Betje Schwarz, DipSoc1,2, Silke Neuderth, PhD3, Christoph Gutenbrunner, MD1 and Matthias Bethge, PhD1,2
From the 1Department of Rehabilitation Medicine, Hannover Medical School, Hannover, and 2Institute for Social Medicine and Epidemiology, University of Lübeck, Lübeck, and 3Department of Medical Psychology, Medical Sociology and Rehabilitation Sciences, University of Würzburg, Würzburg, Germany
OBJECTIVE: Systematic reviews indicate the effectiveness of multimodal rehabilitation. In Germany this has been shown, in particular, for work-related medical rehabilitation. A recently published guideline on work-related medical rehabilitation support the dissemination of these programmes. The feasibility of this guideline was examined in a multicentre study. This paper presents findings on the relevance of multiprofessional teamwork for the implementation of successful work-related medical rehabilitation.
METHODS: Focus groups were conducted with 7 inpatient orthopaedic rehabilitation teams and examined using qualitative content analysis.
RESULTS: Multiprofessional teamwork emerged inductively as a meaningful theme. All teams described multiprofessional teamwork as a work-related medical rehabilitation success factor, referring to its relevance for holistic treatment of multifactorially impaired patients. Although similar indicators of successful multiprofessional teamwork were named, the teams realized multiprofessional teamwork differently. We found 3 team types, corresponding to multidisciplinary, interdisciplinary and transdisciplinary team models. These types and models constitute a continuum of collaborative practice, which seems to be affected by context-related factors.
CONCLUSION: The significance of multiprofessional teamwork for successful multimodal rehabilitation was underlined. Indicators of ideal multiprofessional teamwork and contextual facilitators were specified. The contingency approach to teamwork, as well as the assumption of multiprofessional teamwork as a continuum of collaborative practice, is supported. Stronger consideration of multiprofessional teamwork in the work-related medical rehabilitation guideline is indicated.
Key words: rehabilitation; patient care team; inter-professional relations; qualitative research; focus groups.
J Rehabil Med 2014; 46: 00–00
Correspondence address: Betje Schwarz, Institute for Social Medicine and Epidemiology, University of Lübeck, Ratzeburger Allee 160, DE-23538 Lübeck, Germany. E-mail: betje.schwarz@uksh.de
Accepted Jun 23, 2014; Epub ahead of print Sep 29, 2014
INTRODUCTION
To reduce the risk of health-related early retirement and to promote sustainable participation in employment, most Western welfare systems provide rehabilitation services to help persons with limited work capacity cope with their job demands. Systematic reviews indicate that these programmes and services can increase return-to-work rates and reduce the duration of sick leave, especially when they are following a multimodal approach that combines medical treatment, physical exercise, cognitive-behavioural components, patient education and social counselling (1–3). Given the inherent involvement of different health professions, multimodal programmes and services are also called “multidisciplinary” interventions (2, 3). Following the bio-psycho-social model of functioning (4), their effectiveness is reasoned by the complexity of the underlying chronic health problems, which have both biomedical and psychosocial dimensions of aetiology and persistence and therefore call for a comprehensive treatment strategy (5, 6). Multiprofessional teamwork (MPT) is especially important for the successful implementation of such programmes, since they require a high level of communication, coordination and cooperation among the health professions involved.
Systematic reviews have proven the superiority of multiprofessional, in contrast to mono-professional, rehabilitation strategies (2, 5). However, the mode of organizing multiprofessional strategies can differ markedly. Several authors distinguish between multidisciplinary, interdisciplinary and transdisciplinary teamwork (7) (Table I).
|
Table I. Characteristics of multidisciplinary, interdisciplinary and transdisciplinary team models |
|
Multidisciplinary teamwork |
|
Hierarchically structured: guided by the physician |
|
Each discipline has a defined role and specified tasks |
|
Disciplines working independently of each other, in parallel or sequentially |
|
Discipline-related treatment goals and strategies |
|
Minimum of communication and coordination among the disciplines |
|
Only problem cases are discussed in team meetings |
|
Interdisciplinary teamwork |
|
Flat hierarchies/stronger equality |
|
Higher degree of communication and cooperation among the disciplines |
|
Regular team meetings |
|
Collaborative setting of treatment goals and strategies |
|
Joint intervention |
|
Transdisciplinary teamwork |
|
Shared responsibilities |
|
Highest degree of communication and cooperation among the disciplines |
|
Joint setting of treatment goals and strategies |
|
Transfer of knowledge and skills |
|
Blurring of and working across disciplinary boundaries |
Recent findings indicate that the decision to use a certain team model may affect the effectiveness of rehabilitation programmes, as interdisciplinary and transdisciplinary teams appear to be more effective than multidisciplinary teams (7–9).
In addition, the so-called “contingency approach to teamwork” states that situational variables, such as the complexity of the client’s problem, may determine the adequacy of a particular team model and probably moderate its effectiveness (7, 10, 11). Consequently, transdisciplinary and interdisciplinary teamwork are particularly necessary when the client’s problem is highly complex (7, 10, 11). Furthermore, effective teamwork can be promoted or hindered by different context-related factors (e.g. team size, number of treated cases, physical proximity of team members, time for, and remuneration of, team meetings) in daily routine (7, 12). Team development strategies therefore also need to consider organizational development issues.
In Germany, rehabilitation services for people of working age are provided mainly by the German Pension Insurance (GPI) and, as in many Western countries, a chronic musculoskeletal disorder (CMSD) is the most common reason for rehabilitation (13). Case-cohort studies on patients with CMSD revealed that persons with long-term sick leave and poor return-to-work expectations (e.g. severe limitations in work-related activities and participation) do not benefit sufficiently from conventional German medical rehabilitation programmes (14, 15). Following principles of functional restoration (16) and work hardening (17), work-related medical rehabilitation (WMR) programmes have been developed over the last 20 years to improve these patients’ work-related outcomes (18). On the basis of intensified work-related diagnostics focusing on individual job demands, these multimodal programmes complement conventional medical and physical interventions with social counselling, work-related psychological groups and work-related functional capacity training (16–18). Corresponding to international evidence regarding the effectiveness of work-related interventions (1, 3, 17), randomized controlled trials confirmed the effectiveness of WMR programmes regarding diverse health and work-related outcomes (14, 15). To disseminate these findings, the GPI published a WMR guideline (19). Although the implementation of WMR poses specific requirements on multiprofessional teamwork, MPT was hardly addressed in this guideline.
The feasibility of the implementation of WMR according to the guideline was examined in a multicentre trial funded by the GPI. Seven purposively selected inpatient orthopaedic rehabilitation centres took part in the formative evaluation based on a mixed-method approach. This paper presents findings of focus groups with the participating WMR teams, conducted to explore the experiences of the teams regarding the implementation of WMR programmes. More precisely, the paper focuses on intra-organizational MPT in WMR. This topic had emerged inductively as a meaningful theme during data analysis. In particular, our analysis answered the following questions:
• What relevance has MPT for the implementation of a WMR programme?
• What are the implications of the implementation of a WMR programme for MPT?
• What are indicators of successful MPT in WMR (i.e. “ideal” MPT)?
• How is MPT realized in daily routine and what mode of MPT is practiced?
• Which context-related factors are associated with the (non-)realization of ideal MPT in WMR?
METHODS
As mentioned above, MPT in WMR was not a primary research topic. It emerged rather as a meaningful theme during the qualitative part of a larger feasibility study conducted between October 2010 and May 2012. Ethical approval for this study was obtained from the Hannover Medical School (858/2010). For transparent presentation of methods and findings, a draft of this paper was guided by the Consolidated Criteria for Reporting Qualitative Research (COREQ) statement (20).
Data collection
Seven focus groups (21) were conducted with the WMR teams of the participating orthopaedic rehabilitation centres. The topic guide used to moderate the focus groups contained questions referring to the following main topics:
• WMR target group identification and referral
• WMR programme
• Implementation and evaluation of the WMR guideline
• Effort and remuneration
• Wishes regarding the assigning pension insurance agency
• Challenges and operative requirements regarding further dissemination of WMR.
The focus groups were moderated by the first author (B.S.), a female sociologist with comprehensive experiences in conducting and analysing focus groups. She worked as a researcher at a university hospital at the time of the study and had no contact with the participating teams prior to the study. Focus group size varied from 6 to 11 participants, including representatives of all relevant health professions (physicians, psychologists, social workers, physiotherapists, occupational therapists and sport therapists), and sessions lasted approximately 2.5 h. Six rehabilitation centres consented to audio-recording and subsequent transcription of their focus groups. The seventh centre hired a professional steno-typist to prepare a report on the focus group, an additional team conference and visitations of single WMR interventions. Thus, 6 transcripts and 1 report were used for the analysis. All sensitive data were rendered anonymous.
Data analysis
Software-supported (MAXQDA) structuring qualitative content analysis (22) was carried out by the first author using an unconstrained categorization matrix (23). Within the matrix, the above-mentioned main topics of the discussion guide were used as deductive categories representing the study objectives. This provided a structuring framework for coding the individual focus groups, which was enriched with inductively generated subcategories, further main categories and category dimensions during our analysis. The enriched category matrix, case memos, systematic retrieval of text passages and in-depth analysis of selected topics formed the basis for comparative analysis of the focus groups. The research progress and results were discussed continually within the research group and regular scientific advisory board meetings.
RESULTS
MPT emerged inductively as a meaningful theme and was therefore included in the unconstrained categorization matrix as a main category with the following subcategories: relevance of MPT in WMR; team development by WMR implementation; indicators of successful MPT in WMR; realization of MPT in daily routine; and structural and organizational context-related factors influencing MPT (cf. the 5 questions presented in the introduction). In-depth comparative analysis findings of the “team topic” will be presented below according to these subcategories and illustrated using selected quotes from participants in the focus groups.
Relevance of multiprofessional teamwork in work-related medical rehabilitation
All teams emphasized the outstanding importance of MPT in WMR, referring to its essential value for need-oriented treatment of the target group. Since, according to a sports therapist, the target group is characterized by “severe limitations in different [bio-psycho-social] dimensions”, holistic treatment that combines the expertise of different professions (physicians, psychologists, social workers, physiotherapists, occupational therapists, sport therapists) is needed.
Physician: “It is a really great, gathering all the knowledge and experience from the different disciplines. This is enriching, especially with regard to understanding the patients’ problems, because each discipline has made different observations.”
In this respect, an effective WMR programme requires a high level of communication and exchange, as well as close cooperation between the different disciplines.
Social worker: “It is the communication between the relevant professions that is decisive during the 3 weeks of treatment.”
Hence, MPT was described by the practitioners as an important WMR success factor.
Physiotherapist: “It is very important that we work according to the bio-psycho-social model […]. Therefore, it is probably the interdisciplinary teamwork […] that generates the desired effects.”
Team development as a result of work-related medical rehabilitation implementation
The teams reported that the implementation of a WMR programme initiated a team-building process, since conventional medical rehabilitation does not require such extensive and intensive multiprofessional teamwork. They described, in detail, an increase in multiprofessional communication and exchange, accompanied by strengthening of the individual professions, cross-disciplinary learning, and a culture of mutual trust, respect and recognition.
Physician: “Well, in the beginning, some of our medical colleagues had difficulties accepting that they had to decide within the team [...]. It took some time until this was accepted.”
Sports therapist: “With the implementation of such concepts [WMR], they [physiotherapists] had to broaden their perspectives. This was an advantage for me and my colleagues because it improved our standing.”
Indicators of successful multiprofessional teamwork in work-related medical rehabilitation
The following 7 aspects were described as indicators of successful teamwork in WMR:
(i) Participation in conceptual work – creating a holistic programme and growing together as a team. According to the teams, MPT should ideally start while developing a WMR concept. Expertise and experience of the different professions are needed to create a holistic WMR programme. Furthermore, acceptance of, identification with, and commitment to, the programme increases when a WMR philosophy is developed within the team.
Physician: “I think it is very important that the team members have the opportunity to create and further develop the programme. […] It makes a difference. The programme is filled with life then.”
The teams identified an additional advantage of early involvement. When MPT is practiced during the conceptual planning stage, the team will already have grown together by the time the programme is implemented into daily routine.
(ii) Multiprofessional diagnostics – getting the whole picture. The teams stressed that multiprofessional diagnostics and assessment is the only way to obtain a comprehensive picture of the patient’s limitations. Therefore, it is the basis of holistic and effective treatment.
Physiotherapist: “[This means].. that we can put together the pieces of the patient’s puzzle … [and see] the medical and psychological aspects, as well as those from the practical field.”
Moreover, this deepens and enlarges the team’s practical and theoretical knowledge on the WMR target group. By discussing findings within the team, each profession gains further insights into the work of the other professions. This promotes mutual recognition as well as cross-disciplinary learning.
(iii) Participation in treatment planning and management – establishing joint treatment goals and strategies. The teams specified the participation of all professions in treatment planning and management as a further indicator of effective MPT. They stressed that comprehensive treatment goals and strategies should be jointly defined. Furthermore, discipline-related goals and strategies should be coordinated within the team. The agreed goals and strategies should be monitored and mutually adjusted during the rehabilitation process. One physiotherapist pointed out “[…] how important it is to have a common goal […] defined in a team meeting. It is important that the goal is not only mine, but also that of the others.”
(iv) Joint treatment provision – working together rather than in parallel. The teams underlined the significance of working together in therapeutic interventions rather than working independently, in parallel, not really knowing what the other professions do. Synergetic effects and a successful treatment need continuous cross-disciplinary exchange and synchronized actions.
Physiotherapist: “We must act in concert; when we do, we have a good outcome.”
(v) Regular team meetings – providing opportunities for communication, coordination and exchange. Regarding cross-disciplinary exchange and concerted actions, the teams emphasized the significance of regular team meetings in which all team members come together to discuss patients (case conferences), problems or open questions in a structured manner.
Psychologist: “We implemented special WMR team meetings, which improved cross-disciplinary exchange a lot.”
In addition to team meetings, other ways of communication, such as e-mail, phone calls or personal consultations with other team members, should ideally contribute to achieving an overall high communication density.
(vi) Common language and shared knowledge – becoming WMR specialists. The teams stressed the significance of having a common language and shared knowledge as an indicator of, and prerequisite for, effective MPT in WMR.
Director: “It is crucial that everyone speak the same language.”
Technical jargon and knowledge should not create barriers to cooperation. Therefore, it is important that the individual team members are not only experts in their fields, but also open to acquiring cross-disciplinary competences.
Physician: “[It is important] that you can contribute input and be a partner on equal footing.”
Ideally, the team should generate knowledge that crosses disciplinary boundaries. In this way, the individual team members become WMR specialists and are no longer just members of a given profession.
(vii) Flat hierarchies – creating greater equality and shared responsibility. The previously described indicators already contain another aspect that was mentioned by the teams: greater equality. This implies a shift from authoritarian team structures towards flat hierarchies, shared decision-making and shared responsibility.
Realizing multiprofessional teamwork in daily routine
Compared with the ideal, the focus groups revealed that MPT was realized quite differently in the daily routine of the 7 teams. Based on 3 aspects – treatment planning and management, provision of services, and communication practice – we distinguished 3 types of teams: “Consultative involvement” (2 out of 7 teams), “Inclusive participation”(3 out of 7 teams) and “Joint performance”(2 out of 7 teams). These types are described and illustrated by quotations in Tables II–IV. Direct comparison of the 3 types shows that the extent and intensity of MPT increase from types 1 to 3. Furthermore, the reported characteristics of successful MPT are performed at a higher level.
|
Table II. Type 1 teams – “Consultative involvement” |
|
|
Treatment planning and management |
Based on an examination at the beginning of rehabilitation, the physician identifies rehabilitation goals and strategies and establishes a rehabilitation plan for each patient. In 1 out of 2 teams, a social worker explores supplemental information that helps selecting an individual or subgroup-specific combination of work-related medical rehabilitation (WMR) interventions. Other professions are only involved in problematic cases. Each profession determines its own discipline-related treatment goals and strategies, which must be adjusted to the rehabilitation plan. All information about the treatment flows together on the desk of the physician who makes the final evaluation of the patient‘s working capacity at the end of rehabilitation. |
|
Communication practice |
The physician consults other disciplines only in problematic cases in a bi- or multiprofessional manner. There are no regular multiprofessional WMR team meetings and therefore little multiprofessional exchange. The communication density between the different professions is low to moderate. |
|
Provision of services |
Each profession contributes to the treatment process independently. Only in problematic cases are these contributions discussed and synchronized. Further coordination and integration only result from the underlying WMR concept and the physician‘s rehabilitation plan. Overall, their approach to providing treatment can be described as professions working in parallel, with all professions adding their own discipline-specific contributions, the sum of which yields the treatment as a whole. |
|
Quotes |
Physician: “The most important thing is that all information flows to the ward physician, because he is the contact person for the patient and the one who has to write the discharge letter at the end of rehabilitation.” Physician: “We have 12 ward physicians, 7 psychologists and 30 therapists. [….] Therefore, it would not be reasonable to have team meetings. The actual work would be totally disrupted. Moreover, not every staff member treats or knows each of our patients. … They could not join in the conversation anyway.“ |
|
Table III. Type 2 teams – “Inclusive participation” |
|
|
Treatment planning and management |
Based on a more multiprofessional diagnostic workup at the beginning of rehabilitation (including psychologists and social workers and/or physiotherapists in some cases), both general and discipline-related rehabilitation goals and strategies are discussed and synchronized within the team. All professions participate in developing and determining the rehabilitation plan. Information about the treatment is centralized. Since the information is not collected electronically, it can only be used by 1 person at a time. At the end of rehabilitation, the attending physician evaluates the patients‘ working capacity in agreement with the team. |
|
Communication practice |
There are regular multiprofessional work-related medical rehabilitation team meetings in which all relevant cases are discussed. In addition to these multiprofessional team meetings, communication and exchange between the professions takes place bilaterally via telephone and e-mail and, occasionally, in face-to-face conversations. The communication density between the different professions is higher in type 2 teams than in type 1 teams. |
|
Provision of services |
The contributions of the single professions are coordinated and concerted within the teams, reflecting their participatory approach to working together and providing treatment services. Since this multiprofessional cooperation and exchange results in synergetic effects, the treatment is more than just the sum of its individual parts. |
|
Quotes |
Occupational therapist: “I personally consider the team both important and absolutely appropriate. Information can be merged and we are able to get the best out of it for the patient.” Physician: “It is incredibly relieving when you are not alone with the patient and the responsibility.“ |
|
Table IV. Type 3 teams – “Joint performance” |
|
|
Treatment planning and management |
All decisions are made in mutual agreement, and responsibilities are shared more equally. At the beginning of rehabilitation, each profession carries out an examination or consultation with each patient. The findings are documented in a common electronic database and discussed within the team. General rehabilitation- and discipline-related treatment goals and strategies are determined by the team, which jointly develops a rehabilitation plan. All information is disseminated within the team. The team members mutually monitor the individual rehabilitation process and adjust the rehabilitation plan if necessary. At the end of the rehabilitation, the patient‘s working capacity is evaluated by the team based on all collected information and data, including a final diagnostic procedure. |
|
Communication practice |
Multiprofessional work-related medical rehabilitation team meetings in which all cases are discussed are held weekly or more frequently if necessary. The common database is used to structure these case conferences, to enrich them with the collected information, and to record the discussed results of the team meetings. Each team member has unrestricted access to the database and can use it at any time to document his or her own work or track the work of colleagues. This allows deeper insight into the work of colleagues from other professions, facilitates exchange and stimulates cross-professional learning. The same effect is reached by direct collaboration of different professions in selected interventions. Further communication and exchange take place bilaterally via telephone and e-mail or, occasionally, in face-to-face conversations. The communication density between the different professions is very high. |
|
Provision of services |
The treatment is jointly provided. The contributions of the different professions are characterized by a high degree of mutual exchange and cooperation. Borders between disciplines are (partly) overcome, which increases synergetic effects. |
|
Quotes |
Excerpt from the report: “There are at least 3 team meetings for each patient. In the initial meeting, the findings of the multiprofessional diagnostic procedure are reported and discussed case-by-case. […] Individual rehabilitation goals and strategies are identified and the rehabilitation plan is determined by mutual agreement. […] Individual rehabilitation processes are discussed in a second team meeting, in which adjustments to the rehabilitation plan are made, if necessary. In the final meeting, the results of the individual interventions and remaining limitations are discussed. Basically, the team evaluates the patient‘s working capacity and return-to-work.“ |
Structural and organizational context-related factors influencing multiprofessional teamwork
The 3 team types were characterized by different structural and organizational context-related factors, which may therefore play an important role in the realization of MPT (Fig. 1).
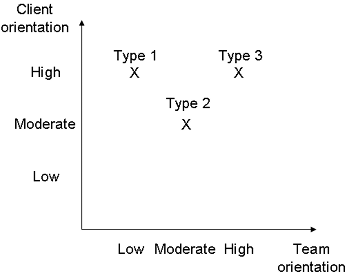
Type 1 teams lacked a structurally or operatively separate WMR department in which WMR cases were clustered and treated by a firmly assigned WMR team. Their treatment programmes were integrated into existing organizational structures (wards, units, staff, etc.) and processes (e.g. communication processes). Therefore, their WMR teams were large and loose. The personnel composition of the team varied from patient to patient. This was perceived as necessary for managing a large number of WMR cases and for considering the heterogeneity of their cases by providing each individual a patient- or subgroup-specific combination of WMR modules. Their structural and organizational context can be described as highly client-oriented, but rarely team-oriented. These conditions seem to hamper the realization of close and successful MPT in WMR.
Type 2 teams had an operatively separate WMR department with a fixed multiprofessional WMR team. In contrast to the others, type 2 teams were medium-sized and dealt with a moderate number of cases. Their WMR patients were clustered in closed groups and completed a standardized multimodal WMR programme. Individual or subgroup-specific needs were considered to a certain extent by modifying single content items and/or by offering additional interventions. One rehabilitation centre had no separate WMR department, but an appointed multiprofessional WMR team, which handled a moderate number of cases. Their programme was semi-standardized: one part was obligatory for all WMR patients, and the other was adjusted to individual or subgroup-specific needs. The structural and organizational context of type 2 teams can be described as moderately client- and team-oriented. These conditions seem to promote close and successful MPT in WMR.
Type 3 teams worked at specialized WMR centres, with all organizational structures and processes focussed on the provision of WMR. Both centres offered a standardized multimodal WMR programme, which was conducted in closed groups and adapted for each patient according to the results of an electronically assisted and constantly updated comparison of work demands and work capacities. As described in Table IV, this assessment and monitoring decisively promoted communication, coordination and cooperation within the multiprofessional WMR teams. These multiprofessional teams treated specifically assigned patients (lowest number of cases) and were the smallest in the sample. Another special context-related factor of type 3 teams was the physical proximity of all team members and professions (next door to each other), which further improved multiprofessional exchange. The structural and organizational context of type 3 teams can be described as highly client- and team-oriented. These conditions seem to be optimal for close and effective MPT in WMR.
DISCUSSION
This study emphasizes the significance of MPT in WMR. It shows that MPT is essential to the implementation of multimodal rehabilitation programmes that aim to provide comprehensive treatment to patients with complex health problems. Furthermore, our findings suggest that it is not only important that but also how MPT takes place. The interviewed teams described 7 characteristics of effective MPT in WMR: broad participation in conceptual work, diagnostic as well as treatment planning and management, joint provision of treatment, regular team meetings, a common language and shared knowledge and, last but not least, flat hierarchies with more equality and shared responsibilities. However, our analysis showed that these indicators were accomplished to a different degree in the teams’ daily routine. We identified 3 team types based on their approaches to treatment planning and management, treatment provision, and communication.
There are different theoretical approaches to distinguishing different modes of MPT in the rehabilitation context. The most common is the above-mentioned differentiation between multi-, inter- and transdisciplinary team models (18). Our team types show strong similarities to, but no congruence with, these team models (Fig. 2).
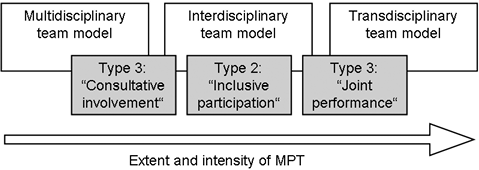
Fig. 2. Relationships between the multidisciplinary, interdisciplinary and transdisciplinary team models and the team types identified here.
Our findings support the assumption that teamwork must be understood as a continuum of the extent and intensity of collaboration (7, 24, 25). The identified team types and established team models can be seen as different points on this continuum.
There are few empirical findings regarding the effectiveness of different team models in medical rehabilitation. Two German studies showed that members of interdisciplinary teams evaluated their team performance better than members of multidisciplinary teams (8, 9). In a Swedish study, team effectiveness ratings were highest among members of interdisciplinary and transdisciplinary teams (7). The findings of the present study correspond to these results with respect to the increasing realization of the identified success factors of MPT in WMR by team type (type 1 < type 2 < type 3). Furthermore, the findings are in accordance with the “contingency approach to teamwork” (7, 10, 11) which suggests that interdisciplinary and transdisciplinary teamwork is particularly necessary when the client’s problem is highly complex.
However, our study showed that not every team was successful in realizing more interdisciplinary or transdisciplinary teamwork. This might be due to the different contexts and frameworks of the 3 team types. Many of these contextual and situational determinants (small team size, team cohesion/stable composition, physical proximity, small numbers of cases, etc.) were found to be promoters of interdisciplinary and transdisciplinary teamwork in other studies (7, 12). This underlines the significance of taking structural and organizational context-related factors into account when analysing or developing MPT.
Some limitations of the study should be mentioned. Firstly, our results refer only to intra-organizational MPT, since inter-organizational MPT or cooperation (for example with employers, the unemployment agency, and general or company physicians) is still the exception, even in the context of WMR.
Secondly, the findings were generated within a study that was not primarily designed for systematic examination of MPT in WMR. Therefore, the focus group discussion guide did not contain fixed questions explicitly to explore this topic. Instead, MPT emerged rather inductively as a meaningful theme during our analysis. Thus, the results of the individual focus groups concerning teamwork are less comparable to each other than those regarding other subjects surveyed in a more standardized manner. Nonetheless, the significance of this issue is highlighted by the fact that the teams extensively discussed MPT without explicitly being asked about it.
As the teams’ perception of MPT is highly positive, we want to add, thirdly, that this perception is likely to be triggered by the experience of better rehabilitation outcomes. In general, it seems that the challenge of implementing a WMR programme and the corresponding changes to teamwork were perceived as a substantial improvement. Although we are aware of common problems and drawbacks of teamwork, the participants did not refer to these limitations. Perhaps these limitations get stronger consideration if intensified teamwork is already firmly established.
Fourthly, all findings were derived from self-reported data in a focus group setting. In future research, enriching the database with observational and process data could help to further examine different modes of teamwork and relevant contextual factors. Thereby it should be examined if, or to what extent, teams vary their teamwork along different needs of patients or rehabilitation phases. One-to-one interviews may help to avoid group-think. An enriched database would therefore help to check the validity and reliability of findings by triangulation of methods and data. Moreover, controlled studies are needed to evaluate effectiveness.
Fifthly, because coding was done by only one person, we were not able to check the quality of coding by calculating intercoder reliability. We tried to compensate for this limitation by continually discussing all findings within the research group and scientific advisory board.
Sixthly, even if we did achieve a certain degree of generalizability of results by generating types, the findings of the present study remain attached to the survey situation (7 WMR teams from selected German inpatient rehabilitation centres). Therefore, further research is needed to study the transferability of the results.
In conclusion, MPT plays an important role in the context of rehabilitation. This particularly applies to the rehabilitation of patients with severe and multifactorially conditioned limitations, as is the case in WMR. The present study supports the assumption that MPT is ideally realized in an interdisciplinary or even transdisciplinary manner and emphasizes the significance of promoting contextual factors. MPT should be given greater consideration in future research and clinical practice. Further studies are needed to examine the effectiveness of different team types and systematically assess relevant structural and organizational context-related factors. Team development programmes that integrate organizational development should be carried out in rehabilitation centres. The development and evaluation of MPT should be an integral part of quality management. This could be promoted by a stronger consideration of MPT in official manuals, requirements or standards, such as the WMR guideline. The findings of our feasibility study were incorporated into the third edition of the guideline, which was published in August 2012 (26). The relevance of MPT for successful implementation of WMR is now considered to a higher degree.
ACknowledgement
This research was funded by the German Pension Insurance. There was no further financial and material support for this research. The authors declare that they have no conflicts of interest.
REFERENCES

