Bridget Hill, Grad Dip (Physio)1,2, Gavin Williams, PhD2, John Olver, MBBS, MD (Melb)2 and Andrea Bialocerkowski, PhD1
From the 1Menzies Health Institute, Griffith University, Queensland and 2Epworth Monash Rehabilitation Medicine Unit Epworth HealthCare, Melbourne, Victoria, Australia
OBJECTIVE: To identify the range of activities limited following adult traumatic brachial plexus injury and triangulate these with existing patient-reported outcome measures identified from the literature.
DESIGN: A qualitative cross-sectional design.
SUBJECTS: Adults with traumatic brachial plexus injury and expert clinicians.
METHODS: Using an International Classification of Functioning, Disability and Health (ICF) framework, participants identified day-to-day activities that are limited following traumatic brachial plexus injury. Two independent reviewers classified all reported activities into the Comprehensive ICF Core Set of Hand Conditions (CCS-HC) activity domains. Reported activities were triangulated with patient-reported outcome measures identified from the brachial plexus injury literature.
RESULTS: Fifty-one participants (21 adults with brachial plexus injury, 30 expert clinicians) generated a total of 522 items. The inter-rater reliability for classification to CCS-HC domains was excellent (k = 0.94, 95% confidence interval (95% CI) 0.92–0.96). Activities reported by patients and clinicians represented all 29 CCS-CH activity domains. Five activities (2%) could not be classified to any ICF domain. Fifteen CCS-HC activity domains were represented in the Disabilities of Arm, Shoulder and Hand (DASH) and ABILHAND, 2 measures currently used in the brachial plexus injury literature.
CONCLUSION: Adults with a brachial plexus injury report a range of activities that are limited following injury, and are under-represented in currently used patient-reported outcome measures. The activities reported in this study could be used to inform the development of a new brachial plexus injury targeted questionnaire.
Key words: brachial plexus neuropathies; ICF Core Set; activity limitation.
J Rehabil Med 2015; 47: 00–00
Correspondence address: Bridget Hill, Menzies Health Institute, Griffith University, Queensland, Australia. E-mail: bridget.hill@epworth.org.au
Accepted Dec 10, 2014; Epub ahead of print Mar 6, 2015
Introduction
Injury to the brachial plexus, which typically occurs in young males after motorbike accidents, ranges markedly in severity (1, 2). People with a brachial plexus injury (BPI) present with a very wide spectrum of disability and report on-going dissatisfaction with the day-to-day use of their arm (3–5). Psychosocial adjustment issues are often reported, together with poorer quality of life and an inability to return to pre-morbid work and leisure activities. Whilst some may regain almost full use of their arm, others may retain the use of their hand but are unable to move or place their arm, thus rendering the hand virtually useless. Others may use their arm only as a passive stabilizer (2). Treatment for BPI is focused on improving the use of the affected limb. Individuals often undergo reconstructive surgeries and rehabilitation over many months or years, and the burden on family and society can be considerable (1, 3, 5, 6). Therefore, determining the most cost-effective form of treatment that results in the significant change over time that is important and meaningful to the injured person is paramount.
There is an increasing body of evidence that advances in microsurgical techniques result in increased strength of individual muscles and therefore movement at individual joints (6, 7). There is little evidence, however, that strength gains at a muscle level translate into better ability to use the arm to perform day-to-day tasks that require complex positioning and holding of multiple joints in space (8, 9). It is important to assess all factors that impact on outcome following traumatic BPI, including psychological response to injury, pain and quality of life. Multi-dimensional measures have been developed to assess factors that impact on outcome (10–12). For example, the Disabilities of Arm, Shoulder and Hand (DASH) (10) is the most commonly used patient-reported outcome measure (PROM) following BPI (13). Designed as a measure of physical function and symptoms, the DASH contains items that assess pain and sleep, both impairments, together with activity limitations and participation restrictions (14). However, a multi-dimensional measure on its own cannot determine which factor is attributable for the measured change. Without uni-dimensional psychometrically robust measures that are specific to the injured limb, which contain items that reflect the underlying disorder, clinicians cannot be sure that any measured change has occurred as a direct result of therapeutic management.
In complex conditions such as BPI, how the arm is used day-to-day is the key to long-term outcome and overall satisfaction (3–5). Patient-reported outcome measures (i.e. questionnaires) are increasingly being used clinically to evaluate outcome from the perspective of the injured individual. However, a systematic review of BPI literature undertaken by the authors found questionnaires that assess activity, as defined by the ICF, are infrequently used to evaluate day-to-day arm use in this population (13). Most questionnaires identified (n = 18) were designed for a specific research or clinical purpose, with no psychometric data to enable their quality to be evaluated. The high prevalence of these site-specific questionnaires may reflect the lack of a BPI-specific uni-dimensional targeted questionnaire that accurately measures day-to-day activity from the individual’s perspective.
Two questionnaires with published psychometric data for people with upper limb disorders were identified in the BPI literature (13), the ABILHAND (15) and the DASH (10). The DASH, as a measure of physical symptoms and disability, apportions 54% of the total score to items that assess activity. Other items address issues related to symptoms such as pain, sleeping and strength (16, 17). As a consequence, it is entirely feasible that a person with traumatic BPI may meet the minimal clinically important difference for the DASH (>15 points) by reporting a decrease in pain intensity, sleeping better and increasing their social activities while experiencing no neurological improvement in their arm (18). Furthermore, both the DASH and the ABILHAND evaluate performance regardless of how the activity is performed. Thus, for a unilateral arm injury, such as BPI, improved scores over time may reflect an individual’s ability to compensate by using other parts of their body, and/or adapt to their injury by changing hand dominance in the absence of any physical recovery in the injured upper limb (UL).
To date there is no empirical evidence as to which day-to-day activities are meaningful and relevant to this population as they regain use of their arm and whether these activities are reflected in the questionnaires currently being used to evaluate outcome. This study, therefore, addressed this gap by having 2 aims:
• To identify the range of day-to-day activities that are limited in adults following traumatic BPI, using the ICF as a framework (aim 1).
• To compare activities reported by adults with a traumatic BPI with those identified by: (i) clinical experts; (ii) items contained in site-specific questionnaires identified in the BPI literature; (iii) items contained in the psychometrically evaluated questionnaires identified in the BPI literature (i.e. the DASH and ABILHAND) (aim 2).
METHODS
The study received full ethics approval from the University of Western Sydney, Australia (H8616). All participants provided written informed consent.
Phase 1
A cross-sectional design, using a qualitative deductive content analysis methodology, was used to address aim 1.
Inclusion criteria
Purposeful sampling with maximum variation was used to select information-rich participants based on their knowledge of traumatic BPI (19). Adults diagnosed with traumatic BPI who were managed in 2 treatment centres in Melbourne, Australia, were invited to participate. Participants were invited regardless of injury level, time post-injury, or surgical intervention to ensure identification of the full range of activities undertaken by this demographic. BPI was confirmed by electromyography, magnetic resonance imaging, computerized tomography, myelogram, intra-operative or clinical findings. Participants were excluded if they had an isolated upper limb peripheral nerve lesion, concurrent traumatic brain injury (defined as a Glasgow coma score of ≤ 13 at the time of injury), were unable to undertake a medical examination or were unable to read and write treatment goals in English without an interpreter.
A cross-section of clinical experts was recruited, based on their experience in managing both BPI and a variety of upper limb disorders. Given the relatively small numbers of therapists who have extensive experience in managing BPI, experts in related fields were also recruited, in particular neurological and trauma therapists. All had experience in the day-to-day treatment of adults with BPI. Experts recruited included physiotherapists, occupational therapists, (some of whom specialized in hand therapy), academics, plastic surgeons who performed brachial plexus reconstructions and rehabilitation physicians. All had a minimum of 5 years clinical experience. Participants were identified using multiple sources, including publically available websites, departmental heads of rehabilitation centres and universities in Victoria, Australia. Snowballing techniques were used to identify additional participants who met the inclusion criteria, irrespective of their geographical location of practice (20).
Data collection
All participants attended either a nominal group session (21, 22) or a one-to-one interview based on their personal preference or availability to attend a nominal group. Adults with a traumatic BPI and clinical experts did not attend the same nominal group session to maintain patient confidentiality and so responses were not influenced by the possible presence of their treating clinician. Participants were asked to answer the key question: “Which activities best represent the key day-to-day use of the arm following brachial plexus injury?” They were provided with the specific examples listed in the ICF manual for each of the ICF domains: d430 – Lifting and carrying, d440 – Fine hand use, d445 – Hand and arm use, d510–d560 – Self-care, and d630–d649 – Household tasks, to inform item generation (23). For the purpose of this study, activity was defined as “discrete physical actions or tasks, undertaken by the individual” (23). Participants were requested to focus on activities that reflected the whole spectrum of regular day-to-day activities undertaken by the arm and hand. Where possible each activity should consist of no more than 1 task, be relevant to adult males and females and unlikely to become redundant over time because of changes in technology. Each group session and individual interview was audio-taped. Activities were transcribed into Microsoft Excel spreadsheets (Excel Mac 2008) in real time.
Data analyses
Data analyses were based on deductive content analysis, which is the subjective interpretation of qualitative data through the systematic coding and identification of themes, based on an underlying framework (19). Data from patients and clinicians were analysed separately. The Comprehensive ICF Core Set for Hand Conditions (CCS-HC) underpinned analyses (24). It was designed to describe functioning and disability of patients with hand conditions and provides a standard of aspects that should be considered for assessment and reporting in individuals with hand and other upper limb conditions. The CCS-HC consists of 117 ICF domains deemed to be specific to the hand, of which 38 are specific to the ICF component of Activity and Participation (23). After each nominal group session and interview, reported activities were reviewed by 2 independent researchers. Following removal of all duplicates and similar activities were combined (e.g. turn a doorknob/turn a door handle), the remaining items were assigned to a CCS-HC activity domain based on the linking rules by Cieza et al. (25, 26). For the purposes of this study, items were classified as either activity or participation, based on the definition used by Eyssen (27) and Jette (28), i.e. combinations of multiple activities that relate to a life role are participation restrictions, activities are simple discrete tasks that can be carried out alone. Table I outlines the 9 participation-specific ICF domains as determined by the authors. All items assigned to these 9 domains were excluded from the analyses. In cases of disagreement, a third researcher resolved the discrepancy. Kappa coefficients and 95% confidence intervals were calculated to assess the inter-rater reliability of classification of the items to the CCS-HC activity domains and were interpreted according to Landis and Koch, with moderate agreement > 0.60, substantial agreement > 0.61–0.8 and excellent agreement > 0.81–0.99 (20). Data collection continued until saturation occurred, that is when no new items were generated.
|
Table I. Comprehensive ICF Core Set – Hand Conditions domains specific to participation |
|
|
ICF code |
CCS-HC domaina |
|
d230 |
Carrying out daily routine |
|
d470 |
Using transportation |
|
d570 |
Looking after ones health |
|
d620 |
Acquisition of goods and services |
|
d660 |
Assisting others |
|
d7 |
Interpersonal interactions and relationships |
|
d810–d850 |
Education |
|
d840–d859 |
Work and employment |
|
d920 |
Recreation and leisure |
|
aActivities classified to these CCS-HC domains were excluded from this study. CCS-HC: Comprehensive ICF Core Set for Hand Conditions. |
|
Phase 2
All items contained within the 20 patient-reported outcome measures (18 site-specific and 2 psychometrically evaluated questionnaires) identified in the systematic review of the BPI literature (13) were assigned to a CCS-HC activity domain by 2 independent researchers using the same methodology as described above. Where an item covered more than 1 activity classification was based on the meaningful concept within the item, e.g. “Make a bed” is housework (d640) (14). A descriptive comparison was then undertaken between CCS-HC domains reported by adults with traumatic BPI, clinical experts, the site-specific and psychometrically-evaluated questionnaires identified in the BPI literature (13).
RESULTS
Participants
Invitations were sent to 30 adults with traumatic BPI, 21 of whom participated in this study. Ninety percent of participants were males. The mean age of participants was 38 years (range 26–57 years) and they were a mean of 129 weeks post-injury (range 37–306 weeks). Participants represented a wide range of brachial plexus trauma, from loss of only the posterior cord to complete avulsion of C5–T1. Those who declined to take part in this study had a similar range of clinical presentation; their mean age was 32 years (range 20–56 years) and they were a mean of 157 weeks post-injury (range 68–246 weeks).
Sixty-three invitations were sent to clinical experts, and 30 (22 females and 8 males) participated in this study: 20 physiotherapists, 8 occupational therapists, (4 of whom were hand therapists), 1 plastic surgeon who regularly performs brachial plexus reconstruction surgery, and 1 rehabilitation physician. The mean age of the clinical experts was 37 years (range 26–53 years), and the experts had a mean of 12 years of experience in their chosen speciality field (range 5–31 years). Half of the participants had post entry-level qualifications in their discipline.
Aim 1: Reported activities
Fig. 1 demonstrates the flow of reported activities through the study. Adults with traumatic BPI identified 416 activities. Following the removal of duplicate items, items representing participation and similar activities were combined, 197 activities were classified into 28 of the 29 CCS-HC activity domains (Table II). No activities were identified in the CCS-HC domain d4403 – Releasing. Eleven items (2%) could not be classified into a CCS-HC activity domain (Table III). Of these, half were classified into a non-CCS-HC ICF domain of “d335 – Producing nonverbal messages” (i.e. conveying meaning by movements of the arm and hand and postures, such as embracing to indicate affection). The remainder were unclassifiable by the ICF (Table III).
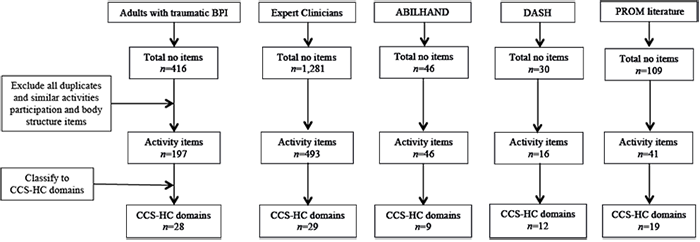
Fig. 1. Flow of activities through the project. DASH: Disabilities of the Arm, Shoulder and Hand; CCS-HC: Comprehensive ICF Core Set for Hand Conditions; BPI: brachial plexus injury.
Expert clinicians identified 1,281 activities (Fig. 1). After the removal of duplicates, participation items, and consolidation of similar items, 493 activities remained, which were assigned to all 29 CCS-HC activity domains (Table II). Expert clinicians identified all the items from the ICF domain d335 (Producing non-verbal messages) and the same unclassifiable items as adults with a traumatic BPI (Table III). When the activities generated by adults with a traumatic BPI and clinical experts were combined 522 different items were identified, representing all CCS-HC domains. Adults with a traumatic BPI reported 19 additional items not identified by expert clinicians. The inter-rater reliability of the classification of the reported items to CCS-HC activity domains was excellent (k = 0.94, 95% CI 0.92–0.96) (20). The independent researchers had 100% agreement on allocation of 19 activities reported only by adults with a traumatic BPI (k = 1.0).
Aim 2: Triangulation with existing questionnaires
Items contained within the ABILHAND and DASH were classified into 14 of the CCS-HC activity domains (Table II), and neither questionnaire contained activities, classified to domain “d335 – Producing non-verbal messages”. Items contained in the 18 site-specific questionnaires were classified to 19 of the 29 CCS-HC activity domains (Table II). They also contained 4 of the 5 unclassifiable items gained from adults with BPI (Table III), but no items from d335.
|
Table II. Comprehensive ICF Core set – Hand Condition activity domains |
||||||
|
ICF code |
CCS-HC domain |
Patient |
Expert clinician |
ABILHAND DASH |
PROM Literature |
Distal arm use, whole arm use |
|
d170 |
Writing |
* |
* |
* |
* |
Distal arm |
|
d3600 |
Using communication devices and techniques |
* |
* |
* |
Whole arm |
|
|
d410 |
Changing basic body position |
* |
* |
Whole arm |
||
|
d420 |
Transferring oneself |
* |
* |
Whole arm |
||
|
d4300 |
Lifting and carrying objects |
* |
* |
* |
* |
Whole arm |
|
d4440 |
Picking up |
* |
* |
* |
* |
Distal arm |
|
d4401 |
Grasping |
* |
* |
* |
* |
Distal arm |
|
d4402 |
Manipulating |
* |
* |
* |
* |
Distal arm |
|
d4403 |
Releasing |
* |
Distal arm |
|||
|
d4408 |
Fine hand use, other specified |
* |
* |
Distal arm |
||
|
d4450 |
Pulling |
* |
* |
Whole arm |
||
|
d4451 |
Pushing |
* |
* |
* |
* |
Whole arm |
|
d4452 |
Reaching |
* |
* |
* |
* |
Whole arm |
|
d4453 |
Turning or twisting the hands and arms |
* |
* |
* |
* |
Distal arm |
|
d4454 |
Throwing |
* |
* |
Whole arm |
||
|
d4455 |
Catching |
* |
* |
Whole arm |
||
|
d4458 |
Hand and arm use, other specified |
* |
* |
Whole arm |
||
|
d455 |
Moving around |
* |
* |
Whole arm |
||
|
d465 |
Moving around using equipment |
* |
* |
Whole arm |
||
|
d475 |
Driving |
* |
* |
* |
Whole arm |
|
|
d510 |
Washing oneself |
* |
* |
* |
* |
Whole arm |
|
d520 |
Caring for body parts |
* |
* |
* |
* |
Whole arm |
|
d530 |
Toileting |
* |
* |
* |
Whole arm |
|
|
d540 |
Dressing |
* |
* |
* |
* |
Whole arm |
|
d550 |
Eating |
* |
* |
* |
Whole arm |
|
|
d560 |
Drinking |
* |
* |
* |
Whole arm |
|
|
d630 |
Preparing meals |
* |
* |
* |
* |
Whole arm |
|
d640 |
Doing housework |
* |
* |
* |
* |
Whole arm |
|
d650 |
Caring for household objects |
* |
* |
* |
* |
Whole arm |
|
Total number of CCS-HC domains |
28 |
29 |
14 |
19 |
||
|
CCS-HC: Comprehensive ICF Core Set Hand Conditions; ICF: International Classification of Functioning Disability and Health; DASH: Disability of the Arm, Shoulder and Hand; PROM: patient-reported outcome measure identified in the brachial plexus injury (BPI) literature, with no known psychometric properties. |
||||||
|
Table III. Identified activities unable to be assigned to a Comprehensive Core set – Hand Condition activity domain |
|||||||
|
Activity |
ICF code |
ICF domain |
Patient |
Expert clinician |
ABILHAND |
DASH |
PROM literature |
|
Maintain control of the affected arm so not required to wear a sling |
NA |
* |
* |
* |
|||
|
Stabilizing an object with the affected arm to manipulate with the unaffected, i.e. using the arm primarily as a paperweight |
NA |
* |
* |
* |
|||
|
Hold 1 object while doing another activity |
NA |
* |
* |
* |
|||
|
Holding an object between upper arm and chest (brachiothoracic grasp) |
NA |
* |
* |
* |
|||
|
Roll over when sleeping without having to wake to move affected arm |
NA |
* |
* |
||||
|
Gesticulate with your hands for communication |
d335 |
Producing non-verbal messages |
* |
* |
|||
|
Shake hands |
d335 |
Producing non-verbal messages |
* |
* |
|||
|
Hold hands |
d335 |
Producing non-verbal messages |
* |
* |
|||
|
Hug partner or children |
d335 |
Producing non-verbal messages |
* |
* |
|||
|
Waving to somebody |
d335 |
Producing non-verbal messages |
* |
* |
|||
|
Clapping |
d335 |
Producing non-verbal messages |
* |
* |
|||
|
ICF: International Classification of Functioning Disability and Health; DASH: Disability of the Arm, Shoulder and Hand; PROM: patient-reported outcome measure identified in the brachial plexus injury (BPI) literature, with no known psychometric properties. |
|||||||
DISCUSSION
This study provides empirical evidence that traumatic BPI affects a wide variety of frequently undertaken day-to-day activities, as evidenced by the large number of activities reported (n = 522) that were classified to all CCS-HC activity domains (n = 29). There was very close agreement between adults with a traumatic BPI and clinical experts. Fifteen of the 29 CCS-HC domains (Table II) were not represented in the psychometrically evaluated questionnaires currently used in the literature to evaluate this population (ABILHAND and DASH) (13). It is likely, therefore, that these measures do not fully represent the spectrum of day-to-day use of the arm demonstrated by this population (20). While the DASH is being used increasingly in BPI research, the results of this study suggest that the face and content validity may be compromised in this population. Moreover, as a multi-dimensional questionnaire, the summed DASH score should be viewed with considerable caution, as change could be related to a range of non-physical factors while people’s ability to actually use their limb day-to-day as a direct consequence of their clinical management remains very limited (12, 18).
BPI may affect the whole upper limb, which impacts all joints required to place and hold the hand for day-to-day use. While titled a Hand Core Set, the activities classified to CCS-HC domains require distal and whole arm use (Table II) (29, 30). However, adults with traumatic BPI and expert clinicians identified a small number of activities (n = 6) classified to an ICF domain (d335 – Producing nonverbal messages) not included in the CCS-HC. The way we use our hands to interact with our environment is unique to each individual and influenced by beliefs and expectations (31). Adults with a traumatic BPI reported that not being able to communicate with family and friends using arm and hand gestures altered their opinion of themselves as individuals. It could be argued that these movements or gestures be defined as participation and therefore eliminated. However, participation is an abstract concept demonstrated at a community and society level that relates to a specific life role (27). In contrast, an activity is an observable phenomenon at an individual level (32). Given that participants in this study described these tasks as discreet activities that impact on their sense of self, they were classified as activities. The importance of these activities has been reported by other authors and represents a key aspect of arm use that should be assessed following BPI (3–5). Furthermore, these items were not contained in the site-specific or psychometrically evaluated questionnaires and therefore represent an area that has not previously been assessed in this population.
A small number of reported activities (n = 5) could not be classified to any ICF activity domain. All were identified by adults with a traumatic BPI, expert clinicians and were contained in the site-specific questionnaires identified in the BPI literature (Table III) (13). These activities may be termed “low-level”, as they represent the simplest tasks undertaken by the arm, e.g. not constantly requiring a sling or rolling over in bed without waking to re-position the arm. As the growing consensus for reanimation following BPI is to first address the shoulder and elbow (7, 33), these activities are some of the first that may be regained following reconstructive microsurgery. Thus they are important to assess. Indeed, for the individual with a flail limb, they may represent the only improvement in the use of their arm over time (34). None of the “low-level” activities were contained in the psychometrically-evaluated questionnaires identified in the BPI literature (Table III). Without items at either end of the spectrum of ability, outcome measures cannot comprehensively evaluate the underlying construct. Floor or ceiling effects may occur, and important changes that have resulted following costly surgical and therapeutic intervention may not be identifiable (20). These “low level” activities are rarely, if ever, included in any patient-reported outcome measure. To the best of our knowledge only 1 new outcome measure, the Arm Activity Measure (ArMA), which was designed to measure active and passive function following stroke, includes items that address this level of ability (35).
Study limitations
A possible limitation of this study is the relatively small number of adults with traumatic BPI. However, those recruited had a wide cross-section of BPI and time post-injury, and represented most of the clinical presentations of this diagnosis. Although the ratio of males to females was 1:10, this ratio is consistent with the epidemiology of BPI (1, 36). While the recruitment strategy targeted a diverse sample of expert clinicians, the sample size of professional groups was dissimilar; thus, the yield of reported items may have been influenced. However, this is unlikely given the large number of items generated, across all CCS-HC domains (II) and the very close relationship between items identified by adults with a traumatic BPI and the expert clinicians. Recruitment of additional expert clinicians could have been extended outside Victoria, Australia; however, as data collection continued to saturation it is unlikely that additional activities would have been identified.
Two different methods of data collection were utilized, the group sessions and 1:1 interviews. While other methods of qualitative data collection could have been used, it was felt that these methods offered the greatest opportunity for activity generation due to the brainstorming effects of the nominal group technique, while acknowledging the geographical and time constraints of working clinicians (37). In addition, the large yield reported would seem to indicate that this strategy was successful.
The upper limb performs activities that are influenced by multiple factors, including hand dominance and whether uni- or bi-manual skills are required (38, 39). BPI is a unilateral upper limb injury where dominance may be transferred and a wide variety of compensatory techniques used to carry out day-to-day tasks (40). However, as the aim of this project was to identify activities that may be limited following BPI, tasks were not separated along these lines. Further work is required to determine the influence of hand dominance and other factors on performance following BPI.
Conclusion
Using the CCS-HC framework to compare multiple sets of information from a variety of sources, adults with traumatic BPIs and clinical experts identified a large number of activities that are limited following injury across all CCS-HC domains and levels of ability. The face and content validity of the ABILHAND and DASH appear to be compromised as neither contains activities that reflect the full spectrum of activities reported, in particular for those with very limited ability to use their arm. Thus, these measures may be not adequately measure change over time in this demographic. The day-to-day activities generated in this study could be used to inform the development of a new patient-reported questionnaire, specific to adult traumatic BPI, which can target all levels of ability.
REFERENCES

