Andrea Hållstam, MSN1, Britt Marie Stålnacke, MD, PhD2, Christer Svensen, MD, PhD1 and Monika Löfgren, PT, PhD3
From the 1Department of Clinical Science and Education, Södersjukhuset, Karolinska Institutet, Stockholm, 2Department of Community Medicine and Rehabilitation, Umeå University, Umeå and 3Karolinska Institutet, Department of Clinical Sciences, Danderyd University Hospital, Stockholm, Sweden
OBJECTIVE: To explore patients’ experiences of activity, participation and quality of life one year after a rehabilitation programme for chronic pain, and to determine the impact of the programme on their current life situation.
DESIGN: Qualitative study with emergent design.
Subjects and methods: The 14 informants were patients with chronic pain who had participated in rehabilitation at a pain clinic. Individual semi-structured interviews were analysed with inductive, qualitative content analysis.
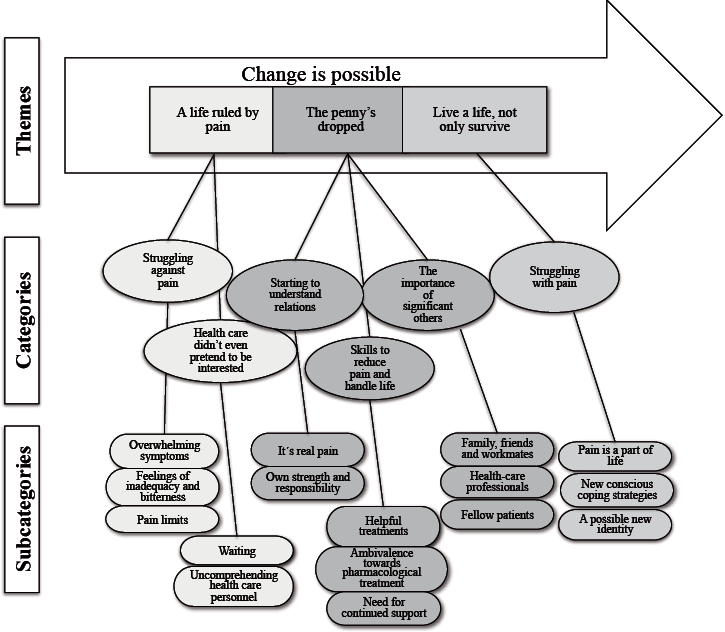
RESULTS: The core theme “Change is possible” and the themes “A life ruled by pain” (the situation before rehabilitation), “The penny’s dropped” (experience during rehabilitation) and “Live a life, not only survive” (the situation at the time of the interviews) emerged from the data. These themes represent a process through which, during and after rehabilitation, the informants integrated earlier disabling symptoms into a functioning lifestyle.
CONCLUSION: Individuals living with disabling chronic pain can create a better life by integrating their illness. A prerequisite is that healthcare professionals empower patients to develop the strength to take responsibility for their daily lives. This process is facilitated by skills to reduce pain and handle life, plus support from significant others.
Key words: chronic pain; rehabilitation; qualitative research; pain clinic; interview.
J Rehabil Med 2015: 47: 00–00
Correspondence address: Andrea Hållstam, Department of Clinical Science and Education, Södersjukhuset, Karolinska Institutet, SE-118 83 Stockholm, Sweden. E-mail: andrea.hallstam@sodersjukhuset.se
Accepted Oct 9, 2014; Epub ahead of print Dec 9, 2014
Introduction
Chronic pain, defined as persistent or recurring pain for at least 3 months, is a common, complex condition negatively affecting both the individual and society (1, 2). Chronic pain can be understood from a bio-psycho-social perspective including somatic, psychological, environmental and personality aspects (3). Pain is always a personal and intangible experience. Individuals with chronic pain often report other symptoms, such as fatigue, insomnia, concentration difficulties, anxiety and depression (4, 5). To live with chronic pain is described as a loss of identity (6, 7). Negative experience related to uncomprehending relatives and caregivers is also commonly reported (8, 9).
No medical treatment has been universally successful in relieving chronic pain (10). The most evidence-based and recommended treatment is multimodal, multidisciplinary rehabilitation programmes (11, 12). While studies have shown that it is possible to reduce pain and disability and thus improve psychological well-being as well as quality of life (13, 14), questions remain about how to tailor multimodal programmes to meet individual needs (11, 12).
Qualitative research has suggested some models for understanding patients` experience based on rehabilitation. These models describe a change process from chaos and despair to acceptance, improvement in self-image, and life- and work-roles in individuals with diagnoses, such as fibromyalgia, chronic widespread pain and whiplash-associated disorders (15–19). Getting a diagnosis (20), examination by medical experts (21), being believed by healthcare professionals (18) and recognition from fellow patients are all described as important in initiating a change process (16, 22, 23). Few studies so far, however, have explored patients’ experience regarding the multimodal rehabilitation (MMR) process and its impact on daily life (15).
Individuals with chronic pain are treated in different clinical contexts, such as in primary care, rehabilitation medicine or anaesthesia, with MMR or uni-modal treatments. Although the use of MMR in traditional pain clinics has increased, knowledge about patients’ experience in this context is scarce. The present study therefore aimed to explore how patients experience activity, participation and quality of life one year after the start of MMR at a pain clinic, and what impact this has had on their ability to manage daily life.
Methods
Study design
A qualitative method with an emergent design was used, since it is suitable for exploring human experience in areas where knowledge is scarce and minimally theorized (24, 25). Data were collected using semi-structured individual interviews and analysed according to qualitative content analysis. This permitted us to build a model of the phenomena described by the informants (24).
Informants
Sixteen patients (informants) meeting the inclusion criteria were consecutively asked to participate in the study. Fourteen (13 women and 1 man) accepted and gave their informed consent. Two declined due to lack of interest or time. Inclusion criteria were: participation in MMR during the previous year, participation in a questionnaire survey, and the ability to understand and speak Swedish. Inclusion criteria for the questionnaire study were: pain for more than 3 months and age >18 years. The exclusion criterion was severe illness. The informants lived in the Stockholm area. For background data see Table I.
|
Table I. Background data for the 14 informants at the time of the interview |
|
|
Age, years, mean (SD) |
46 (13) |
|
Gender female/male, n |
13/1 |
|
Country of origin, n |
|
|
Sweden |
9 |
|
Nordic countries |
1 |
|
Other European country |
2 |
|
Outside Europe |
2 |
|
Education, n |
|
|
Elementary school |
2 |
|
Upper secondary school |
8 |
|
University |
2 |
|
Other |
2 |
|
Civil status, n |
|
|
Living alone |
5 |
|
Married/attached |
2 |
|
Living with a family |
7 |
|
Livelihood, n |
|
|
Employment income > 50% |
4 |
|
Sickness benefit > 50% |
4 |
|
Sickness compensation > 50% |
4 |
|
Early retirement > 50% |
2 |
|
Unemployed |
2 |
|
Student > 50% |
2 |
|
Retired |
1 |
|
Pain duration, years, mean (SD) |
12 (13) |
|
Pain diagnosis, n |
|
|
Fibromyalgia |
4 |
|
Cervicobrachial syndrome |
2 |
|
Central sensitization |
4 |
|
Coxarthrosis |
1 |
|
Disc herniation |
1 |
|
Frozen shoulder |
1 |
|
Myalgia |
1 |
|
Lumbago with sciatic pain |
1 |
|
Pelvic pain, endometriosis |
2 |
|
Nociceptive pain NOS |
1 |
|
Co-diagnosis, n |
|
|
Anxiety |
4 |
|
Depression |
5 |
|
Pharmacological treatmenta, n |
|
|
SNRIs |
6 |
|
SSRIs |
1 |
|
TCAs |
1 |
|
Paracetamol |
1 |
|
Tramadol |
1 |
|
Pregabalin |
1 |
|
NSAIDs |
1 |
|
aPrescribed during the programme. SD: standard deviation; SNRIs: serotonin–norepinephrine reuptake inhibitors; SSRIs: selective serotonin re-uptake inhibitors; TCAs: tricyclic antidepressants; NSAIDs: non-steroidal anti-inflammatory drugs; NOS: not otherwise specified. |
|
Rehabilitation programme and team
The programme was part of the pain clinic activities at Södersjukhuset, Stockholm, Sweden. This clinic serves a catchment area of approximately 500,000 inhabitants.
The referred patients were initially assessed by a multidisciplinary team, which planned the treatment together with the patient. The prerequisites for MMR were significant impact of pain on function and quality of life and readiness for behaviour change.
The MMR included coordinated treatment individually and/or in groups, was conducted according to the principles of behavioural medicine, and varied according to the patient’s needs. The team members were physicians, who adjusted the pharmacological treatment (see Table I) and sick-listing and led mindfulness groups. A psychologist who was responsible for individual cognitive behavioural therapy (CBT) (10) and a physiotherapist with special training provided acceptance and commitment therapy (ACT) (26, 27). Nurses provided first assessments and treatment with transcutaneous electric nerve stimulation (TENS), pharmacological follow-up and counselling. Physiotherapists led physical activities, such as individually adapted training in the gym, warm-water exercise and basic body awareness therapy according to the principles of Roxendahl (28). The pain self-management courses and the training groups comprised, on average, 10 participants. Representatives from all the professions mentioned participated in the 8-session pain self-management courses. A contact person from among the team members supported each patient in identifying and following up rehabilitation goals. The 3-month programme included 2–4 weekly treatment sessions of 1–2 h each. The team collaborated with the Swedish Social Insurance Agency and the patient’s employer when required.
Data collection
Data were collected from May 2012 to January 2013, approximately 1 year after the informants’ rehabilitation. An interview guide comprising 2 question areas, “Former and present lifestyle” and “Rehabilitation programme”, was formed and tested in a pilot interview. The guide was further developed during the study (Table II), according to emergent design (29).
|
Table II. Interview guide and examples of follow-up questions |
|
Initial question areas: • Former and present lifestyle • Rehabilitation programme Emerging question areas: • Expectations of pain clinic • Where to find strength for change • Future Examples of follow-up questions: • Tell me how your life works today • What do you do during the day? • What feelings and thoughts do you have about your activities? • What is the difference compared with before rehabilitation? • What are your memories of how life worked before? • Can you tell me about any changes? • Can you tell me how you got the strength for the change? |
The informants chose the location for the interview. Eleven interviews were conducted in the hospital, the others in the informants’ homes. The interviews lasted between 32 and 68 min (mean 50 min) and were recorded digitally and transcribed verbatim. The interviewers (AH and ML) had not been involved in the informants’ rehabilitation.
Data analysis
Inductive qualitative content analysis was carried out (24). An emergent design was used, in which the interviews and the analysis continued and developed in parallel (29). The analysis started with AH listening to and reading each interview several times for gist. The first interview was divided into meaning units, which were coded by AH and ML independently of each other and then discussed until agreement was reached. The freeware Open Code (30) was used for coding and abstraction. After 6 interviews, the codes were sorted into preliminary sub-categories by AH and ML. In the next steps the sub-categories were formed into categories, relationships between the categories were explored and preliminary themes developed. The interviewing, coding and exploration of the model continued until 14 interviews had been analysed; for examples see Table III. After 12 interviews, saturation was reached within the themes, and the last 2 interviews confirmed these results. The analysis continued with discussions among all the researchers. The process was continued by AH returning to the interviews and re-reading to compare the results with the original interview data. During the whole process the results were discussed regularly by AH and ML and finally among all the authors.
|
Table III. Examples of content analysis process with quotations from different informants |
||||
|
Quotations |
Code |
Subcategory |
Category |
Theme |
|
“When the penny’s dropped, you know, when these small parts of the puzzle, it was before the mindfulness course, but when these small parts of the puzzle quite suddenly fell into place I realized that I, that I, have just as much pain if I’m lying here in bed and crying as I do if I get up and take my kids to the park” |
The penny’s dropped |
Own strength and responsibility |
Starting to understand relations |
The penny’s dropped |
|
“I got pelvic girdle loosening then, that I do know, and that’s where my pain started”. |
Cause of pain |
It’s real pain |
||
|
“Oh that’s very heartening, ‘cos then I know that next time, I have my own proof that I can manage this, I don’t need to, sort of rush off anywhere, don’t need to take any tablets. Ahh…but it can be sorted out”. |
Own ability |
Own strength |
||
|
“You weren’t just one among the many they visit or as a patient, yeah, it felt good to go there and then I got, yes, I got more energy and strength just because it felt so good”. |
Understanding things |
Healthcare professionals |
The importance of significant others |
|
Ethical considerations
The study was approved by the Regional Ethical Review Board, Stockholm (Dno: 2010/1903-31/5) with a supplementary application (Dno: 2012/75-32).
Results
The analysis resulted in a core theme formed of themes, categories and subcategories (Fig. 1). The core theme “Change is possible” represents the process the informants described from before rehabilitation (“A life ruled by pain”) through the rehabilitation programme (“The penny’s dropped”) to the life situation 1 year after starting rehabilitation (“Live a life, not only survive”).
Fig. 1. Patients’ experience of a rehabilitation programme for chronic pain. The arrow representing the core theme illustrates the change process, which is linked by 3 phases described in the themes. Within the themes the categories and subcategories describe the content.
Change is possible
The core theme, formed of 3 themes, describes the informants’ process from a life ruled by pain to a life worth living. The informants described their lives before the rehabilitation programme as being dominated by pain, a social life in chaos and with limited activities. Experience of negative encounters and of being distrusted in healthcare had made them frustrated and hopeless. During rehabilitation the informants received validation of the pain and reassurance that they were credible individuals. They became aware of their own strength; that they were not victims of the pain, but were able to change their situation, and that they were responsible for changing it. They started to learn about and understand the relationship between the pain and their own lifestyle. Multiple factors, differing among the informants, were important for driving this process. For example, to be met as a trustworthy person with “real” pain strengthened the informants and supported them in believing in themselves. This enabled them to think that their own action could make a difference for the better and they started to develop different strategies to handle their life situation. At the time of the interviews, approximately one year later, their life was not only bearable, but had also gained a sense of worth.
The themes and associated categories that emerged from the data are presented below.
A life ruled by pain. This theme describes the situation before the first visit to the pain clinic. Life was chaos and the informants’ experience of healthcare was disappointing. Two categories emerged from the data on this theme, as follows:
• Struggle against pain: every single moment of everyday life was governed by pain. Informants described how life was falling apart, not only for themselves, but also for the whole family. Pain influenced their minds and lowered their self-esteem. Hopelessness, anxiety and depression were described, as well as bitterness and the injustice of having been afflicted by pain. Concentration was difficult, and energy went on pain, leaving no possibilities to maintain previous social roles.
“With the children and that, earlier I hardly dared do a thing … I was in pain, there was loads of irritation and I poured heaps of it out over other people. You got cross and angry and so on… (sigh)..”
Disabling pain stopped them from being active in the household and at work. Life was limited by poor finances and dependence on others. Some informants had more or less stayed in bed for months before the rehabilitation programme started.
• Healthcare did not even pretend to be interested: describes prior experience of meeting healthcare professionals in all kinds of setting. The opinion was that the waiting time to see a pain specialist, and to get treatment and diagnosis was too long. Meetings with healthcare professionals were occasionally described as supportive or understanding, but mainly as negative encounters. Informants felt misjudged, distrusted and that their hopes had been dashed. They felt that caregivers expected them to appreciate treatment or surgery, regardless of the result.
“The orthopaedic surgeon I met this time, he was terrifically clumsy, and said, well, that’s something you cause yourself, he said.”
Information about pain was unclear or lacking and this was explained by the informants as the physicians’ limited knowledge and limited commitment to healthcare.
Negative experience before the pain clinic visit had made the informants insecure and sceptical. Their expectations regarding getting help were minimized.
The penny’s dropped. This theme describes the informants’ sudden awareness of being responsible for their own lives; a turning point. This awareness, together with support from treatment and significant others, enabled them to change towards a better life. For some informants the change was more cautious or even unconscious. Three categories emerged from the data on this theme, as follows:
• When the informants Started to understand relationships between their pain and their own attitude and actions, they were strengthened. Seeing the relationships made it possible for informants to take responsibility and manage their life differently. In the clinic they receive credible explanations of their pain, explanations they had longed for. A diagnosis or acknowledgement of the existence of pain helped the informants to feel accepted as individuals with pain. They discovered a power within themselves and they stressed the significance of acknowledging their responsibility for their own lives. Examples of taking responsibility were to start getting involved socially, to do physical activity or to use coping learnt during CBT.
“When the penny’s dropped, you know these small parts of the puzzle, that was before the mindfulness course, when these small parts of the puzzle fell into place and I suddenly realized that I have just as much pain lying here in bed and crying as I do if I get up and take my children to the park.”
• Skills to reduce pain and handle life describes how treatment could be useful or cause disappointment. For example, pool training made the body feel more supple, and mindfulness helped the informants to manage difficult situations. The pain self-management course increased knowledge about pain, thoughts and behaviour. Skills to reduce pain and to handle life facilitated the change process.
“And then I got it (TENS), that’s helped me tremendously I do it every day, erm, when I’m in greatest pain it can, it helps and it may be that it’s a mental thing, I don’t know, but I think it helps at all levels.”
The informants preferred non-pharmacological treatment and expressed ambivalence or resistance to pharmacological treatment. Prescribed drugs could sometimes reduce pain, but if they did not, the feeling was disappointment and side-effects were described.
“And I tried new medicines, you see, for my pain, I had to, but I was not really satisfied with them so I, er, said they made me feel ill, I didn’t have any feelings, it was, I could not live with things as they were, it was, I thought, not sort of me.”
The rehabilitation programme was experienced as a good beginning, but too short and the informants wanted continued support.
• The importance of significant others; support from family and friends was of major weight, especially in the early phase of rehabilitation, for encouragement and support in the change of behaviour.
“Well, it was probably not me but my eldest son who told me, start making a timetable and, what d’you call it, write in what you’ve got to do and be prepared a little. They’re very wise, these kids.”
Later, when the informants were on their way back to work, support from workmates and the possibility of flexible working hours facilitated the return to work.
The positive encounters with the pain clinic’s team members raised the informants’ self-esteem and facilitated the change process. For several informants it was the first time they had felt understood, respected and seen. They appreciated meeting professionals who truly cared and being treated as equals in discussions about the rehabilitation plan. The informants felt safe and regained hope.
“Yes, well, I think I got strength from feeling I was no longer mistrusted and not feeling I’d been declared an idiot. Instead, you were very very well received, spoken to by name and they remembered you. You weren’t just one of a crowd they visit, or as a patient, but yeah, it felt good to go there and I got, I think I got, more energy and strength just because it felt so good.”
Fellow patients contributed towards feelings of not being alone, or they provided an insight that other people are even worse off. The informants appreciated learning from the others in the group, and also realizing that their own participation was important and helpful to others.
Live a life, not only survive. This theme describes the differences in the informants’ daily life before rehabilitation compared with at the time of the interviews. The following category emerged from the data on this theme:
• Struggle with pain; the informants were still having pain, but “fighting against pain” was replaced by “struggling with pain”. Life had mostly regained normality. They were able to do most of what they wanted to and they had resumed their social contacts. They now took part in household and leisure activities. Five had gained employment or started an education.
“I can, yes I can do everything again, practically can go with my children to the park again, I can do the washing, washing up, cook, I can work!”
The informants accepted that pain had become a part of their life, inflicting some restrictions, but not a limiting condition. Since pain had become a part of the individual self, there was no longer a need to fight it. The informants acknowledged that life could be better sometimes and worse other times.
“I my greatest wish in the whole world should be that I was free of pain, but I am, as I said, I realized that it’s not to be so I have to focus on other things.”
New coping strategies were described. The strategies included awareness of the importance of regular physical activity, dealing with anxiety and practical matters. The importance of setting goals for activities and finding a balance between activity and rest was stressed. The informants used non-pharmacological treatment for pain reduction and they had learnt to manage their feelings by, for example, allowing themselves to show emotion or using coping strategies learnt during the programme.
“I must stand up when they get home, meet me. Not that they (the children) meet the sofa. I must manage, it isn’t some illness, it is, like, everyone has some illness, people like me...”
A possible new identity had emerged at the time of the interviews. Informants described feelings of pride and maturity as humans related to the new life experience.
“Eh, this has led to my accepting all this, that I’m quite simply not fully fit, but I, they call it functional impairment and it took a bit of time to accept it, but that’s how it is..”
However, not all had this experience; instead their main experience was still a struggle.
Those who gained fewer benefits from the rehabilitation programme experienced their lives as unchanged and difficult to manage due to pain and anxiety. They described an increased level of activity, but felt no better.
Discussion
The main results of this study were the informants’ change from a life of disabling pain and chaos towards one of functioning and good quality. One year after rehabilitation they described how their family life had improved and some had started to work or study. The important steps towards the integration of pain into everyday contemporary life were that the informants received an explanation of the pain and found their own strength and responsibility to govern their daily lives. Support from significant others and skills to reduce pain were other important factors in this integration process. During the year after starting the rehabilitation most informants had developed new conscious coping strategies and new identities.
To understand the informants’ rehabilitation process and their improved ability to manage daily life, a theoretical framework is needed. At the start of the project we sought an unbiased approach, allowing the results to form our theoretical frame. During the analysis it became clear that the core findings could be explained by Hernandez’ theory of integration (31, 32) and by the theory of empowering encounters (33).
Hernandez’ theory provides a model for understanding how individuals with chronic illness can integrate new life experiences of the illness into the self via a 3-phase process (31). To integrate negative life experiences is a way to find new approaches in the development of a new identity. The theory’s first phase is characterized by a lack of knowledge about the disease, denial and minimal control. This is consistent with our results in the theme “A life ruled by pain” where the informants’ desire for good information and an explanation of the pain are described. In addition, the informants’ experience of activity limitation, pain and other symptoms is in line with the theory. Phase 2 of the theory includes an emotional crisis that alters the informant’s attitude to the illness (32). In the present study, as well as in other studies of chronic pain (15, 19, 34), the informants described becoming aware of their own strength and responsibility: this initiated change. The distinct awareness pinpointed in the present study is, however, rarely described in other studies. At the time of the interviews, in the theme “Live a life, not only survive”, the informants described their lives as functioning well. They had accepted pain with limitations and developed new coping strategies as well as a new identity. Their individual self and the illness chronic pain had become integrated, consistent with Hernandez’ phase 3 where focus is on knowledge and handling the disease. These findings are in line with previous studies (16, 35).
Some informants, however, were caught in the experience of pain that ruled their life. They did not reach integration or the turning point. Integration is a non-linear and unpredictable process (36). It is difficult to be a part of a change process such as the one described here. There may be many reasons for being unable to achieve such comprehensive changes.
Another important finding, as in previous studies, is the significance of the patients’ encounters with healthcare professionals in facilitating the change process (18, 20). The theory of empowering encounters describes the importance of professional support for women with chronic pain (37). The encounter can be empowering or disempowering depending on the quality of healthcare the professionals provide (33). Our findings underline the essential meaning of the encounter as an interpersonal process.
The informants’ criticism of caregivers and care organizations has been illustrated in other studies (8, 17, 20). A negative encounter keeps the patient disempowered and promotes a sense of losing control (17, 20, 37) and thus counteracts a positive change process.
The support, not only of family, friends and workmates, but also of fellow patients is reportedly significant in starting the change process (23, 38). Our results add the informants’ sense of personal significance in helping others by contributing their own experience or by being a good example.
Methodological considerations
We propose that the present results can be transferred to other contexts in which patients with chronic pain are treated. We used a convenience sample, which is possibly a limiting factor; but the informants represented a wide range of experience related to diagnosis, age and time living with pain. Most of the informants were women, reflecting the chronic pain population. Gender might influence expectations and experience in neck or back pain (39); but the one male informant in our study had a rich narrative, with experience similar to those of the women. Only 2 informants from outside Europe were included due to the language-related inclusion criterion. Their experience was similar to the other informants’, but other immigrants might have different experiences (7).
Several techniques were used during data collection and analysis to ensure trustworthiness.
To increase the credibility of the results (40), triangulation by researchers with various professional and research perspectives was used. AH is a nurse with many years’ experience of working with persons with chronic pain, working in the department where the study was performed. ML is a physiotherapist, specialist in pain and pain treatment and experienced in qualitative research. BMS is a physician, specialist in rehabilitation medicine and experienced in rehabilitation research, and CS is a professor and physician, specialist in anaesthesia. The authors’ discussions about pre-understanding during the data collection and analysis ensured neutrality.
The implications of these findings for clinicians are that healthcare professionals using MMR could help patients with chronic pain to find their own strength and responsibility by providing explanations of the pain. The encounters should be considered and developed for the purpose of empowering individuals. Fellow patients’ roles should be taken into account in the change process when planning group interventions.
Our findings connect well with the theory of integration and confirm the value of applying the theory in order to understand individuals with chronic pain. The theory can be useful in the further development of care for patients with chronic pain as well as in the training of healthcare teams.
Future studies are needed to increase knowledge of patients’ experience of rehabilitation. In addition to pain diagnoses, age, gender and ethnicity are important areas to explore further.
In conclusion, by integrating their illness, individuals with disabling chronic pain can create a better life. A prerequisite is that healthcare professionals in their encounters empower patients to develop the strength to take responsibility for their daily lives. Treatment and support from significant others facilitate this process.
AcknowledgementS
The authors would like to thank the informants who shared their personal experiences, the Pain Clinic at the Department of Anesthesia and Intensive Care at Södersjukhuset, the Scandinavian Association for the Study of Pain (SASP), Swedish nurses with special interest in pain (SSOS), the Swedish Society of Nursing, and the Stockholm County Council Fund for Care Development for supporting this project.
References

