Lauren Reid, MD1, Penny Thomson, BSc2, Markus Besemann, MD3 and Nancy Dudek, MD, MEd1
From the 1Department of Medicine, Division of Physical Medicine and Rehabilitation, The Ottawa Hospital Rehabilitation Centre, University of Ottawa, 2University of Ottawa, Faculty of Medicine and 3Department of Rehabilitation Medicine, Canadian Forces Health Services, Ottawa, Canada
OBJECTIVE: Assessing a patient’s ability to walk the distance required for community ambulation (at least 300 m) is important in amputee rehabilitation. During the 2-min walk test, most amputees cannot walk 300 m. Thus, the 6-min walk test may be preferred, but it has not been fully validated in this population. This study examined the convergent and discriminative validity of the 6-min walk test and assessed whether the 2-min test could predict the results of the 6-min test.
METHODS: A total of 86 patients with unilateral or bilateral amputations at the Syme, transtibial, knee disarticulation or transfemoral level completed the 6-min walk test, 2-min walk test, Timed Up and Go test, Locomotor Capabilities Index version 5, Houghton Scale of Prosthetic Use, and Activity-Specific Balance Confidence scale.
RESULTS: The 6-min walk test correlated with the other tests (R = 0.57–0.95), demonstrating convergent validity. It demonstrated discriminative validity with respect to age, aetiology of amputation, and K-level (p < 0.0001). The 2-min walk test was highly predictive of the 6-min walk test distance (R2 = 0.91).
CONCLUSION: The 6-min walk test is a valid measure of amputee ambulation. However, the results suggest that it may not be necessary, since the 2-min walk test strongly predicts the 6-min walk test. Clinicians could therefore save time by using the shorter test.
Key words: amputation; rehabilitation; ambulation; mobility; outcome assessment.
J Rehabil Med 2015; 47: 00–00
Correspondence address: Lauren Reid, Room 1200, 505 Smyth Road, Ottawa, Ontario, K1H 8M2, Canada. E-mail: laurenreid @rogers.com
Accepted Sep 10, 2014; Epub ahead of print Jan 12, 2015
Introduction
Walking ability “strongly influences a patient’s personal independence” (1) and is a goal of rehabilitation programmes for lower extremity amputees (LEAs). Community ambulation is “the ability to walk with or without a gait aid to destinations (shops, banks, etc.) important for participation in community life” (2). Researchers have concluded that 300 m is the minimum distance for community ambulation (3–5).
Deathe et al. (6) assessed 17 outcome measures used to assess aspects of LEA mobility that had published psychometric data. Each measure was assigned a rating from 0 (no formal published psychometric data) to 4+ (extensively validated and widely used). These measures include self-reported, amputation-specific rating scales, such as the Locomotor Capabilities Index version 5 (LCI-5), Houghton Scale of Prosthetic Use, and Activity-Specific Balance Confidence (ABC) scale (6). Four walk tests were assigned at least 2+ (minimal validity): the 10-M Walk Test, the Timed Up and Go test (TUG), the L-test, and the 2-Min Walk Test (2MWT) (6). However, none of these walk tests measures the distances required for community ambulation. The longest of the tests is the 2MWT, in which LEAs walk mean distances of up to 140 m (7–9).
The 6-Min Walk Test (6MWT) was not included in the study by Deathe et al. Many clinicians use the 6MWT in LEAs to assess longer walking distance ability, since 6 min allow LEAs to achieve distances greater than 300 m (10, 11). The 6MWT is widely used in cardiovascular and respiratory patients (12, 13) and in muscular dystrophy (14), spinal cord injury (15) and stroke populations (16).
The reliability of the 6MWT has been established for LEAs, with published test-retest reliabilities greater than 0.9 (10, 17). In addition, the 6MWT correlates moderately with the TUG test and the timed 1-leg balance test, suggesting some convergent validity (17). In 1 study (10), the minimal detectible change was calculated as 34.3 m for the 2MWT and 45.0 m for the 6MWT. Patients assigned different K-levels (measures of potential functional ability) achieve significantly different distances on the 6MWT (p < 0.0001), demonstrating some discriminative validity (11).
However, to establish the 6MWT as a valid measure in LEAs requires additional work. Evaluation of discriminative validity should be repeated and expanded, and convergent validity needs to be more fully demonstrated.
Therefore, the first objective of this study is to further validate the 6MWT by examining its convergent and discriminative validity. Based on previous work, we hypothesize that the 6MWT will demonstrate good convergent and discriminative validity, enabling clinicians to use it confidently in LEAs.
In our healthcare environment it would be more cost-effective if a shorter test could be used to assess community ambulation distance potential. There is some indication that the 2MWT provides sufficient information to assess community ambulation distances in other patient populations. Studies of multiple sclerosis and respiratory patients have demonstrated a strong association between the 2MWT and the 6MWT (18, 19), suggesting that no additional information is gained from the additional time required by the 6MWT.
Therefore, the second objective of this study is to determine whether the 2MWT is a valid assessment of community ambulation distances, by assessing the ability of the 2MWT to predict the results of the 6MWT in LEAs.
Methods
The study was approved by The Ottawa Hospital Research Ethics Board.
Setting and participants
Participants were recruited from the outpatient amputee clinic at The Ottawa Hospital Rehabilitation Centre. Participants included in the study were at least 18 years old, had a lower extremity amputation at the Syme, transtibial, transfemoral or knee disarticulation level, and used a prosthesis. Participants had unilateral or bilateral amputations. Participation required sufficient literacy in English or French to complete questionnaires. Participants were excluded from the study if they were unable to provide informed consent due to cognitive impairment, or if they had a medical condition that precluded them from completing the mobility tests.
A total of 86 participants with lower extremity amputations were tested. The demographics of the sample are shown in Table I. Of the 3 participants with bilateral amputations, all had bilateral transtibial amputations.
|
Table I. Participant demographics |
|||||
|
|
K1 |
K2 |
K3 |
K4 |
Total |
|
Male |
2 |
22 |
22 |
20 |
66 |
|
Female |
1 |
5 |
12 |
2 |
20 |
|
Total |
3 |
27 |
34 |
22 |
86 |
|
Age at study entry, years, mean (SD) |
72.7 (7.0) |
66.9 (10.1) |
58.7 (13.9) |
45.0 (12.7) |
60.0 (15.3) |
|
Aetiology of amputation |
|
|
|
||
|
Trauma |
1 |
8 |
15 |
17 |
41 |
|
Vascular |
2 |
8 |
11 |
0 |
21 |
|
Diabetes including peripheral vascular disease |
0 |
5 |
4 |
0 |
9 |
|
Cancer |
0 |
1 |
2 |
2 |
5 |
|
Congenital |
0 |
1 |
0 |
3 |
4 |
|
Infection |
0 |
4 |
2 |
0 |
6 |
|
Level of amputation |
|
|
|
|
|
|
Syme |
0 |
0 |
0 |
4 |
4 |
|
Transtibial |
2 |
22 |
24 |
15 |
63 |
|
Knee disarticulation |
0 |
0 |
2 |
1 |
3 |
|
Transfemoral |
1 |
5 |
6 |
1 |
13 |
|
Bilateral |
0 |
0 |
2 |
1 |
3 |
|
K1: restricted to household ambulation; K2: can traverse low-level environmental barriers and is considered a limited community ambulator; K3: community ambulator able to traverse most environmental barriers; K4: exceeds basic ambulatory skills and can perform higher-level activities. SD: standard deviation. |
|||||
Protocol
Testing was carried out from May to December 2013. Informed consent, including acknowledgement that participation was voluntary, was obtained prior to testing. On the day of testing, the investigators recorded the level and aetiology of amputation, the use of gait aids, and the age and sex of the participant. If invasive infection was the primary cause of the amputation (e.g. meningococcal infection, necrotizing fasciitis), the aetiology of their amputation was classified as infection. Participants who had diabetes with a secondary infection were placed into the diabetes category.
Prior to testing, participants were assigned a K-level by their treating physiatrist and the principal investigator, based on records from the most recent clinic visit. If there was a discrepancy in the K-level assigned, consensus was reached by discussion and review of the participant’s chart before testing. K-levels were developed by the American Medicare system whereby clinicians assign patients to 5 potential functional levels, or K-levels, that determine funding and prosthetic component selection. K-levels have also been used for research purposes (K0 = non-ambulator; K1 = restricted to household ambulation; K2 = can traverse low-level environmental barriers and is considered a limited community ambulator; K3 = community ambulator able to traverse most environmental barriers; K4 = exceeds basic ambulatory skills and can perform higher-level activities) (20, 21).
Participants performed several tests over a period of 1–2 h. They were allowed to use their usual gait aid. They completed the 6MWT, the 2MWT and the TUG test for objective measures of walking ability. The tests were performed in random order as determined by a random number generator, with 20 min rest in between. The 6MWT was conducted according to American Thoracic Society guidelines, in which patients are allowed to stop and rest at any time during the test. Participants walked between pylons separated by 30 m for the duration of the test (22). If participants needed to sit down, the test was considered complete at that point, and the distance they had walked up to that point was recorded. The 2MWT was conducted similarly, following a standardized protocol as described by Brooks et al. (7), where subjects were asked to walk as far as they could in 2 min without further encouragement. The test administrator walked behind the participant to minimize pacing, and participants were provided with clear instructions and were allowed to stop and rest. The test ended if the participant needed to sit down (8). Distances for the 2MWT and 6MWT were recorded to the nearest 0.1 m using a precimeter.
The TUG test was conducted according to the protocol described in Schoppen et al., 1999, whereby the participant started sitting in a standard arm chair. On the word “Go” the participant stood, walked to a line on the floor 3 m away, turned, walked back to the chair, and sat down again (23). Times were recorded to the nearest 0.1 s.
Participants also completed the Houghton Scale, the LCI-5, and the ABC Scale. The Houghton Scale quantifies prosthetic use by time, context, ambulatory aids and confidence over variable terrain (24). The LCI-5 measures ambulatory skill as perceived by the participant (25). The ABC scale is a 16-item self-report questionnaire that measures an individual’s balance confidence when performing various activities (26). Participants’ scores were recorded on the day of testing.
Analysis
Data analysis was completed in Excel 2010. A power calculation was performed prior to recruitment for the primary outcome measures of convergent validity and discriminative validity by K-level; other measures were considered secondary and included for completeness. The goal of recruitment was 61 participants to demonstrate convergent validity and 100 to determine discriminative validity. A total of 86 participants were recruited within the study period. Distributions of continuous measures were assessed graphically, and were found to be approximately normally distributed.
Mean participant age and standard deviation (SD) were calculated for each K-level group.
Convergent validity exists when the results of 1 test are consistent with another instrument attempting to measure the same properties (27). As reported in previous rehabilitation outcome measures (6, 28), convergent validity is considered excellent if R (correlation coefficient) is greater than 0.60, adequate if R is between 0.31 and 0.59, and poor if R is less than 0.3. The 6MWT result for each participant was correlated with the results of the 2MWT, the TUG, the Houghton Scale, the LCI-5 and the ABC Scale, using Pearson’s correlation coefficients.
Discriminative validity is the ability of a measure to differentiate between patient groups and identify meaningful differences in patients’ abilities (29). Participants were sub-grouped based on K-level, aetiology, level of amputation, age and sex. Mean 6MWT distances and standard deviation for each sub-classification were calculated. An analysis of variance (ANOVA) was used to test differences between groups based on K-level, aetiology of amputation, age and sex. For the ANOVA calculations, subgroups of less than 5 were aggregated with appropriate adjacent subgroups.
Regression analysis was used to assess the relationship between the 2MWT and the 6MWT for the entire group and key subgroups. Mean absolute error was calculated for each equation.
Results
Analysis of Six-Minute Walk Test validity
Table II illustrates the convergent validity of the 6MWT by presenting the correlations between the 6MWT and the 5 other tests. Most correlations are excellent, with R between 0.60 and 0.95 (p < 0.0001). The Houghton Scale (R = 0.57) is an adequate correlation. As expected, the 6MWT is more highly correlated with the other performance tests (the 2MWT and TUG) and slightly less correlated with the self-report measures. These correlations suggest that the 6MWT has good convergent validity when used in the LEA population.
|
Table II. Convergent validity of the 6-min walk test (6MWT) |
|||
|
6MWT R |
R2 |
p-value |
|
|
2MWT |
0.95 |
0.91 |
< 0.0001 |
|
TUG |
–0.72 |
0.52 |
< 0.0001 |
|
LCI-5 |
0.61 |
0.38 |
< 0.0001 |
|
Houghton |
0.57 |
0.33 |
< 0.0001 |
|
ABC |
0.60 |
0.36 |
< 0.0001 |
|
2MWT: 2-min walk test; TUG: Timed Up and Go test; LCI-5: Locomotor Capabilities Index version 5; ABC: Activity-Specific Balance Confidence scale; Houghton: Houghton Scale of Prosthetic Use. |
|||
The 6MWT was also evaluated with regard to discriminative validity. The mean 6MWT distances for each subgroup were calculated and the results are shown in Table III. An analysis of variance (ANOVA) was performed and showed statistically significant between-group differences in the 6MWT distances based on the aetiology of amputation, K-level and age (p < 0.0001). The p-level and F-statistic for each ANOVA is included in the table. Between-group differences trend towards significance for sex, with males walking further than females (p = 0.24). For level of amputation only the mean and standard deviation are presented as it is not appropriate to collapse Syme or knee disarticulation level amputees, or bilateral amputees, with other groups. In general, amputees with lower levels of amputation walked further.
|
Table III. Discriminative validity of the 6-Min Walk Test (6MWT) |
||
|
Patients n |
6MWT distance, m Mean (SD) |
|
|
K-level (p < 0.0001, F = 3.1) |
||
|
K1 and K2 |
30 |
271.8 (96.3) |
|
K3 |
34 |
408.2 (82.5) |
|
K4 |
22 |
540.4 (79.3) |
|
Aetiology of amputation (p < 0.0001, F = 2.5) |
||
|
Diabetes |
9 |
256.1 (122.0) |
|
Infection (not related to diabetes) |
6 |
261.4 (76.3) |
|
Vascular disease |
21 |
345.1 (104.4) |
|
Cancer |
5 |
444.6 (88.9) |
|
Trauma and congenital |
45 |
457.3 (120.1) |
|
Age (p < 0.0001, F = 3.9) |
||
|
≥ 50 years |
63 |
350.9 (115.6) |
|
< 50 years |
23 |
513.6 (112.5) |
|
Sex (p = 0.24, F = 3.9) |
||
|
Female |
20 |
373.9 (106.7) |
|
Male |
66 |
400.6 (43.5) |
|
Amputation level |
||
|
Syme |
4 |
503.4 (100.9) |
|
Transtibial |
63 |
383.1 (136.7) |
|
Knee disarticulation |
3 |
441.0 (98.3) |
|
Transfemoral |
13 |
343.0 (82.8) |
|
Bilateral |
3 |
451.4 (111.2) |
|
K1: restricted to household ambulation; K2: can traverse low-level environmental barriers and is considered a limited community ambulator; K3: community ambulator able to traverse most environmental barriers; K4: exceeds basic ambulatory skills and can perform higher-level activities. |
||
Analysis of the predictive ability of the two-minute walk test
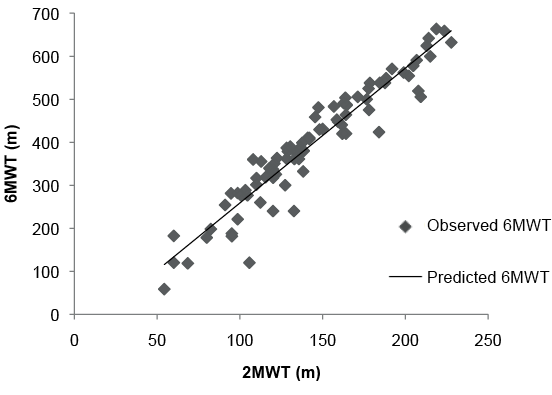
The relationship between the 2MWT distance and the 6MWT distance was assessed using regression analysis (Fig. 1), and the predictive equation found was 6MWT (m) = 3.14 (2MWTm) – 54.5. The predictive ability of this equation was excellent, with an R2 of 0.91, meaning that 91% of the variance in the 6MWT distance was explained by the 2MWT. The error of the equation was calculated by subtracting the predicted 6MWT distance from the actual 6MWT distance for each participant. The mean absolute error for the prediction equation in the study population is 29.6 m (SD 27.9).
Subgroup analysis
Since lower extremity amputees make up a heterogeneous patient population, a subgroup analysis was performed to assess the 2MWT ability to be predictive of the 6MWT for different participant subgroups (Table IV). The subgroup prediction equations, as well as the mean absolute error for each equation are represented in Table IV. Based on sample size, the global prediction equation has the strongest generalizability, but the subgroup equations are included for interest and completeness.
|
Table IV. Relationship between 2-Min Walk Test (2MWT) and 6-Min Walk Test (6MWT) |
|||
|
Group (n) |
Correlation strength (R2) |
Prediction equation |
Mean absolute error of equation (m) |
|
Full sample (86) |
0.91 |
6MWT = 3.1 (2MWT) – 54.5 |
29.6 |
|
K1 and K2 (30) |
0.79 |
6MWT = 3.2 (2MWT) – 75.8 |
32.1 |
|
K3 and K4 (56) |
0.87 |
6MWT = 2.8 (2MWT) – 1.6 |
25.2 |
|
Vascular (21) |
0.82 |
6MWT = 4.0 (2MWT) – 177.4 |
29.9 |
|
Trauma (41) |
0.89 |
6MWT = 2.8 (2MWT) – 5.8 |
25.8 |
|
K1: restricted to household ambulation; K2: can traverse low-level environmental barriers and is considered a limited community ambulator; K3: community ambulator able to traverse most environmental barriers; K4: exceeds basic ambulatory skills and can perform higher-level activities. |
|||
The 30 participants assigned K-levels of 1 and 2 were grouped together, representing those with lower functional ambulation potential. Linear regression showed an excellent predictive relationship (R2 = 0.79). The 56 higher potential ambulators, K-levels 3 and 4, were also grouped, and an excellent predictive relationship was demonstrated (R2 = 0.87).
Participants were also subgrouped based on aetiology of amputation. The 41 participants who had an amputation as a result of trauma also demonstrated an excellent predictive relationship between the 2MWT distance and the 6MWT distance (R2 = 0.89). In those who had an amputation as a result of vascular disease (n = 21), there was also an excellent predictive relationship (R2 = 0.82).
Discussion
Overall, this study demonstrated adequate to excellent correlation between the 6MWT and previously validated measures of ambulation in lower extremity amputees. It also found that the 2MWT was strongly predictive of the 6MWT distance in this population, suggesting that, for LEAs, the longer test is not needed to assess the ability to walk the distances required in the community.
The first objective, to further validate the 6MWT by examining its convergent and discriminative validity, was a necessary first step, given the limited number of studies assessing the reliability and validity of the 6MWT in lower extremity amputees (10, 11, 17). As the results indicate, there was sufficient sample size to demonstrate significant differences between K-level groups and convergent validity. This study demonstrates adequate to excellent correlation for the results of the 6MWT compared with several previously validated measures in LEAs. All of the correlations were statistically significant. As expected, the 6MWT best correlated with the other objective walking tests (2MWT and TUG). These correlations suggest that the 6MWT has good convergent validity in LEAs.
The results of the study also suggest that the 6MWT has good discriminative validity. The study found statistically significant between-group differences in the 6MWT distances based on aetiology of amputation, K-level and age. When divided by K-level, the mean K-level 1 and 2 participant (limited community ambulator) did not reach the 300 m threshold for community ambulation, whereas the participants considered completely functional community ambulators (K-levels 3 and 4) were able to walk further than 300 m in the 6MWT.
As has been shown in previous examinations of the 6MWT (30), men walked further than women. This result was not statistically significant in the present study. It is likely that this study was not adequately powered to demonstrate this difference as this was a secondary outcome measure.
When testing for the 6MWT’s ability to discriminate between patients with different levels of amputation, generally those with lower levels of amputation were able to walk further. This study was not sufficiently powered to detect this secondary measure, given the relatively small number of participants with knee disarticulation level and bilateral amputations. Due to the small numbers in each group, only means and standard deviations were reported in Table III. The 3 participants with knee disarticulation amputations were all K-level 3 and 4 ambulators and, not surprisingly, were able to walk greater distances than the average participant with a transtibial amputation, since the transtibial amputation group (n = 66) included a much more representative sample of varying ambulation abilities. Moreover, the 3 bilateral transtibial amputees were K-level 3 or 4, which explains their longer distance compared with the unilateral transtibial amputee group. A larger sample, probably achievable only in a multicentre study or with a much longer collection period, may have access to a more diverse population of knee disarticulation and bilateral amputees and may statistically demonstrate discrimination based on level of amputation.
Given the previously published literature (10, 11, 17) and these results, we believe that there is sufficient evidence to support the use of the 6MWT in LEAs. The level of validity evidence is now comparable to that described for the TUG, L-test, 10-m test and 2MWT in LEAs (6), and we suggest that the 6MWT be considered on par with these tests as valid measures of ambulation in LEAs.
The second objective of this study was to determine whether the 2MWT is a valid assessment of the potential for community ambulation distance by assessing the 2MWT ability to predict the results of the 6MWT. Many clinicians currently prefer the 6MWT when community ambulation is the ultimate goal of rehabilitation, since a longer walk test allows for sufficient distance to be travelled, despite the increased therapy time to complete the test. However, it would be more efficient to save 4 min and be able to use this time for another test or activity, assuming that no additional information is lost in doing this.
In this study population, the 2MWT distance was so highly predictive of the 6MWT distance that we believe the 2MWT could be used in place of the 6MWT to assess community ambulation distance potential in LEAs. This is a significant result, and echoes similar findings in the respiratory and multiple sclerosis populations (18, 19).
There is inherent error in using a predictive equation, but the question of how much error is acceptable can be challenging for clinicians. Based on their reliability assessment, Resnik & Borgia calculated the minimal detectible change of the 6MWT, or the statistical error of the test, to be 45 m for patients with LEAs (10). By this calculation, clinicians should look for changes greater than 45 m (greater than the error of the test) before concluding that there has been a true change in a patient’s functional status. The mean absolute error in the 6MWT predictive equation produced by this study is 29.6 m (SD 27.8 m), which falls below the 45 m threshold for statistical error in the 6MWT. Thus, clinicians do not need to worry about the small amount of error when using the predicted 6MWT distance.
The prediction equation resulting from this study is 6MWT (m) = 3.14 (2MWTm) – 54.5. This means that a 2MWT distance of ≥ 113 m is required for patients to be likely to walk ≥ 300 m in the 6MWT and demonstrate that they have community ambulation potential with respect to distance.
Given the varied aetiologies and levels of lower extremity amputation, the amputee population is heterogeneous. Hebert et al. describe a bimodal distribution of community dwelling amputees: older individuals with disease-related lower limb amputations and younger, generally healthier, individuals with trauma-related lower limb amputations (31). Distances covered in the 2MWT are too short to measure community ambulation potential, therefore some clinicians use the 6MWT for patients they believe can walk longer distances, e.g. patients who are healthier or who have lower levels of amputation. In this study, however, these higher level ambulators (K-levels 3 and 4) showed the stronger predictive relationship between the 2MWT and the 6MWT. Therefore, given this data, we would suggest that it is not necessary to use the 6MWT in these higher level performers because the 2MWT predicts the 6MWT so well in these populations. We suggest that clinicians use the 2MWT to establish that a patient has community ambulation distance potential. The saved time could be used to test higher level ambulatory skills, such as those assessed by measures such as the Comprehensive High-Level Activity Mobility Predictor (CHAMP) (32).
Very low level participants, such as those with a K-level of 1, were less likely to meet inclusion criteria, and are underrepresented in this study. Thus, caution should be exercised when applying these results to very low functioning amputees. However, when examining our subgroups with lower functional potential (K-levels 1 and 2 and those with amputations caused by vascular disease) the predictive ability of the 2MWT for the 6MWT was still considered excellent. It is notable that the relationship was slightly weaker in the lower functioning groups than in the higher functioning groups. It is possible that endurance is a greater factor in these people, leading to a less predictive relationship. Thus, a clinician may wish to use the 6MWT to measure changes in endurance. However, for most patients, the 2MWT is a robust proxy to measure community ambulation distance potential.
In conclusion, this study demonstrates that the 2MWT result predicts the 6MWT distance in a diverse population of amputees. The 2MWT takes 4 min less time to perform. Therefore, in the assessment of community ambulation distance potential in patients with lower extremity amputations, the shorter test could be a more efficient way to gain the same knowledge, benefiting both the patients and the facilities where they receive care.
AcknowledgementS
The authors would like to thank physiotherapists Sandra Macleod and David Follows for their contributions to the project design and their clinical expertise regarding the participant testing.
This research was supported by funding from the Canadian Forces Health Services, Surgeon General Health Research Project, CIMVHR task 20, and the University of Ottawa Summer Studentship.
References

