Myrna Elena van Geffen, MSc1,2, Nienke ter Hoeve, MSc1,2, Madoka Sunamura, MD1, Henk J. Stam, MD, PhD, FRCP2, Ron T. van Domburg, PhD3 and Rita J. G. van den Berg-Emons, PhD2
From the 1CAPRI Cardiac Rehabilitation Centre, 2Department of Rehabilitation Medicine and 3Department of Cardiology, Erasmus Medical Centre, Rotterdam, The Netherlands
OBJECTIVE: To estimate fatigue during and after a multidisciplinary cardiac rehabilitation programme and its association with aerobic capacity.
DESIGN: Longitudinal cohort study.
Patients: A total of 121 patients with coronary artery disease (79% men), mean age 57 years.
METHODS: Fatigue was measured with the Fatigue Severity Scale (FSS) and aerobic capacity with the 6-min walk test (6MWT). FSS scores ≥ 4 were defined as fatigue and > 5.1 as severe fatigue. Measurements were taken before (T0) and after rehabilitation (T1) and at 1-year follow-up (T2).
RESULTS: Fatigue decreased from 3.49 at baseline to 3.03 post-rehabilitation (p = 0.002) and decreased further to 2.75 at follow-up (p < 0.001 vs T0). At baseline, 17.7% of patients were classified as severely fatigued. After cardiac rehabilitation, the prevalence decreased to 10.6% (p < 0.001) and to 8.1% at follow-up (p = 0.011 vs T0). Although the prevalence of severely fatigued patients decreased, it was still high compared with healthy individuals (3.5%). Aerobic capacity was weakly associated with a reduction in fatigue (p = 0.030).
CONCLUSION: Fatigue decreased during and after cardiac rehabilitation. However, the prevalence of severely fatigued patients remained high after cardiac rehabilitation. Fatigue should be identified at an early stage in order to provide additional programmes aiming to reduce severe fatigue.
Key words: cardiac rehabilitation; fatigue, severity; depression; aerobic capacity; coronary artery disease.
J Rehabil Med 2015; 47: 569–574
Correspondence address: Myrna Elena van Geffen, Department of Rehabilitation Medicine, Erasmus Medical Centre, CAPRI Cardiac Rehabilitation, NL-3016BC Rotterdam, The Netherlands. E-mail: m.vangeffen@erasmusmc.nl
Accepted Feb 18, 2015; Epub ahead of print May 5, 2015
INTRODUCTION
Cardiovascular diseases (CVD) are the leading cause of death worldwide (1). In 2008, 17.3 million people died from CVD, which represents 30% of global deaths (1). The most common form of CVD is coronary artery disease (CAD), which caused 7.3 million deaths in 2008 (1). The economic impact of CAD is high, due to high healthcare costs and sickness absence (2).
Cardiac rehabilitation (CR) is known to improve the physical and psychological status of patients with CAD, thereby reducing both cardiovascular mortality and total mortality (3). Physical improvements are often seen in aerobic capacity, for which previous intervention studies have shown favourable effects directly after exercise-based CR (3, 4).
Studies (5, 6) have shown that illness-related fatigue is one of the most disturbing symptoms experienced by patients with CAD (6). This type of fatigue is difficult to manage, because it differs from any earlier experience with fatigue unrelated to CAD (6). Another reason for the often quite considerable impact of fatigue is that fatigue negatively influences physical and mental capacity and therefore quality of life (5). Despite the impact fatigue might have, only 2 studies have examined the severity of the problem in patients with CAD (5, 6). One study (6) found that fatigue decreases over time without participation in CR. Nevertheless, half of patients still reported fatigue 4 months to 2 years after myocardial infarction. It appears that additional interventions, such as CR, are necessary to improve long-term fatigue after CAD. Besides the direct influence on fatigue, participation in CR may also indirectly improve fatigue. A study (5) showed that fatigue levels seem to be associated with aerobic capacity in patients with CAD. It may therefore be hypothesized that improvements in aerobic capacity, which are known to occur during exercise-based CR, lead to a decline in fatigue. However, those studies that have examined the effect of CR on fatigue focused only on patients with heart failure and, indeed, reported less fatigue after exercise-based CR (7, 8).
The primary aim of this study was to estimate fatigue in patients with CAD before and after CR and at 9 months follow-up. A secondary aim was to explore whether aerobic capacity was associated with fatigue. Because fatigue or loss of energy is one of the main symptoms of depression (6) and depression is common in patients with CAD (9), depression seems to overlap with illness-related fatigue (6, 10). Thus, all analyses were controlled for depression.
METHODS
Patients and design
Inclusion criteria were: (i) a diagnosis of acute myocardial infarction or angina pectoris; (ii) scheduled to participate in the regular CR programme; (iii) 18 years of age or older; (iv) provided signed informed consent; and (v) proficient in Dutch language. Exclusion criteria were: (i) comorbidities; (ii) left ventricle ejection fraction of < 40%; and (iii) psychological or cognitive impairments that might impair participation in the rehabilitation programme.
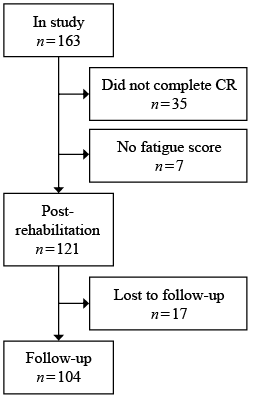
Between October 2010 and July 2012, 163 consecutive patients were included in this single-centre prospective observational cohort study. Of these, 121 patients who had completed the CR programme and who had at least 1 fatigue score were included in the analysis (Fig. 1). Reasons given by patients (n = 17) for not participating in the follow-up measurements were: (i) lack of time, (ii) immobility; and (iii) unwillingness.
Measurements were taken at the following time-points: pre-rehabilitation (T0), post-rehabilitation (T1), and 1 year after the start of rehabilitation (9-month follow-up) (T2). The study was approved by the medical ethics committee of the Erasmus Medical Centre in Rotterdam.
Cardiac rehabilitation programme
The rehabilitation programme at Capri cardiac rehabilitation centre is based on the Dutch guidelines for CR (11). The duration of CR varied from 4 to 13 weeks, depending on the patient’s individual improvement. The CR programme was completed when an individual’s physical and psychosocial goals were achieved. This was evaluated with an exercise test on a bicycle ergometer and a consultation with the multidisciplinary team that consisted of a social worker, physical therapist and nurse.
The patients exercised twice a week. One training session lasted 75 min; the other session had additional relaxation exercises and lasted 105 min. The exercise sessions consisted of: (i) warming-up exercises; (ii) gymnastics exercises; (iii) an aerobic programme of 12 min, which involved a combination of brisk walking and jogging with increasing the component of jogging over time; (iv) sports activities; and (v) cooling-down exercises.
In addition to the regular exercise programme, patients could voluntarily attend educative medical sessions, risk factor sessions, healthy diet sessions or emotional advice sessions. Stress management modules, dietary advice modules and smoking cessation programmes were also provided to help adjust the lifestyle behaviour of the patients.
Measures
Fatigue. The primary outcome measure was fatigue, which was measured with the Fatigue Severity Scale (FSS). The FSS consists of 9 questions. Answers are given on a 7-point scale from “totally disagree” to “totally agree”. A higher FSS score indicates more severe fatigue (12, 13). Both the mean FSS score (SD), indicating the level of fatigue, and the prevalence of fatigued patients and severely fatigued patients were calculated. Patients were classified as being fatigued if their FSS score was ≥ 4 and ≤ 5.1 (12) and as being severely fatigued if their FSS score was > 5.1 (13). The FSS has been found reliable and valid in healthy subjects (12), in patients with multiple sclerosis (12, 14) and in patients with recent ischaemic stroke (12).
Aerobic capacity. Aerobic capacity was measured with the 6-min walk test (6MWT). The 6MWT is a submaximal exercise test for measuring aerobic capacity (15). During this test, patients walk as fast as they can over a distance of 30 m during a period of 6 min. The distance walked is recorded. Patients were not allowed to run, and standardized words of encouragement were given every minute. The 6MWT has been found moderately reliable and moderately valid in patients with CAD undergoing CR (16). The 6MWT has been shown to be responsive to the relevant clinical changes that occur during CR (16).
Depression. Depression was measured with the Hospital Anxiety and Depression scale (HADS). This questionnaire has subscales for depression and anxiety, each comprising 7 items. Answers are given on a 4-point scale from “never” to “almost always”. Higher scores on the depression subscale indicate higher levels of depression (17). Patients with a score ≥ 8 are considered to have signs of depression (18). The HADS is a valid instrument for the screening of depression in patients with CAD (17, 19).
Baseline characteristics. Data on age, gender, body mass index (BMI), waist circumference, blood pressure, cardiac diagnosis for referral, smoking, diabetes and medication were obtained from the patients’ medical files for the purpose of descriptive statistics. In addition, the number of training sessions was recorded.
Procedure
Depending on their individual preferences, patients completed the questionnaires either on paper or digitally. The questionnaires were completed at home. The 6MWT was performed either at Capri cardiac rehabilitation centre or at Erasmus Medical Centre under the supervision of a nurse, physical therapist or researcher.
Statistical analysis
Descriptive statistics were used to present baseline characteristics, level and prevalence of fatigue, level of aerobic capacity and depression. To test the difference in baseline characteristics between the patients who completed CR and the patient who did not, an independent t-test and χ2 test were performed.
To assess the changes in prevalence of fatigue during and after CR, a χ2 test was performed. To investigate the changes in the level of fatigue during and after CR, a generalized estimated equation (GEE) model was performed with fatigue as dependent outcome variable and time as categorical predicator. A GEE model corrects for missing values and the dependency for observation within a subject is taken into account (20). In case time effects in fatigue were found, a second GEE model was performed to test whether the changes in fatigue were mediated by aerobic capacity and depression. In this second model, fatigue was used as dependent outcome variable and time, aerobic capacity and depression were used as predictors. All models were adjusted for age, gender and cardiac diagnosis. Since the time between the measurements was not equal, an autoregressive structure was used in all models. The outcomes of the GEE analysis are regression coefficients (B), which indicate the change in the dependent variable that is associated with a 1 unit change in the predictor variable.
To examine the difference in baseline characteristics between patients who were severely fatigued at follow-up and those who were not, a post-hoc independent t-test and χ2 test were performed. SPSS version 20 was used for data analysis. An overall 2-sided α of 0.05 was set for all analyses.
RESULTS
Patients
The majority of patients were men (79%) and mean age was 56.6 years (Table I). The main diagnosis for referral to CR was myocardial infarction (75%). The mean number of training sessions was 22 (Table I). There were no differences in baseline characteristics between the 121 patients who completed the rehabilitation programme and the 35 patients who did not complete the programme and who were excluded from analysis.
|
Table I. Baseline characteristics of the study population (n = 121) |
|
|
Baseline characteristics |
|
|
Men, n (%) |
96 (79) |
|
Diagnosis, n (%) Myocardial infarction Angina pectoris |
91 (75) 30 (25) |
|
Age, years, mean (SD) |
56.6 (9.1) |
|
BMI, kg/m2, mean (SD) |
28.1 (5.8) |
|
Waist circumference, cm, mean (SD) |
100.9 (13.8) |
|
Systolic blood pressure, mmHg, mean (SD) |
133.9 (19.4) |
|
Diastolic blood pressure, mmHg, mean (SD) |
79.5 (11.4) |
|
Number of training sessions |
22 (4.6) |
|
Smoking, n (%) |
29 (25) |
|
Diabetes, n (%) |
17 (14) |
|
Medication, n (%) Aspirin Statin Beta blocker ACE inhibitor ADP antagonist |
116 (95.9) 118 (97.5) 101 (83.5) 79 (65.3) 99 (81.8) |
|
SD: standard deviation; ACE: angiotensin-converting enzyme; ADP: adenosine diphosphate; BMI: body mass index. |
|
Fatigue
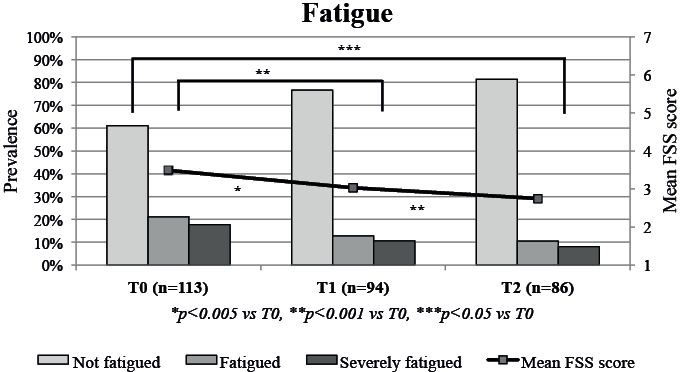
Patients with AP (mean FSS 4.05 (standard deviation (SD) 1.59)) were significantly more fatigued at baseline than patients with MI (mean FSS 3.31 (SD 1.38), p = 0.024). There was no difference at baseline in prevalence of fatigued patients between patients with AP (21.4% fatigued, 28.6% severely fatigued) and MI (21.2% fatigued, 14.1% severely fatigued, p = 0.131). The mean level of fatigue significantly decreased in the total study population from 3.49 (SD 1.5) at baseline to 3.03 (SD 1.3) post-rehabilitation (B = –0.417 p = 0.002) and to 2.75 (SD 1.4) at follow-up (B = –0.678, p < 0.001 vs T0) (Table II and Fig. 2 (line)). At baseline, 21.2% of the patients were classified as fatigued (mid-grey) and 17.7% as severely fatigued (dark-grey). The prevalence of fatigued patients decreased to 12.8% post-rehabilitation (p < 0.001) and to 10.5% at follow-up (p = 0.011 vs T0, p < 0.001 vs T1). The number of severely fatigued patients decreased to 10.6% post-rehabilitation (p < 0.001) and to 8.1% at follow-up (p = 0.011 vs T0, p < 0.001 vs T1) (Fig. 2). Those patients who were classified as severely fatigued at follow-up, were also severely fatigued prior to CR. Therefore, the fatigued and non-fatigued patients did not change into severely fatigued patients.
|
Table II. Generalized estimating equation model for changes in fatigue scores during and after cardiac rehabilitation |
|||
|
|
B |
95% CI |
p-value |
|
T0–T1 |
–0.42 |
–0.68; –0.15 |
0.002 |
|
T0–T2 |
–0.68 |
–1.00; –0.36 |
< 0.001 |
|
T1–T2 |
–0.26 |
–0.51; –0.01 |
0.042 |
|
Measurements taken: T0 = baseline; T1 = after rehabilitation; T2 = at 1-year follow-up. T0: n = 113, T1: n = 94, T2: n = 86. 95% CI: 95% confidence interval; B: unstandardized regression coefficient. |
|||
Post-hoc analysis revealed differences in baseline characteristics between patients who were severely fatigued at follow-up and those who were not. The severely fatigued group consisted of significantly more patients with diabetes and women compared with fatigued and non-fatigued patients (Table III). At follow-up, the patients with severe fatigue walked a shorter distance on 6MWT; 449.4 m (SD 109.66) compared with 613.9 m (SD 84.8) for those who were not severely fatigued (p = 0.026). In addition, the severely fatigued patients showed significantly more depressive symptoms (66.7%), compared with 16.7% in mildly fatigued patients and 3.3% in non-fatigued patients.
|
Table III. Difference in baseline characteristics between severely fatigued patients and fatigued and non-fatigued patients at follow-up |
|||
|
|
Severely fatigued patients |
Fatigued and non-fatigued patients |
p-value |
|
Men, % |
42.9 |
83.5 |
0.010 |
|
Diagnosis, % Myocardial infarction Angina pectoris |
71.4 28.6 |
75.9 24.1 |
0.790 |
|
Age, years, mean (SD) |
58.4 (7.6) |
57.7 (9.3) |
0.845 |
|
BMI, kg/m2, mean (SD) |
30.6 (5.69) |
28.1 (6.5) |
0.328 |
|
Waist circumference, cm, mean (SD) |
104.1 (19.2) |
101.0 (9.8) |
0.688 |
|
Systolic blood pressure, mmHg, mean (SD) |
72.1 (14.1) |
80.6 (10.6) |
0.054 |
|
Diastolic blood pressure, mmHg, mean (SD) |
132.9 (25.3) |
135.9 (19.5) |
0.701 |
|
Smoking, % |
14.3 |
23.0 |
0.597 |
|
Diabetes, % |
57.1 |
10.1 |
0.001 |
|
SD: standard deviation; BMI: body mass index. |
|||
Aerobic capacity and depression
The distance walked during the 6MWT increased by 7.1%, from 581 m (SD 81) at baseline to 622 m (SD 87) at post-rehabilitation (B = 36.59, p < 0.001). At follow-up, the distance walked decreased by 3.4% to 601 m (SD 93) (B = –18.34, p = 0.011 vs T1) (Table IV), but was still higher compared with baseline (B = 18.25, p = 0.006).
|
Table IV. Generalized estimated equation (GEE) model for changes in 6-min walk test (6MWT) and depression during and after cardiac rehabilitation |
|||
|
|
B |
95% CI |
p-value |
|
6MWT |
|
|
|
|
T0–T1 |
36.59 |
22.16; 51.02 |
< 0.001 |
|
T0–T2 |
18.25 |
5.34; 31.16 |
0.006 |
|
T1–T2 |
–18.34 |
–32.55; 4.12 |
0.011 |
|
Depression |
|
|
|
|
T0–T1 |
–0.56 |
–1.06; –0.07 |
0.026 |
|
T0–T2 |
–0.77 |
–1.34; –0.21 |
0.008 |
|
T1–T2 |
–0.21 |
–0.74; 0.32 |
0.440 |
|
Associations |
|
|
|
|
6MWT and fatigue |
–0.002 |
–0.005; 0.000 |
0.030 |
|
Depression and fatigue |
0.203 |
0.145; 0.260 |
< 0.001 |
|
Measurements taken: T0 = baseline; T1 = after rehabilitation; T2 = at 1-year follow-up. T0: n = 99, T1: n = 70, T2: n = 67. 95% CI: 95% confidence interval; B: unstandardized regression coefficient. |
|||
The mean level of depression decreased from 3.57 (SD 3.6) at baseline to 2.87 (SD 2.9) at post-rehabilitation (B = –0.56, p = 0.026). This lower level of depression was maintained at follow-up (2.67 ± 3.1, B = –0.770, p = 0.008 vs T0) (Table IV).
An association was found between distance walked during 6MWT and fatigue (B = –0.002, p = 0.030) when adjusted for depression. A mean increase in 6MWT of 1 m was associated with a mean decrease of 0.002 in the fatigue score (Table IV). An association was also found between depression and changes in fatigue (B = 0.203, p < 0.001) (Table IV). A mean decrease of 1 in the score on the depression subscale was associated with a mean decrease of 0.203 in the fatigue score.
DISCUSSION
This study estimated fatigue during and after CR. The level and the prevalence of fatigue both decreased. However, one year after the start of rehabilitation, the prevalence of severely fatigued patients remained high. In this group of severely fatigued patients, the prevalence of depressive symptoms was also high. As hypothesized, aerobic capacity was associated with reductions in fatigue scores, even after correction for depressive symptoms.
Our finding of a mean baseline level of fatigue of 3.49 indicates that, on average, this patient group is not fatigued. However, since the mean FSS score in healthy populations is 3.00±1.08 (12), the level of fatigue in patients with CAD is higher at baseline. After rehabilitation and at follow-up, FSS scores were equal to scores in the healthy population.
Examination of the prevalence of fatigue showed that the findings were encouraging for the fatigued patients, but are still a cause of concern for the severely fatigued patients. In a healthy population, the prevalence of fatigued individuals (including severely fatigued patients) is 18% (12). While the prevalence in patients with CAD was higher than this at baseline, this difference was no longer present at follow-up. In contrast, the prevalence of severely fatigued patients in the current study was higher than the figure of 3.5% seen in the healthy population (12), not only at baseline, but also after rehabilitation and at follow-up. The current CR programme thus seems inadequate for reducing fatigue in this subgroup of severely fatigued patients. Since fatigue might negatively influence physical and mental capacity and thus quality of life (6), it is important to know whether CR can be optimized to reduce fatigue in this group. The most striking factor shown by the characteristics of this subgroup was the very high occurrence of depressive symptoms at follow-up. Since one of the main symptoms of depression is fatigue or loss of energy (21), an extra intervention that focuses on the treatment of depression is likely to be beneficial.
To the authors’ knowledge, no previous studies have explored levels of fatigue after CR in patients with CAD. However, a treatment effect of CR on vital exhaustion was found by one study (5). The features of vital exhaustion are fatigue and loss of energy (22). Another study reported a decrease in fatigue from baseline to 4 months and 2 years after infarction on the Multidimensional Fatigue Inventory scale (6). Since the patients in this second study did not participate in CR, it seems that the improvements in fatigue reported in our study cannot completely be attributed to CR. It should be noted, however, that while 48% of the patients in the second study still reported fatigue at 4 months and at 2 years after a myocardial infarction (6), this was only 23% in our study after participation in CR.
Besides a direct result of CR on fatigue, CR could also indirectly lead to improvements in fatigue. According to the results of previous studies, our study demonstrated a significant increase in aerobic capacity during CR. This increase has been shown to improve a patient’s ability to perform activities of daily living, including work and leisure activities (23). These improvements influence the patient’s psychological condition and thus improve their quality of life (23). A small decline in aerobic capacity was seen at follow-up; however, the distance walked was still higher than baseline. These results are in line with a previous study (24). Also consistent with our hypothesis was the finding of a positive association between aerobic capacity and changes in fatigue. To achieve a level of fatigue equal to that of healthy individuals, patients with CAD had to reduce their FSS score on average by 0.5. Based on the model, patients would therefore have had to increase the distance walked in 6MWT on average by 250 m. Since the mean improvement was only 33 m, the reduction in fatigue was also clearly influenced by other factors.
Previous research has indicated a strong, positive association between scores on the HADS depression subscale and fatigue scores (5). The prevalence of depression is high in patients with CAD and overlaps with fatigue (6). In line with these findings, the results of our study showed that changes in fatigue were significantly associated not only with aerobic capacity, but also with depression. A reduction in depression was associated with a decline in fatigue. Whereas aerobic capacity was only a weak mediator for changes in fatigue, the decline in fatigue during and after CR seems to have been caused mainly by a reduction in depression. This again underlines the importance of focusing on depressive symptoms in the group of severely fatigued patients for whom CR does not seem to be effective in terms of reducing fatigue.
Further research is required into more causes of fatigue and severe fatigue. Fatigue is likely to be influenced not only by the patient’s disease, but also by factors such as socio-economic factors and comorbidities (6). It is also important to identify patients with severe fatigue at an early stage of the rehabilitation programme so that other additional fatigue-relieving strategies can be provided for this group.
Study limitations
This study has some limitations. First, since there was no control group, the effects of CR on fatigue remain unclear. The changes in fatigue could be attributed to time rather than to exercise-based CR. Ideally, future research should study the effect of CR on fatigue in a randomized controlled trial. However, since CR is currently seen as standard care, it would be unethical to exclude patients from CR.
A second limitation is our use of the 6MWT to assess aerobic capacity. The gold standard for determining aerobic capacity is measuring oxygen consumption during cardiopulmonary exercise testing. This test could, however, not be performed for logistic reasons. Instead, we used the 6MWT, a test that is often recommended in patients undergoing CR. It is well known from previous research that the 6MWT is a valid instrument to estimate aerobic capacity in patients undergoing CR (16). Nevertheless, previous research has also shown that there is a learning effect for repeated 6MWTs, which can also result in improvements (16). We attempted to reduce this effect by performing a practice session at baseline. Despite this, patients who walk only a short distance in the 6MWT at baseline have more scope for improvement than those who walk a greater distance, in whom a “ceiling effect” may therefore occur (16). A final limitation is that, since someone’s experience of fatigue may differ during the day, their answers may depend on when the questionnaire was completed (6).
Conclusion
This is the first study, to our knowledge, which investigated the level and prevalence of fatigue in patients with CAD during and after CR. Levels of fatigue were improved both post-rehabilitation and at follow-up. On average, patients obtained levels of fatigue equal to those in a healthy population. However, after rehabilitation the prevalence of severe fatigue remained higher in patients with CAD than in healthy individuals. This suggests that the current CR programme might be inadequate for these patients in terms of fatigue. Although aerobic capacity was found to be associated with a decline in fatigue, the association was weak. Since a stronger association was found between fatigue and depression, interventions that focus on reducing depression might also have a positive influence on reducing fatigue in patients with CAD. Patients with severe fatigue should be identified in an early stage of rehabilitation so that additional programmes to relieve fatigue can be provided.
REFERENCES

