Arjan J. T. Bakkum, MSc1,2, Thomas A. W. Paulson, PhD3,4, Nicolette C. Bishop, PhD3, Victoria L. Goosey-Tolfrey, PhD3,4, Janneke M. Stolwijk-Swüste, MD, PhD5, Dirk J. van Kuppevelt, MD, PhD6, Sonja de Groot, PhD2,4,7 and Thomas W. J. Janssen, PhD1,2,4
From the 1MOVE Research Institute Amsterdam, Faculty of Human Movement Sciences, VU University, 2Amsterdam Rehabilitation Research Centre, Reade, Amsterdam, The Netherlands, 3The Peter Harrison Centre for Disability Sport, School of Sport, Exercise and Health Sciences, Loughborough University, Loughborough, UK, 4European Research Group in Disability Sport (ERGiDS), 5Meander Medical Center, Department of Rehabilitation Medicine, Amersfoort, 6Sint Maartenskliniek, Nijmegen and 7University of Groningen, University Medical Centre Groningen, Center for Human Movement Sciences, Groningen, The Netherlands
OBJECTIVE: To examine the effects of a 16-week exercise programme, using either a hybrid cycle or a handcycle, on cardiovascular disease risk factors in people with spinal cord injury.
PARTICIPANTS: Nineteen individuals with spinal cord injury ≥ 8 years.
DESIGN: Multicentre randomized controlled trial. Both the hybrid cycle group (n = 9) and the handcycle group (n = 10) trained twice a week for 16 weeks on the specific cycle. Outcome measures obtained pre and post the programme were: metabolic syndrome components (waist circumference, systolic and diastolic blood pressure, high-density lipoprotein cholesterol, triglycerides and insulin resistance), inflammatory status (C-reactive protein (CRP), interleukin (IL)-6 and -10), and visceral adiposity (trunk and android fat).
RESULTS: For all outcome measures, there were no significant differences over time between the 2 training groups. Overall significant reductions were found for waist circumference (p = 0.001), diastolic blood pressure (p = 0.03), insulin resistance (p = 0.006), CRP (p = 0.05), IL-6 (p = 0.04), IL-6/IL-10 ratio (p = 0.03), and trunk (p = 0.04) and android (p = 0.02) fat percentage. No significant main effects for time were observed for systolic blood pressure, triglycerides, high-density lipoprotein cholesterol, IL-10, and trunk and android fat mass.
CONCLUSION: The 16-week exercise programme, using either a hybrid cycle or a handcycle, found similar beneficial effects on metabolic syndrome components, inflammatory status and visceral adiposity, indicating that there were no additional benefits of functional electrical stimulation-induced leg exercise over handcycle exercise alone.
Key words: metabolic syndrome; insulin resistance; inflammation; adiposity; paralysis; electric stimulation.
J Rehabil Med 2015; 47: 523–530
Correspondence address: S. de Groot, PhD, Amsterdam Rehabilitation Research Center, Reade, PO Box 58271, NL-1040 HG Amsterdam, The Netherlands. E-mail: s.d.groot@reade.nl
Accepted Nov 19, 2014; Epub ahead of print Maj 11, 2015
INTRODUCTION
With today’s specialized medical care, life expectancy of people with spinal cord injury (SCI) has improved considerably (1). Despite this, mortality rates in people with SCI remain high compared with non-disabled people (2). Cardiovascular disease (CVD) is the leading cause of mortality in the SCI population and is more prevalent in this population than in people without SCI (3). An important contributor for the increased risk of CVD is the fact that several CVD risk factors, such as metabolic syndrome (MetS), chronic low-grade inflammation, and visceral adiposity, are more prevalent in people with SCI than in people without SCI (4–6). The inactive lifestyle observed in many individuals with SCI is strongly associated with higher prevalence of these risk factors (7).
MetS is a condition characterized by clustering of the following CVD risk factors: abdominal obesity, hypertension, high triglycerides (TG), low high-density lipoprotein cholesterol (HDL-C) and insulin resistance (8). The chronic low-grade elevation in plasma concentrations of pro-inflammatory mediators (e.g. C-reactive protein (CRP) and interleukin-6 (IL-6)) is suggested to play an important role in the development of insulin resistance and atherosclerotic plaque (9, 10). Low-grade inflammation is therefore strongly associated with the abnormalities experienced in MetS and the pathophysiology of CVD development (11). Consequently, the suppression of chronic inflammation is an important factor in reducing CVD risk in people with SCI.
Participation in regular exercise has been shown to promote a range of anti-inflammatory benefits in non-disabled individuals, including reduced visceral adiposity (12). However, in SCI, the anti-inflammatory benefits of exercise may be lower due to lower-limb paralysis, and reliance on the relatively small muscle mass activated during upper-body activities (e.g. handcycling) (13). However, cross-sectional analyses have shown positive relationships between chronic inflammation and physical activity levels in this population (5, 14). The circulating cytokine response to upper-body exercise in non-SCI and thoracic SCI is also of a similar magnitude to that observed following lower-body exercise (15). Therefore, increasing physical activity by participating in regular exercise training may provide a protective effect against chronic inflammation and CVD risk in people with long-term SCI.
To date, no intervention studies have examined the effect of long-term upper-body exercise on chronic inflammation in people with SCI. The activation of the paralysed lower-limb musculature via functional electrical stimulation (FES)-evoked cycle training has previously been shown to significantly reduce plasma concentrations of the inflammatory mediators CRP, IL-6 and tumour necrosis factor-alpha (16). The performance of combined FES-evoked leg exercise and voluntary upper-body exercise (i.e. hybrid exercise) has the potential to augment the anti-inflammatory response even further, since a larger muscle mass is activated than during FES-evoked leg exercise or upper-body exercise alone (17).
The potential greater effect of hybrid exercise over handcycle exercise on CVD risk factors requires investigation. Therefore, the aim of this study was to examine the effects of a 16-week exercise programme, using either a hybrid cycle exercise or a handcycle, on MetS components, resting inflammatory status and visceral adiposity in people with long-term SCI.
METHODS
Trial design
The design of the current study (which is part of a larger study) has been described previously by Bakkum et al. (18). Briefly, this study was a 16-week open, explanatory, parallel-group randomized controlled trial (RCT), performed in 2 Dutch rehabilitation centres with a specialized SCI unit. Within each rehabilitation centre, block randomization (fixed block size of 6; allocation ratio 1:1; no stratification) was used to assign participants to either the experimental group (hybrid cycle group) or the control group (handcycle group). A blinded independent researcher provided the allocation in sequentially numbered, opaque, sealed and stapled envelopes. After the included participants completed all baseline measurements, the principal investigator opened the envelopes and allocated the participants to the intervention. Blinding of outcome assessment was ensured for all outcome measures. The sample size calculation was performed on the main outcome measure of the larger study (i.e. peak power output) and revealed a group size of 18 participants. The power was 0.8 and alpha was set at 0.05.
Participants
As previously described (18), participants were recruited from the databases of the 2 participating rehabilitation centres. Inclusion criteria were: time since injury (TSI) ≥ 10 years, age at onset SCI ≥ 18 years, age 28–65 years, wheelchair-dependent, and physically inactive. People were qualified as “physically inactive” if their score on the “Physical Activity Scale for Individuals with Physical Disabilities (PASIPD)” (19) was lower than the 75th percentile (< 30) of a Dutch cohort study population (20). The PASIPD score (range 0‒182.3) was assessed by a research assistant in a telephone interview prior to inclusion. Exclusion criteria were: contraindications for physical training and testing (e.g. pressure sores or severe cardiovascular problems), psychiatric problems that could interfere with study participation, plans to change current lifestyle habits (e.g. physical activity or diet changes) during the experimental training period, and insufficient knowledge of the Dutch language to understand the purpose and protocol of the study. Due to difficulties with inclusion, one year after trial commencement, the inclusion criterion TSI ≥10 years was reduced to TSI ≥ 8 years to be able to recruit more participants. All participants provided written informed consent indicating voluntary participation in this study, approved by the Medical Ethics Committee of the VU University Medical Center Amsterdam.
Training devices
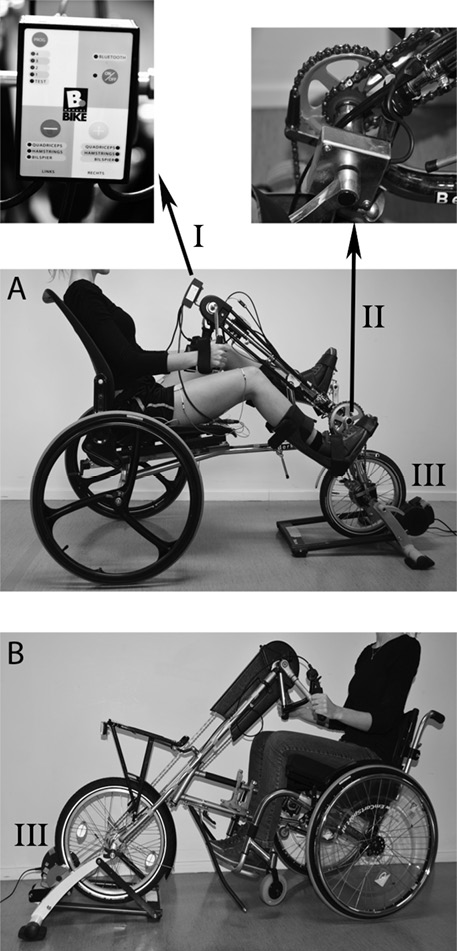
The hybrid cycle (BerkelBike Pro, BerkelBike BV, St Michielsgestel, The Netherlands; Fig. 1A) combines synchronous voluntary handcycling with asynchronous FES-induced leg cycling. A 6-channel stimulator (Impuls, BerkelBike BV, St Michielsgestel, The Netherlands; Fig. 1A-I) provided electrical stimulation via self-adhesive 50 × 90 mm surface electrodes placed bilaterally over the quadriceps, hamstrings and gluteus muscles. During cycling, the stimulator received information from the crank angle encoder (Fig. 1A-II) about pedal position and velocity to control the cyclic stimulation pattern.
The handcycle (Speedy-Bike, Reha-Technik GmbH, Delbrück, Germany; Fig. 1B) was equipped with a wide synchronous bull-horn crank. The front wheel of both devices was mounted on an ergotrainer (Tacx Flow, Technische Industrie Tacx BV, Wassenaar, The Netherlands; Fig. 1A-III and 1B-III) that was adapted to the wheel size of the cycles. Both cycles were equipped with 8 gears that could be changed manually, and quad grips for those participants who needed them.
Training protocol
In the current RCT, an interval training protocol (previously described by Bakkum et al. (18)) was used, since previous studies suggested that these protocols are very convenient to prevent early muscle fatigue and soreness during training (21, 22). Under the supervision of a trainer, participants performed 32 individual training sessions in the rehabilitation centre within a continuous period of 16 weeks. Each session consisted of a 3-min warm-up and cool-down period. After the warm-up, the interval training protocol for that training session started. During the programme, the duration of the training sessions increased from 18 to 32 min (Table I). To provide sufficient recovery time, at least 1 day of rest was scheduled between training days. Following a graded peak wheelchair exercise test on a motor-driven treadmill (also described by Bakkum et al. (18)), the training intensity was set to attain a heart rate response of 65–75% heart rate reserve during training. Briefly, the wheelchair exercise test consisted of a 3-min warm-up session, a 5-min rest interval, 2 3-min submaximal exercise blocks on different constant workloads, and a graded exercise test in which the workload was increased every minute by gradually increasing the slope of the treadmill belt. During the test, heart rate was monitored continuously using radiotelemetry (Polar, Polar Electro Inc., Woodbury, NY, USA). Resting heart rate (HRrest) was defined as the lowest heart rate (mean values over 30 s) attained during the rest interval; peak heart rate (HRpeak) was defined as the highest heart rate (mean values over 30 s) attained during the graded exercise test. The heart rate reserve is the difference between HRpeak and HRrest. The exercise heart rate (HRexercise) at the given training intensity (i.e. 65‒75% heart rate reserve) was calculated as follows: HRexercise = 65‒75% (HRpeak ‒ HRrest) + HRrest. Since the use of heart rate as an indicator for training intensity can be unreliable in some individuals with tetraplegia (23), rating of perceived exertion (RPE) served as a supplementary measure of training intensity; a target RPE of 4–7 on the Borg’s 10-point scale (24) was required during training.
|
Table I. Interval training protocol |
||||
|
Session |
Exercise bout (min) |
Rest (min) |
Repetitions |
Total cycling time (min) |
|
1–3 |
3 |
2 |
6 |
18 |
|
4–5 |
3 |
2 |
7 |
21 |
|
6–7 |
3 |
1.5 |
7 |
21 |
|
8–11 |
3 |
1.5 |
8 |
24 |
|
12–13 |
3 |
1 |
8 |
24 |
|
14–15 |
4 |
2 |
7 |
28 |
|
16–18 |
4 |
1.5 |
7 |
28 |
|
19–20 |
4 |
1 |
7 |
28 |
|
21–24 |
4 |
1.5 |
8 |
32 |
|
25–32 |
4 |
1 |
8 |
32 |
|
Both the hybrid cycle and handcycle training group trained twice a week, following the 16-week interval training protocol. |
||||
Training intensity was controlled by the participant making adjustments in cycle velocity or by the trainer adjusting the gear of the cycle or the resistance of the ergotrainer. In addition, during hybrid cycling, the current amplitude of the electrical stimulation was adjusted manually by the trainer to control the degree of muscle activation. The trainer tried to induce strong muscle contractions throughout training; however, if the legs were moving too fiercely due to the stimulation, or if the participant indicated that the stimulation was too intense, the trainer decreased the current amplitude. Heart rate was recorded constantly during each training session using radiotelemetry (Polar, Polar Electro Inc., Woodbury, NY, USA), and RPE was assessed after each training block. During each training session, information regarding exercise intensity (i.e. heart rate, RPE, current amplitude of the electrical stimulation), gear setting, cycling time, and local pain/complaints was registered by the trainer in the participant’s personal training logbook.
Outcome measures
The outcome measures in the current study (i.e. MetS, inflammatory status and visceral adiposity) were obtained in the week before (pre-) and after (post-) the 16-week training programme.
Metabolic syndrome. MetS was defined as having ≥ 3 of the following symptoms: abdominal obesity (waist circumference (WC) > 102 cm for males, > 88 cm for females); high blood pressure (> 130/85 mmHg or use of medication for hypertension); high TG (≥ 1.7 mmol/l); low HDL-C (< 1.03 mmol/l for males, < 1.29 mmol/l for females); insulin resistance, identified by ≥ 1 of the following: high fasting glucose (≥ 5.6 mmol/l) or insulin (≥ 139 pmol/l) levels, homeostasis model assessment of insulin resistance (HOMA-IR) ≥ 4.0, or use of medication for hyperglycaemia (8, 25). All MetS measurements were performed after a 12-h overnight fast, meaning that participants did not smoke, drink (except for maximal 0.5 l of water) or eat 12 h before these measurements. Supine WC was measured 3 times at the level of the umbilicus using a tape measure, and the mean values was used for data analysis. Blood pressure was taken on the left arm in a sitting position using an automatic device, and the mean values were used for data analysis. Blood samples were taken from an antecubital vein into 3 ml lithium heparin (HDL-C and TG), 2 ml fluoride/oxalate (glucose) and 6.0 ml clot activator (insulin) tubes. Within 2 h after collection, the blood samples were spun down in a centrifuge at 1,800 g for 10 min at room temperature. Subsequently, plasma TG and HDL-C were determined using an enzymatic colorimetric assay, using the reagents GPO-PAP and HDL-C plus, respectively (Roche Diagnostics, Mannheim, Germany). Determination of plasma glucose was carried out using the hexokinase method (Gluco-quant, Roche Diagnostics, Mannheim, Germany). Serum concentrations of insulin were determined using an immunometric assay (Luminescence, Advia Centaur, Siemens Medical Solutions Diagnostics, USA). Glucose and insulin values were used to calculate HOMA-IR (26).
Inflammatory status. Fasting blood samples were collected from an antecubital vein into 6 ml ethylenediaminetetraacetic (EDTA) tubes. Within 2 h of blood collection, plasma was isolated by centrifugation at 1,800 g for 10 min at room temperature, and subsequently aliquoted and stored at –80°C. At the end of the study, plasma concentrations of CRP, IL-6 and IL-10 were determined using quantitative sandwich-type enzyme-linked immunosorbent assay kits (CRP: IBL international, Hamburg, Germany; IL-6 and IL-10: R&D systems, Abingdon, UK), according to the manufacturers’ instructions. The resting pro/anti-inflammatory ratio was calculated by dividing resting plasma IL-6 concentration by resting plasma IL-10 concentration. All samples were analysed in duplicate.
Visceral adiposity. Dual-energy X-ray absorptiometry (DXA; Hologic Discovery, Hologic Inc., Waltham, MA, USA) was used to determine trunk and android fat, which highly correlates (R = 0.65‒0.90) with visceral fat measured by computed tomography (CT) (27–29). Whole-body imaging was acquired according to the manufacturer’s instructions with the participants in the supine position. The trunk and android region were automatically defined using the analytic software accompanying the system (Apex 13.3.3). Since the DXA device was only available in Amsterdam, DXA measurements were only performed in the group that trained in the rehabilitation centre in Amsterdam (Table II).
Trial registration
Netherlands Trial Register (NTR) no. 2855.
Statistical analysis
The assumption of normality was checked by visual inspection of the q-q plot and the box plot of the data within the groups. A Shapiro-Wilk test was also performed on the data. Homogeneity of variance was checked using Levene’s test. In case of violations of these assumptions, as was the case for insulin, HOMA-IR, CRP, IL-6, IL-10 and IL6/IL10-ratio, the statistical analyses were performed on the log-transformed data. Independent sample t-tests were employed to determine potential baseline differences in the outcome measures and personal and lesion characteristics between: (i) the hybrid cycle and handcycle group; (ii) the people who dropped out and those who completed the 16-week training programme; and (iii) the participants from the 2 rehabilitation centres. For each outcome measure separately, differences between pre and post training values were examined using a 2-factor (time × group) mixed measures analysis of variance (ANOVA). In addition, paired-samples t-tests were performed to determine differences between pre and post values for each training group individually. Data are presented as mean ± standard error. Statistical significance was set a priori at p < 0.05. All data were analysed using SPSS version 20 (SPSS Inc., Chicago, IL, USA).
RESULTS
Between November 2011 (start of recruitment) and August 2013 (end of recruitment), 313 people were assessed for eligibility, of whom 35 were randomized to either the hybrid cycle (n = 16) or handcycle (n = 19) group. Of the 35 participants, 19 (9 hybrid cycle, 10 handcycle) completed the 16-week study (Table II). The main reasons for drop-out were illness (3 hybrid cycle, 5 handcycle) and lack of adherence to the training (4 hybrid cycle, 4 handcycle). All 19 participants who completed the study recorded 100% compliance to the programme. For the insulin and HOMA-IR analysis, 3 participants (1 hybrid cycle, 2 handcycle) were excluded due to missing samples. For the inflammatory status, 3 participants (2 hybrid cycle, 1 handcycle) were excluded due to the presence of underlying urinary tract infection or missing sample. No significant baseline differences were present for any of the outcome measures and personal and lesion characteristics between: (i) the 2 intervention groups (all p-values > 0.19); (ii) the people who dropped out and those who completed the 16-week training programme (all p-values > 0.36); (iii) the participants from the 2 rehabilitation centres (all p-values > 0.58). At baseline, MetS was observed in 2 of the 16 drop outs, and in 3 of the 19 people who completed the study.
|
Table II. Participants’ characteristics |
|||||||||
|
Participant |
Sex |
Age (years) |
TSI (years) |
Lesion level |
AIS |
Height (cm) |
Body mass (kg) |
BMI (kg/m2) |
PASIPD score |
|
Hybrid cycle |
|
|
|
|
|
|
|
|
|
|
1a |
M |
55 |
34 |
C3 |
C |
178 |
90.7 |
28.5 |
5.7 |
|
2 |
M |
39 |
13 |
C6 |
B |
184 |
84.4 |
24.9 |
2.4 |
|
3a |
M |
49 |
31 |
C7 |
A |
174 |
55.5 |
18.3 |
1.3 |
|
4a |
M |
53 |
10 |
C7 |
C |
182 |
63.4 |
19.1 |
2.1 |
|
5 |
M |
49 |
27 |
T1 |
A |
186 |
67.2 |
19.4 |
2.8 |
|
6a |
M |
40 |
18 |
T6 |
A |
188 |
66.6 |
18.9 |
1.8 |
|
7 |
M |
58 |
24 |
T8 |
A |
172 |
83.0 |
28.1 |
20.9 |
|
8a |
M |
64 |
18 |
T9 |
A |
174 |
80.2 |
26.5 |
6.0 |
|
9 |
M |
31 |
14 |
T10 |
A |
173 |
73.5 |
24.6 |
8.2 |
|
Mean (SE) |
|
49 (3) |
21 (3) |
|
|
179 (2) |
73.8 (3.8) |
23.1 (1.4) |
5.7 (2.1) |
|
Handcycle |
|
|
|
|
|
|
|
|
|
|
1a |
M |
63 |
10 |
C2 |
D |
180 |
73.6 |
22.9 |
5.9 |
|
2a |
M |
48 |
30 |
C6 |
C |
171 |
91.6 |
31.3 |
9.2 |
|
3 |
M |
47 |
12 |
C6 |
C |
174 |
80.2 |
26.5 |
1.7 |
|
4a |
M |
51 |
21 |
T3 |
A |
181 |
72.6 |
22.2 |
1.8 |
|
5 |
M |
30 |
11 |
T4 |
A |
174 |
73.8 |
24.4 |
15.6 |
|
6 |
M |
49 |
16 |
T5 |
A |
174 |
75.0 |
24.8 |
16.7 |
|
7a |
M |
47 |
18 |
T7 |
A |
185 |
82.0 |
24.0 |
1.0 |
|
8 |
M |
38 |
9 |
T9 |
A |
173 |
60.5 |
20.2 |
23.2 |
|
9 |
M |
49 |
15 |
T11 |
A |
187 |
58.8 |
16.8 |
14.7 |
|
10a |
F |
50 |
14 |
L2 |
A |
166 |
67.2 |
24.5 |
7.4 |
|
Mean (SE) |
|
47 (3) |
16 (2) |
|
|
176 (2) |
73.5 (3.1) |
23.8 (1.2) |
9.7 (2.4) |
|
aDual-energy X-ray absorptiometry (DXA) data available. TSI: time since injury; AIS: ASIA (American Spinal Injury Association) Impairment Scale; BMI: body mass index; PASIPD: Physical Activity Scale for Individuals with Physical Disabilities; M: male; F: female; SE: standard error. |
|||||||||
Metabolic syndrome
For all the MetS components, no significant interaction effects (time × group) were found, indicating that there were no significant differences over time between the hybrid cycle and handcycle training group (Table III). As shown in Table III, an overall significant reduction of 3.1 cm (3.5%) in WC was found following the 16-week training programme. Fig. 2A shows that the training benefits were greater in individuals with a high WC at the beginning of the training programme. For diastolic blood pressure (DBP), an overall significant reduction of 4 mmHg (7.0%) was observed (Table III). Furthermore, there was an overall significant decrease of 26% in both insulin and HOMA-IR (Table III). As shown in Fig. 2C, the reduction in HOMA-IR was achieved in almost all participants. No significant main effects for time were found for systolic blood pressure (SBP), TG, HDL-C and glucose (Table III). However, in ~65% of the participants TG was reduced (Fig. 2B).
Inflammatory status
For all the inflammatory markers, no significant time×group interactions were found, indicating that there were no differences over time between the hybrid cycle and handcycle training group (Table III). Overall, significant reductions of 0.45 mg/l (16.1%), 0.64 pg/ml (26.1%) and 2.97 (31.2%) were found for CRP, IL-6 and IL-6/IL-10 ratio, respectively; for IL-10, there was no significant main effect for time (Table III). Fig. 2D shows that almost all participants showed a decrease in CRP. As demonstrated in Figs 2E and 2F, participants with high pre-training IL-6 values and IL-6/IL-10 ratios showed greater reductions than participants with low pre-training values.
Visceral adiposity
For visceral adiposity, no significant time × group interactions were found, indicating that there were no differences over time between the hybrid cycle and handcycle groups (Table III; Fig. 2G and 2H). For trunk and android fat percentage, overall significant reductions of 3.6% and 4.7% were observed, respectively. However, no significant main effects for time were found for trunk and android fat mass (Table III).
Moreover, for all the outcome measures, there were no significant differences over time between people with tetraplegia and those with paraplegia (Fig. 2).
|
Table III. Effects of the 16-week exercise programme, using a hybrid cycle or handcycle, on metabolic syndrome components, inflammatory status and visceral adiposity |
||||||||||||
|
|
HYB |
|
HC |
|
p-values mixed measures ANOVA |
|||||||
|
Pre Mean (SD) |
Post Mean (SD) |
Δ Mean (SD) |
p |
|
Pre Mean (SD) |
Post Mean (SD) |
Δ Mean (SD) |
p |
|
Main effect time |
Interaction (time × group) |
|
|
MetS components (n = 9 HYB, 10 HC) |
||||||||||||
|
WC (cm) |
91.8 (4.7) |
87.8 (4.0) |
–3.9 (1.3) |
0.02 |
|
89.7 (3.5) |
87.3 (2.9) |
–2.5 (1.0) |
0.03 |
|
0.001 |
0.38 |
|
SBP (mmHg) |
112 (6) |
117 (9) |
+5 (5) |
0.39 |
|
119 (4) |
123 (3) |
+4 (4) |
0.30 |
|
0.18 |
0.92 |
|
DBP (mmHg) |
69 (3) |
63 (4) |
–6 (3) |
0.04 |
|
72 (3) |
70 (4) |
–3 (3) |
0.34 |
|
0.03 |
0.31 |
|
TG (mmol/l) |
1.7 (0.2) |
1.4 (0.2) |
–0.3 (0.1) |
0.01 |
|
1.2 (0.2) |
1.1 (0.1) |
–0.1 (0.2) |
0.67 |
|
0.15 |
0.49 |
|
HDL-C (mmol/l) |
1.1 (0.1) |
1.2 (0.1) |
+0.1 (0.1) |
0.22 |
|
1.4 (0.2) |
1.4 (0.2) |
0.0 (0.1) |
0.94 |
|
0.30 |
0.35 |
|
Glucose (mmol/l) |
5.7 (0.3) |
5.8 (0.4) |
+0.1 (0.1) |
0.38 |
|
5.3 (0.2) |
5.1 (0.2) |
–0.2 (0.2) |
0.30 |
|
0.68 |
0.17 |
|
Insulin (pmol/l)a |
72.7 (10.6) |
56.0 (9.5) |
–18.9 (9.4) |
0.11 |
|
54.6 (8.5) |
40.5 (7.3) |
–14.3 (4.0) |
0.01 |
|
0.004 |
0.65 |
|
HOMA-IRa |
2.8 (0.5) |
2.2 (0.6) |
–0.6 (0.4) |
0.16 |
|
1.9 (0.3) |
1.3 (0.2) |
–0.5 (0.2) |
0.02 |
|
0.006 |
0.44 |
|
Inflammatory status (n = 7 HYB, 9 HC) |
||||||||||||
|
CRP (mg/l) |
3.91 (1.75) |
3.20 (1.68) |
–0.71 (0.36) |
0.08 |
|
2.86 (1.36) |
2.47 (1.38) |
–0.39 (0.18) |
0.23 |
|
0.05 |
0.92 |
|
IL-6 (pg/ml) |
2.51 (0.91) |
1.88 (0.58) |
–0.63 (0.59) |
0.20 |
|
2.40 (0.57) |
1.76 (0.36) |
–0.64 (0.36) |
0.10 |
|
0.04 |
0.93 |
|
IL-10 (pg/ml) |
0.29 (0.03) |
0.29 (0.04) |
0.00 (0.02) |
0.73 |
|
0.26 (0.02) |
0.32 (0.05) |
+0.06 (0.04) |
0.15 |
|
0.29 |
0.16 |
|
IL-6/IL-10 ratio |
8.07 (2.33) |
7.23 (2.47) |
–0.84 (2.45) |
0.34 |
|
10.65 (3.40) |
5.96 (1.92) |
–3.70 (2.07) |
0.05 |
|
0.04 |
0.54 |
|
Visceral adiposity (n = 5 HYB, 5 HC) |
||||||||||||
|
Trunk fat (kg) |
9.7 (1.6) |
9.2 (1.5) |
–0.5 (0.5) |
0.40 |
|
13.2 (1.7) |
12.7 (1.7) |
–0.5 (0.5) |
0.34 |
|
0.20 |
0.99 |
|
Trunk fat (%) |
27.5 (2.7) |
25.9 (2.3) |
–1.5 (0.7) |
0.11 |
|
33.7 (2.5) |
33.0 (2.5) |
–0.7 (0.5) |
0.26 |
|
0.04 |
0.41 |
|
Android fat (kg) |
2.0 (0.4) |
1.9 (0.4) |
–0.1 (0.1) |
0.34 |
|
2.6 (0.4) |
2.6 (0.4) |
0.0 (0.2) |
0.85 |
|
0.47 |
0.68 |
|
Android fat (%) |
33.4 (2.9) |
31.3 (2.6) |
–2.1 (0.5) |
0.02 |
|
38.6 (3.7) |
37.2 (3.3) |
–1.3 (1.0) |
0.26 |
|
0.02 |
0.52 |
|
aAnalysis was performed on n = 8 HYB, 8 HC. Pre and post 16-week training values, as well as the mean pre-post difference (with p-values), are provided for all outcome measures (i.e. metabolic syndrome components, inflammatory status and visceral adiposity). For all outcome measures, no significant interaction effects were found, indicating that there were no significant differences over time between the hybrid cycle and handcycle group. HYB: hybrid cycle group; HC: handcycle group; MetS: metabolic syndrome; Δ: mean pre-post difference; WC: waist circumference; SBP: systolic blood pressure; DBP: diastolic blood pressure; TG: triglycerides; HDL-C: high-density lipoprotein cholesterol; HOMA-IR: homeostasis model assessment-estimated insulin resistance; CRP: C-reactive protein; IL-6: interleukin-6; IL-10: interleukin-10. |
||||||||||||
DISCUSSION
The main finding of this study was that the 16-week training programme, using either a hybrid cycle or a handcycle, resulted in similar positive effects on different MetS components (WC, DBP, insulin and HOMA-IR), inflammatory status (CRP, IL-6 and IL-6/IL-10 ratio), and visceral adiposity (trunk and android fat percentage), indicating that there were no notable benefits of the FES-induced leg exercise over handcycle training alone.
Metabolic syndrome
At the start of the intervention programme, 16% of participants who completed the programme met the criteria for MetS. In comparison with a cross-sectional study on the prevalence of MetS in people with SCI (25), this percentage is relatively low. As stated in the introduction, it is well documented that people with SCI have impaired levels of several MetS components (e.g. HDL-C and insulin) (5, 6). However, for the group of participants in this study, the mean values for all the MetS components were not elevated. Since there were no significant baseline differences between the individuals who dropped out and those who completed the study, it might be suggested that the participants who were enrolled in this study were relatively healthy compared with the average population with long-term SCI. Despite this, there were still positive training effects on different MetS components in this participant group. For example, the reduction in WC suggests that hybrid cycle and handcycle exercise reduces abdominal obesity. At the start of this study, 3 of the 19 participants met the criteria of abdominal obesity. After 16 weeks of training, only 1 participant still met these criteria, but this person showed a reduction of 11 cm (9.4%) in WC. Another important result of this study was the reduction in insulin and HOMA-IR, indicating a reduced insulin resistance. Several previous studies have also found positive effects of exercise on insulin resistance (30–32), while another study has not (33). In contrast, no significant changes were found for the lipids TG and HDL-C. That said, looking at the individual data, ~65% of the participants showed reductions in TG (Fig. 2C). These findings are in accordance with a systematic review by Carlson et al. (34), who concluded that there was insufficient evidence that exercise alone improves lipid disorders in people with SCI. It requires further investigation to examine whether a combined exercise and dietary intervention is the optimal method for improving lipid spectrum in people with SCI. Together with the reduced DBP, the above-described findings suggest that exercise has the potential to reduce several MetS components in people with long-term SCI.
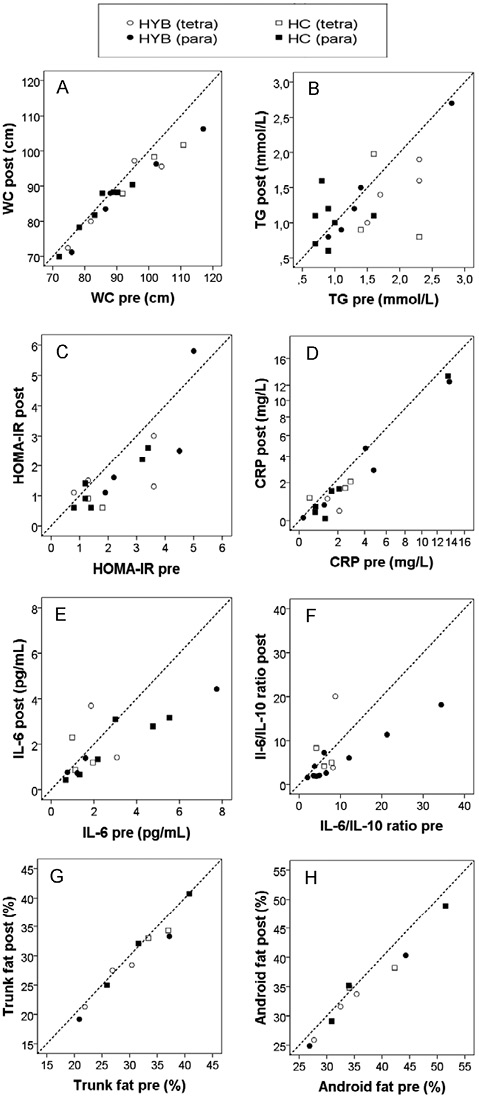
Fig. 2. Individual values for metabolic syndrome, inflammatory status and visceral adiposity in the week before (pre) and after (post) the 16-week training programme. Each data point represents the pre and post value of 1 participant. The dotted line is the line of identity. For example, if for interleukin (IL)-6, a data point lies below the line of identity, this means that the IL-6 concentration was reduced following the 16-week training programme. (A) waist circumference (WC); (B) homeostasis model assessment of insulin resistance (HOMA-IR); (C) triglycerides (TG); (D) C-reactive protein (CRP); (E) interleukin (IL)-6; (F) IL-6/IL-10 ratio; (G) trunk fat percentage; (H) android fat percentage. HYB: hybrid cycle; HC: handcycle; tetra: tetraplegia; para: paraplegia.
Inflammatory status
In the current cohort, resting inflammatory status was typical of untrained chronic SCI population groups (5, 35). Accordingly, 50% of the participants displayed resting inflammatory profiles symptomatic of an increased risk of CVD (IL-6 > 2 pg/ml; CRP > 3 mg/l). However, a large heterogeneity was present in resting values, suggesting SCI and physical inactivity alone are not solely responsible for a chronic inflammatory state. In this study, both exercise interventions resulted in a significant improvement in inflammatory status. These findings are consistent with those of Griffin et al. (16), who reported a significant reduction in resting IL-6 and CRP concentration following a 10-week FES-cycle training programme. Hybrid exercise has previously been shown to induce a greater acute IL-6 response (17) and greater energy expenditure (36) than handcycle exercise alone at a matched workload. However, both exercise modalities in the current study resulted in a similar significant reduction in inflammatory status (IL-6 and CRP).
Visceral adiposity
The mean values for visceral adiposity in this study were relatively low compared with the values reported in a study by Emmons et al. (37), who assessed visceral adiposity in people with SCI and able-bodied persons. This again supports the assumption that the participant group in the current study was relatively healthy. Despite this, a significant reduction in trunk and android fat percentage was found, suggesting that exercise has the potential to reduce visceral adiposity. This finding was in accordance with a study by Gorgey et al. (38). Since DXA measurements are relatively expensive and time-consuming, researchers might also consider using the anthropometric measure WC (which is a reliable surrogate of visceral adiposity in able-bodied persons (5)) as a measure of visceral adiposity.
Hybrid cycle and handcycle exercise
The fact that the hybrid cycle and handcycle groups showed similar improvements in several CVD risk factors suggests that the relatively small muscle mass available during handcycling alone is not a limiting factor for the reduction in CVD risk factors when exercise is performed on a regular basis at an intensity of 65–75% HRR. The findings that handcycle exercise alone provides a sufficient training stimulus and that there were no notable benefits of the added FES-induced leg exercise, promote handcycling as a cheaper and more accessible exercise mode for reducing CVD risk factors than hybrid cycling. However, Bakkum et al. (36) have demonstrated that hybrid cycling induces higher metabolic and cardiorespiratory responses at equal subjective exercise intensity levels than handcycling, suggesting that hybrid cycling might be more suitable for fighting obesity and increasing cardiorespiratory fitness in individuals with SCI. Moreover, the addition of FES-induced leg exercise to handcycling has the potential to provide supplementary benefits on vascular (39) and musculoskeletal systems (40) in the lower extremities.
Study limitations
A possible limitation of this study was that the lower-limb muscles of the participants in the hybrid cycle group were relatively untrained at the beginning of the programme, resulting in muscle fatigue during cycling. If the leg musculature becomes fatigued over time, the arms will take over the entire propulsion. To ensure strong lower-limb muscle contractions over the entire exercise period (i.e. 30 min), a conditioning phase for the paralysed legs (e.g. FES-induced leg cycling only) for the participants in the hybrid group could have been performed. The training effects might have been larger if all participants were able to complete 30 min of continuous leg exercise at the start of the hybrid cycle programme. Another limitation was the relatively high drop-out rate (46%), which considerably reduced the power of the study. Although there were no baseline differences for any of the outcome measures or personal and lesion characteristics between the group that dropped out and the group that finished the training programme, the reduced power might have resulted in type II errors. Moreover, due to the relatively small sample size, there was not enough power to perform multivariate regression analyses to examine the influence of possible confounders (e.g. lesion severity and level) on the present study results. The high drop-out rate might also question the feasibility of this type of exercise intervention in people with long-term SCI. Firstly, it was difficult to recruit participants (only l1.2% of the people who received an invitation letter eventually participated), and secondly, it was difficult to keep the participants in the programme. The most mentioned reason for not participating and drop out was that the exercise intervention was too time-consuming and could not easily be implemented in the daily life of these people. Therefore, future studies should consider how to make exercise interventions more feasible and attractive for this population. For example, better facilitation of the training equipment might save time; if people can exercise at home they do not have to travel to a rehabilitation centre several days a week.
In conclusion, this study demonstrated that a 16-week exercise programme, using either a hybrid cycle or a handcycle, had similar beneficial effects on several CVD risk factors, including MetS components, inflammatory status and visceral adiposity, indicating that there were no notable benefits of the FES-induced leg exercise over handcycle training alone.
ACKNOWLEDGEMENTS
This study was financially supported by Zon-Mw Rehabilitation program and Fonds NutsOhra (grant no. 89000006). The authors would like to thank research assistants Hennie Rijken and Maurits Sloots for recruiting and testing all the participants. Furthermore, the authors would like to thank all the interns for helping the research assistants with the training sessions and the data collection.
The authors declare no conflicts of interest.
REFERENCES

