.006 |
|
59.8 (56.9–62.6) |
68.0 (62.6–72.9) |
0.008 |
|
62.1 (56.5–67.4) |
62.4 (57.9–66.6) |
58.6 (53.2–63.8) |
64.0 (59.0–68.8) |
0.51 |
|
Urinary tract infection |
48.0 (43.9–52.2) |
67.8 (63.4–71.9) |
|
49.0 (43.3–54.6) |
59.6 (51.6–67.1) |
< 0.001 |
|
53.7 (50.7–56.5) |
59.9 (54.3–65.1) |
0.051 |
|
53.2 (47.6–58.8) |
52.1 (47.7–56.6) |
56.5 (51.1–61.7) |
60.2 (55.2–65.1) |
0.097 |
|
Sleep disorders |
58.9 (54.8–63.0) |
55.2 (50.7–59.7) |
|
54.8 (49.1–60.3) |
59.8 (51.9–67.3) |
0.47 |
|
55.5 (52.6–58.3) |
62.5 (57.0–67.6) |
0.027 |
|
54.3 (48.6–59.8) |
58.2 (53.7–62.5) |
53.8 (48.4–59.1) |
62.0 (57.0–66.8) |
0.094 |
|
Contractures |
55.7 (51.5–59.7) |
42.5 (38.1–47.1) |
|
57.8 (52.1–63.3) |
43.6 (36.0–51.6) |
< 0.001 |
|
48.9 (46.0–51.8) |
58.6 (53.1–63.8) |
0.002 |
|
49.6 (44.0–55.2) |
50.6 (46.2–55.1) |
49.1 (43.8–54.5) |
56.1 (51.1–61.1) |
0.21 |
|
Circulatory problems |
33.6 (29.8–37.7) |
38.3 (34.0–42.8) |
|
41.3 (35.8–47.0) |
44.6 (36.9–52.5) |
0.033 |
|
35.8 (33.1–38.6) |
44.2 (38.8–49.7) |
0.006 |
|
31.6 (26.6–37.0) |
39.1 (34.9–43.5) |
35.9 (30.9–41.1) |
43.2 (38.3–48.3) |
0.015 |
|
Pressure sores |
25.7 (22.3–29.5) |
41.0 (36.6–45.5) |
|
30.2 (25.2–35.8) |
40.2 (32.7–48.1) |
< 0.001 |
|
32.2 (29.6–35.0) |
33.6 (28.6–38.9) |
0.65 |
|
28.3 (23.6–33.7) |
30.6 (26.7–34.9) |
34.6 (29.7–39.9) |
37.0 (32.3–42.0) |
0.062 |
|
Autonomic dysreflexia |
23.3 (20.0–27.1) |
26.1 (22.3–30.2) |
|
33.7 (28.5–39.3) |
35.7 (28.5–43.5) |
< 0.001 |
|
27.9 (25.4–30.5) |
26.6 (22.0–31.7) |
0.65 |
|
23.6 (19.1–28.6) |
28.8 (25.0–33.0) |
28.6 (24.1–33.7) |
27.6 (23.3–32.3) |
0.39 |
|
Injury caused by loss of sensation |
24.3 (21.0–28.0) |
23.2 (19.6–27.3) |
|
27.1 (22.3–32.4) |
23.3 (17.3–30.6) |
0.65 |
|
24.7 (22.3–27.3) |
23.7 (19.4–28.7) |
0.71 |
|
18.0 (14.1–22.7) |
27.4 (23.6–31.5) |
24.7 (20.4–29.5) |
25.0 (20.8–29.6) |
0.026 |
|
Respiratory problems |
18.3 (15.3–21.7) |
19.9 (16.6–23.8) |
|
28.6 (23.7–34.1) |
37.0 (29.8–44.9) |
< 0.001 |
|
22.0 (19.7–24.5) |
25.5 (21.0–30.6) |
0.19 |
|
21.6 (17.3–26.6) |
23.1 (19.5–27.1) |
20.6 (16.6–25.3) |
26.5 (22.3–31.2) |
0.27 |
|
Postural hypotension |
16.6 (13.7–20.0) |
16.0 (12.9–19.6) |
|
27.0 (22.3–32.4) |
37.0 (29.7–44.9) |
< 0.001 |
|
21.8 (19.5–24.3) |
17.0 (13.2–21.6) |
0.068 |
|
19.8 (15.8–24.6) |
22.0 (18.6–26.0) |
18.6 (14.8–23.2) |
21.7 (17.8–26.2) |
0.62 |
|
Heterotopic ossification |
3.8 (2.5–5.7) |
8.9 (6.6–11.9) |
|
6.7 (4.2–10.5) |
5.0 (2.6–9.5) |
0.008 |
|
6.7 (5.4–8.3) |
3.8 (2.1–6.6) |
0.064 |
|
3.1 (1.7–5.7) |
6.0 (4.1–8.5) |
7.7 (5.3–11.0) |
6.6 (4.5–9.5) |
0.096 |
|
Depression |
19.6 (16.5–23.1) |
9.5 (7.1–12.5) |
|
21.4 (17.0–26.6) |
10.3 (6.3–16.3) |
< 0.001 |
|
15.7 (13.6–17.9) |
17.7 (13.9–22.3) |
0.38 |
|
18.1 (14.1–22.8) |
19.9 (16.6–23.8) |
14.0 (10.6–18.3) |
10.3 (7.5–13.8) |
< 0.001 |
|
Coronary heart disease |
8.9 (6.8–11.5) |
8.9 (6.6–11.8) |
|
11.3 (8.0–15.7) |
7.7 (4.3–13.3) |
0.60 |
|
8.2 (6.7–9.9) |
12.9 (9.6–17.2) |
0.011 |
|
9.6 (6.7–13.6) |
10.2 (7.7–13.2) |
9.3 (6.6–13.1) |
7.3 (5.1–10.3) |
0.50 |
|
Diabetes |
7.5 (5.6–10.0) |
6.2 (4.2–8.9) |
|
5.4 (3.2–8.9) |
7.9 (4.5–13.6) |
0.62 |
|
5.8 (4.5–7.3) |
9.8 (7.0–13.6) |
0.013 |
|
5.8 (3.6–9.1) |
7.2 (5.1–9.9) |
6.8 (4.5–10.1) |
6.6 (4.4–9.8) |
0.90 |
|
Cancer |
4.5 (3.1–6.5) |
2.8 (1.7–4.8) |
|
3.7 (2.1–6.4) |
0 |
0.36 |
|
2.3 (1.6–3.4) |
7.0 (4.8–10.1) |
< 0.001 |
|
5.0 (3.0–8.2) |
3.2 (2.0–5.2) |
1.6 (0.7–3.6) |
4.6 (2.8–7.4) |
0.089 |
|
SCI: spinal cord injury; TSCI: traumatic SCI; NTSCI: non-traumatic SCI; CI: confidence interval. |
||||||||||||||||
Multimorbidity
The mean number of concurrently reported SCI-specific HCs varied between 6.3 and 7.1 across the strata of demographic and SCI-related variables. Multimorbidity (range 0–15) varied with age, lesion characteristics, aetiology, and time since injury, but not with gender. Only the variation with lesion characteristics and aetiology was confirmed in the adjusted analysis (Table V). Participants with a paraplegic-complete or either tetraplegic lesion have an 11–13% higher expected count of HCs than those with a paraplegia-incomplete lesion. In addition, persons with a non-traumatic aetiology are expected to report 11% more concurring HCs than those with a traumatic lesion.
|
Table V. Relative risk of multimorbidity for self-reported SCI-specific conditions (sum-score ranging 0–15) in relation to demographics and lesion characteristics |
||||||
|
Parameter |
n |
Mean (95% CI) |
Unadjusted IRR (95% CI) |
p |
Adjusted IRR (95% CI) |
p |
|
Gender |
|
|
|
0.37 |
|
0.49 |
|
Male |
1,107 |
6.6 (6.4–6.8) |
1 |
|
1 |
|
|
Female |
442 |
6.8 (6.5–7.2) |
1.03 (0.97–1.09) |
|
1.02 (0.96–1.09) |
|
|
Age at questionnaire |
|
|
|
0.02 |
|
0.14 |
|
16–30 years |
129 |
6.3 (5.7–7.0) |
1 |
|
1 |
|
|
31–45 years |
377 |
6.3 (5.9–6.6) |
0.99 (0.89–1.11) |
|
0.99 (0.88–1.11) |
|
|
46–60 years |
571 |
6.9 (6.6–7.2) |
1.09 (0.98–1.21) |
|
1.07 (0.96–1.20) |
|
|
≥ 61 years |
472 |
6.9 (6.5–7.2) |
1.09 (0.97–1.21) |
|
1.06 (0.95–1.19) |
|
|
Lesion characteristics |
|
|
|
0.047 |
|
0.006 |
|
Paraplegia, incomplete |
584 |
6.4 (6.1–6.6) |
1 |
|
1 |
|
|
Paraplegia, complete |
488 |
6.9 (6.6–7.2) |
1.09 (1.02–1.16) |
|
1.11 (1.04–1.19) |
|
|
Tetraplegia, incomplete |
316 |
6.9 (6.4–7.3) |
1.08 (1.00–1.17) |
|
1.11 (1.02–1.20) |
|
|
Tetraplegia, complete |
161 |
6.9 (6.3–7.5) |
1.09 (0.99–1.20) |
|
1.13 (1.02–1.25) |
|
|
Aetiology |
|
|
|
0.012 |
|
0.003 |
|
Traumatic |
1,215 |
6.5 (6.3–6.8) |
1 |
|
1 |
|
|
Non-traumatic |
334 |
7.1 (6.7–7.5) |
1.08 (1.02–1.15) |
|
1.11 (1.04–1.20) |
|
|
Time since SCI |
|
|
|
0.046 |
|
0.18 |
|
0–5 years |
311 |
6.4 (6.0–6.8) |
1 |
|
1 |
|
|
6–15 years |
507 |
6.7 (6.4–7.1) |
1.05 (0.97–1.14) |
|
1.07 (0.99–1.15) |
|
|
16–25 years |
347 |
6.5 (6.1–6.9) |
1.02 (0.94–1.11) |
|
1.04 (0.95–1.14) |
|
|
≥ 25 years |
384 |
7.1 (6.7–7.4) |
1.11 (1.02–1.19) |
|
1.09 (1.01–1.19) |
|
|
Unadjusted and adjusted incidence rate ratios (IRR) are from univariable and multivariable regression modelling using the negative binomial distribution and Wald tests for significance testing. CI: confidence interval. |
||||||
Co-occurrence of health conditions
Multidimensional scaling of the co-occurrence of HCs revealed a clear clustering of the most common conditions, including sexual dysfunction, spasticity, bowel dysfunction, chronic pain, bladder dysfunction and urinary tract infections. Individual HCs adjacent to this cluster included sleep disorders, contractures, circulatory problems, followed by injury due to loss of sensation, pressure ulcers and autonomic dysreflexia. The reporting of general HCs, including heart disease, cancer, depression and diabetes, was weakly associated with any other specific HC (Fig. 2).
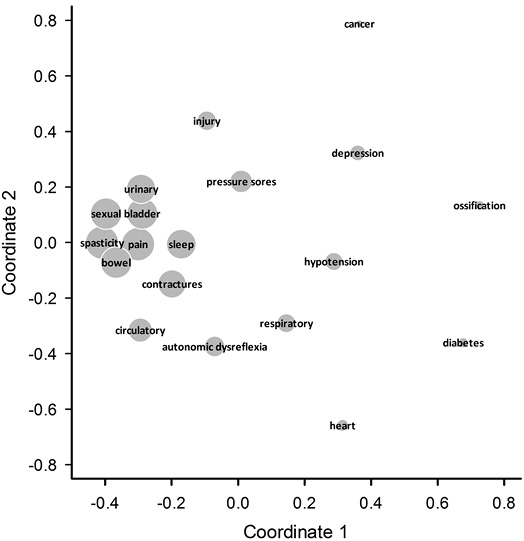
Fig. 2. Two-dimensional representation of the joint reporting of health conditions (HCs) by use of multidimensional scaling. The space between HCs provides a proximity measure for concurrent reporting. Symbol sizes are proportional to the frequency of reporting.
Treatment
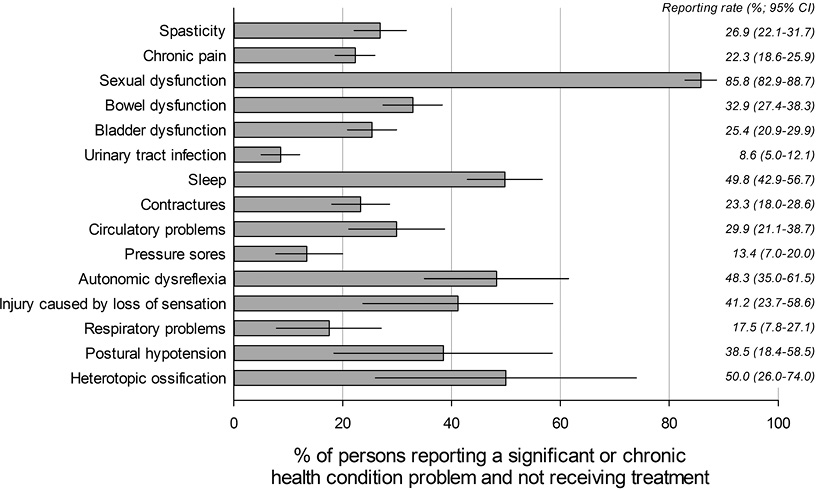
Finally, we investigated whether persons who reported a HC received treatment for that HC. The median number of treatments reported per individual was 3 (interquartile range (IQR) 1–5) and the median proportion of HCs treated was 44% (IQR 25–64%). Not receiving treatment was least frequently reported for general HCs, ranging from 3.9% to 25.2% for heart disease and depression, respectively. In comparison, absence of treatment among the specific HCs that are closely linked to SCI ranged from 26.7% for urinary tract infection to 85.5% for sexual dysfunction. Other HCs with high reporting of non-treatment included postural hypotension (75.9%), injury caused by loss of sensation (73.3%), autonomic dysreflexia (68.9%) and sleep disorders (69.4%). Restricting the breakdown to HCs that were reported as significant or chronic only, sizeable rates for absence of treatment were generally confirmed, particularly for sexual dysfunction (85.5%), sleep disorders (49.8%), autonomic dysreflexia (48.3%), and, although with low prevalence, heterotopic ossification (50%) (Fig. 3). Other commonly reported HCs of significant or chronic nature, including urinary tract infection and pressure ulcers, were associated with markedly lower rates of non-treatment (8.6% and 13.4%, respectively).
DISCUSSION
This survey of Swiss community-dwelling persons with SCI showed a high prevalence of self-reported HCs. Leading HCs included spasticity, chronic pain, sexual dysfunction and bowel and bladder problems. The prevalence of HCs varied across demographic and SCI characteristics. Some HCs were more often reported by females while others were more prevalent in male participants. Higher age was often associated with increased odds of reporting particular HCs. While lesion characteristics were associated with specific HCs, some were more prevalent in persons with paraplegia and in those with complete lesions (e.g. sexual dysfunction), while others were more often reported by people with incomplete lesions or tetraplegia (e.g. spasticity). Non-traumatic aetiology was consistently associated with an increased frequency of reported HCs. Many SCI-specific HCs co-occurred. Patients reported not receiving treatment for many of the HCs, even when the problem was viewed as significant or chronic.
The prevalence and severity of SCI-specific HCs reported in this study is, to a large extent, comparable to findings from other high-income settings with considerable investments in healthcare and similar life expectancy following SCI. In agreement with our results, a recently conducted scoping review found that the most common conditions, with a reported prevalence of over 50%, were pain, bladder and bowel regulation problems, as well as spasticity (5). Comparable to our findings, the prevalence of pressure ulcers and circulatory problems were between 25% and 50% (5). In a population-based study from Canada, Noreau et al. found the highest prevalence rates for urinary tract infections, spasticity and hypotension (24), while Adriaansen et al. found neuropathic pain, musculoskeletal pain and urinary tract infections to be the most frequently reported HCs in wheelchair-dependent persons with SCI from the Netherlands (4). Severity of SCI-related HCs was rated highest in chronic pain and sexual dysfunction in our study. This finding is in line with reports of pain being a severe problem in approximately one-third of persons with chronic pain (5, 25). Although there are few studies on sexual dysfunction in SCI, our figures are higher than reported elsewhere (5, 26, 27). Compared with other SCI studies, we found similar, to slightly lower, depression rates (28–30). Available estimates for depression in the Swiss general population are based on different assessment methods (31), precluding a meaningful comparison with our results. In line with the evidence from other SCI studies (32–34), the prevalence of other general HCs, including diabetes and cancer, appeared to be higher in our sample compared with the general population (35, 36).
In our study, some SCI-specific HCs were more often reported by women, others by men. Research on gender differences in HCs in SCI is sparse and results are difficult to interpret (4). However, our results regarding general HCs, i.e. depression and diabetes, reflect the higher prevalence of depression and the lower prevalence of diabetes in the female general population of Switzerland (31, 35, 37), which might suggest that gender-differences are not affected by SCI. Conclusive evidence may principally come from the comparison of standardized, age- and sex-adjusted prevalence, but relevant estimates of these HCs that are based on self-report using the SCQ are currently not available for the Swiss general population. In line with findings from other SCI studies (4, 24, 38), we observed a higher prevalence of chronic pain, contractures, circulatory problems, respiratory problems, heart disease, diabetes and cancer in the oldest age group. The middle-aged group reported higher prevalence of sexual dysfunction and sleep disorders than the younger or older age groups. In contrast to previous findings (24), we found a higher prevalence of postural hypotension in the youngest age group compared with the older ones. As explanations for these age differences are widely lacking, longitudinal analysis of objective cardiovascular data is warranted to clarify the role of ageing in the change in blood pressure regulation (5).
Many differences in prevalence of HCs with lesion characteristics, such as more respiratory problems in tetraplegia and a higher frequency of pressure ulcers in persons with complete lesions (4, 39), reflect well-known physiological differences. Other variations may be due to differences in the lived experience rather than actual differences in pathophysiology. For example, although there is no obvious reason for sexual dysfunction to be more prevalent in paraplegia, our results may point to differential preferences of persons with para- and tetraplegia. This assumption is supported by Anderson et al. (40), who found that persons with paraplegia rated regaining sexual function as their highest priority to improve their quality of life; while for persons with tetraplegia restoration of arm-hand function was more important. The higher prevalence of self-reported HCs in persons with non-traumatic SCI may be explained in several ways. First, persons with non-traumatic SCI are, on average, older, and underlying causes such as ischaemia, bleeding, and tumours are events of older age. Secondly, causes underlying non-traumatic SCI may additionally enhance the risk of HCs. To shed more light on these phenomena, multivariable analysis and, eventually, longitudinal studies are planned. Finally, most people with SCI were facing multiple HCs, and the extent of the multimorbidity for SCI-specific HCs varied with lesion characteristics and aetiology. This finding should be taken into consideration in the development of guidelines and policy that target improvements in health and community functioning, as well as in improving reimbursement systems by specifically considering the impact of multimorbidity on functioning, e.g. through functioning-related case-mix groups (41).
Across HCs, there was a wide variability in the proportions of individuals who reported receiving treatment. While a relatively high proportion of those with cancer, diabetes, heart disease and depression received treatment, only a very low proportion of those with SCI-related conditions reported receiving treatment, even for conditions reported as significant or chronic. This lack of treatment was most striking for the SCI-related HCs pain and sexual dysfunction. The low prevalence of reported treatment for sexual function may have 2 explanations: first, education and treatment options are not always provided, and secondly it may be the case that not all patients choose to seek treatment for sexual dysfunction due to social and personal inhibitions (42). Treatment rates might be determined by a number of factors, such as the impact of the disease on functioning, quality of life and mortality, the availability of evidence-based treatment options, the clinician’s and patient’s knowledge of these options, the access to treatment, the treatment burden (e.g. time effort, travel, costs, side-effects), the potential benefits and harms, and patient preferences (43). The present study also showed that individuals with SCI commonly receive simultaneous treatment for multiple HCs. In these individuals, clinical decision-making might also be influenced by considerations on the cumulative burden of pharmacological as well as non-pharmacological treatments, interactions between treatments, and the resulting need for prioritization.
A potential limitation of the study concerns the bias introduced through self-report of HCs. First, it might be the case that the severity of a HC is underestimated, as treatments reduce symptoms (e.g. pain is not declared as problem as constant medication reduces pain). Secondly, existing conditions might not be reported, as the technical terminology used in the questionnaire might have caused problems. Although we provided explanations for technical terms, such as autonomic dysreflexia or heterotopic ossification, it remains unclear if all participants understood these. Our results on treatments raise 2 further issues related to the problem of bias in self-report data. First, it must be clarified when and why persons with SCI rated a condition as untreated. Was this due to insufficient attention of caregivers, unavailable treatment, lack of access, because a treatment attempt was not successful, or because person were not aware of treatments? Secondly, it must be determined in which of these conditions and to what extent an available treatment would result in satisfactory improvement in the condition. Although recall bias cannot be excluded, we consider the risk minimal, given that the questionnaire evaluated HCs occurring in the last 3 months. Lastly, HCs that are considered socially undesirable, such as sexual dysfunction or depression (44, 45), may have been under-reported. Future studies that additionally involve chart review or clinical assessment may conclusively verify the extent of the bias in the self-report of HCs and their treatment.
Acknowledging the potential limitations of self-reported evidence, it remains important to note that personal accounts of HCs and their treatment may in fact reflect the reiteration of clinical information that was communicated during patient consultation. Community follow-up in Switzerland involves annually scheduled check-ups to monitor patient health and functioning and to strengthen patient’s self-awareness and self-responsibility. The self-report of morbidity is increasingly important in the shared decision-making by medical provider and patient, to facilitate clinical and rehabilitation management that takes both clinical prognosis as well as the lived experience and needs of patients into account. In this respect, the present community survey provides a distinct account of the prevalence and severity of the HCs at stake across the different patient groups. Further strengths of our study include its large sample size and the fact that the sample represents the Swiss SCI community (12). The study population is based on a large community sample rather than on a group selected by convenience, and the data meet high quality standards (12). Hence SwiSCI 2012 provides a sound basis for model-based future studies of the impact of socio-demographic factors and lesion characteristics on specific HCs. In addition, a comprehensive set of HCs was analysed in this study, drawing a detailed picture of HCs in persons with SCI. Moreover, the analysis was adjusted for unit as well as item non-response.
In conclusion, the results of the present study highlight a high prevalence of self-reported multimorbidity in community-dwelling persons with SCI. Treatment rates for some highly prevalent HCs appear to be low in Switzerland, suggesting a need for respective intervention.
ACKNOWLEDGEMENTS
The authors would like to thank all the participants in the SwiSCI survey for their time and effort spent in responding to the questions. The authors also thank Jonviea Chamberlain for her general support in data preparation, valuable discussions and suggestions. Armin Gemperli kindly provided Stata code for the multidimensional scaling analysis. The members of the SwiSCI Steering Committee are: Xavier Jordan, Bertrand Léger (Clinique Romande de Réadaptation, Sion); Michael Baumberger, Hans Peter Gmünder (Swiss Paraplegic Center, Nottwil); Armin Curt, Martin Schubert (University Clinic Balgrist, Zürich); Margret Hund-Georgiadis, Kerstin Hug (REHAB Basel, Basel); Hans Georg Koch (Swiss Paraplegic Association, Nottwil); Hardy Landolt (Representative for persons with SCI, Glarus); Hannjörg Koch (SUVA, Luzern); Mirjam Brach, Gerold Stucki (Swiss Paraplegic Research, Nottwil); Martin Brinkhof, Christine Thyrian (SwiSCI Study Center at Swiss Paraplegic Research, Nottwil). This study was funded by the Swiss Paraplegic Research (SPF), Nottwil, Switzerland.
|
Appendix ı. Description of the methodology used to evaluate health conditions in the SwiSCI Community Survey 2012 as compared to the Spinal Cord Injury Secondary Conditions Scale (SCI-SCS) (15) |
|||||
|
Original SCI-SCS introduction: For the following 16 health problems, please rate how much each one affected your activities and independence in the last 3 months. If you have not experienced a secondary condition in the last 3 months or if it is an insignificant problem for you, please circle ‘’0.’’ Use the following scale to rate each of the secondary conditions. |
|||||
|
SwiSCI introduction: For the following health problems, please indicate how often these problems occurred in the last 3 months and how severe they were. |
|||||
|
Original SCI-SCS response scale: 0=NOT experienced in the last 3 months or is an insignificant problem. 1=MILD or INFREQUENT problem. 2=MODERATE or OCCASIONAL problem. 3=SIGNIFICANT or CHRONIC problem. |
SwiSCI response scale: 0=Not experienced, insignificant problem 1=Mild or infrequent problem 2=Moderate or occasional problem 3=Significant or chronic problem |
||||
|
SCI-SCS title |
SwiSCI title |
SCI-SCS description |
SwiSCI description |
Rating |
|
|
Pressure sore(s) |
Pressure sores, decubitus |
These develop as a skin rash or redness and progress to an infected sore. Also called skin ulcers, bedsores, and decubitus ulcers. |
(no explanation given as it is expected that persons know this condition) |
0 1 2 3
|
|
|
Injury caused by loss of sensation |
(original) |
Injury may occur because of a lack of sensation, such as burns from carrying hot liquids in the lap or sitting too close to a heater or fire. |
These are e.g. burns from carrying hot liquids in the lap or sitting too close to a heater or fire. |
0 1 2 3
|
|
|
Muscle spasms (spasticity) |
Muscle spasms, spasticity |
Spasticity refers to uncontrolled, jerky muscle movements, such as uncontrolled muscle twitch or spasm. Often spasticity increases with infection or some kind of restriction, like a tight shoe or belt. |
(no explanation given) |
0 1 2 3 |
|
|
Contractures |
(original) |
A contracture is a limitation in range of motion caused by a shortening of the soft tissue around a joint, such as an elbow or hip. This occurs when a joint cannot move frequently enough through its range of motion. Pain often accompanies this problem. |
This is a limitation in range of motion of a joint. |
0 1 2 3 |
|
|
Heterotopic bone ossification |
(original) |
This is an overgrowth of bone, often occurring after a fracture. Early signs include a loss of range of motion, local swelling and warmth at the area to the touch. This condition must be diagnosed by a physician. |
This is an overgrowth of bone, often occurring after a fracture. This condition must be diagnosed by a physician. |
0 1 2 3 |
|
|
Diabetes mellitus |
Diabetes (assessed using SCQ) |
Diabetes is a problem resulting from irregularities in blood sugar levels. Symptoms include frequent urination and excessive thirst. This condition is diagnosed by a physician. |
(no explanation given) |
0 1 |
|
|
Bladder dysfunction |
(original) |
Incontinence, bladder or kidney stones, kidney problems, urine leakage and urine back up are all symptoms of bladder dysfunction. NOTE: There is a separate item for urinary tract infections. |
This includes incontinence, bladder or kidney stones, kidney problems, urine leakage and urine back up. |
0 1 2 3 |
|
|
Bowel dysfunction |
(original) |
Diarrhoea, constipation, ‚‘accidents,‘‘ and associated problems are signs of bowel dysfunction. |
This includes diarrhoea and constipation. |
0 1 2 3 |
|
|
Urinary tract infections |
(original) |
This includes infections such as cystitis and pseudomonas. Symptoms include pain when urinating, a burning sensation throughout the body, blood in the urine and cloudy urine. |
This includes kidney or bladder infection. |
0 1 2 3 |
|
|
Sexual dysfunction |
(original) |
This includes dissatisfaction with sexual functioning. Causes for dissatisfaction can be decreased sensation, changes in body image, difficulty in movement, and problems with bowel or bladder, like infections. |
This includes dysfunction in sexual arousal, erection and reaching orgasm. |
0 1 2 3 |
|
|
Appendix ı. Contd. |
|||||
|
SCI-SCS title |
SwiSCI title |
SCI-SCS description |
SwiSCI description |
Rating |
|
|
Autonomic dysreflexia |
(original) |
Autonomic dysreflexia, sometimes called hyperreflexia, results from interference in the body‘s temperature regulating systems. Symptoms of dysreflexia include sudden rises in blood pressure and sweating, skin blotches, goose bumps, pupil dilation and headache. It can also occur as the body‘s response to pain where an individual doesn‘t experience sensation. |
Symptoms are sudden rises in blood pressure and sweating, skin blotches, goose bumps, pupil dilation and headache. |
0 1 2 3 |
|
|
Postural hypotension |
(original) |
This involves a strong sensation of lightheadedness following a change in position. It is caused by a sudden drop in blood pressure. |
This involves a strong sensation of lightheadedness following a change in position. It is caused by a sudden drop in blood pressure. |
0 1 2 3 |
|
|
Circulatory problems |
(original) |
Circulatory problems involve the swelling of veins, feet or the occurrence of blood clots. |
This involves the swelling of veins, feet or the occurrence of blood clots. |
0 1 2 3 |
|
|
Respiratory problems |
(original) |
Symptoms of respiratory infections or problems include difficulty in breathing and increased secretions. |
(original) |
0 1 2 3 |
|
|
Chronic pain |
Pain |
This is usually experienced as chronic tingling, burning or dull aches. It may occur in an area that has little to no feeling. |
(no explanation) |
0 1 2 3 |
|
|
Joint and muscle pain |
(not assessed using SCI-SCS in SwiSCI) |
This includes pain in specific muscle groups or joints. People who must overuse a particular muscle group, such as shoulder muscles, or who put too much strain on their joints are at risk of developing pain. |
|
0 1 2 3 |
|
|
(not assessed in the SCI-SCS) |
Sleep problems |
|
This includes problems falling asleep, sleeping through the night and waking up early. |
0 1 2 3 |
|
|
SCQ: Self-Administered Comorbidity Questionnaire; SwiSCI: Swiss Spinal Cord Injury cohort study. |
|||||
REFERENCES

