Astri Ferdiana, MD, MPH1, Marcel W. M. Post, PhD2, 3, Sonja de Groot, PhD4, Ute Bültmann, PhD1 and Jac J. L. van der Klink, PhD1
From the 1Department of Health Sciences, Community and Occupational Medicine, University Medical Center Groningen, University of Groningen, Groningen, 2Brain Center Rudolf Magnus and Center of Excellence for Rehabilitation Medicine, University Medical Center Utrecht and De Hoogstraat, Utrecht, 3Department of Rehabilitation Medicine, University Medical Center Groningen, University of Groningen, Groningen and 4Amsterdam Rehabilitation Research Center Reade, Amsterdam, the Netherlands
OBJECTIVES: To examine the employment situation and predictors of return to work for individuals with spinal cord injury 5 years after discharge from inpatient rehabilitation.
DESIGN: Prospective cohort study.
SUBJECTS: A total of 114 subjects who were employed before the injury and who completed a 5-year follow-up.
METHODS: Work was defined as having paid work ≥ 1 h/week or ≥ 12 h/week. Predictors of return to work were identified using logistic regression analysis. Demographic, injury-related, pre-injury work factors and self-efficacy were measured at the start of rehabilitation and at discharge.
RESULTS: Return to work rates for ≥ 1 and ≥ 12 h/week were 50.9% and 42.6%, respectively. Median time to return to work was 13 months. Compared with before injury, participants worked for fewer hours per week and had occupations of lower physical intensity. The majority had a supplementary income. Those who returned to work were financially better-off than those who did not. Only 40% of participants received return to work support. A high/middle level occupation was associated with higher odds of return to work ≥ 1 h/week (odds ratio (OR) = 2.39, 95% confidence interval (95% CI) = 1.07–5.30). Low physical intensity of pre-injury occupation was significantly associated with higher odds of return to work ≥ 1 h/week (OR = 3.01, 95% CI = 1.31–6.91) and ≥ 12 h/week (OR = 2.67, 95% CI = 1.18–5.96). After adjustment for potential confounders, these associations were no longer significant.
CONCLUSION: Return to work after spinal cord injury was relatively high in this study, but entailed considerable changes in the employment situation, especially reduced working hours and less physically intense occupations. Rehabilitation interventions should enhance the skills and qualifications of individuals with physically-demanding pre-injury work in order to improve access to suitable jobs after spinal cord injury. Interventions should focus not only on return to work, but also on the quality of employment, including opportunities to pursue full-time work.
Key words: spinal cord injury; employment; return to work; disabled persons.
J Rehabil Med 2014; 46: 00–00
Correspondence address: Astri Ferdiana, Department of Health Sciences, Community and Occupational Medicine, University Medical Center Groningen, University of Groningen, Groningen, The Netherlands. E-mail: astriferdiana@gmail.com
Accepted May 13, 2014; Epub ahead of print Aug 28, 2014
Introduction
The advantages of employment for individuals with spinal cord injury (SCI) extend well beyond the economic aspects. Employment is associated with better functioning, social integration (1, 2), better quality of life and adjustment (2–4), psychological wellbeing (1) and lower mortality (5, 6). Nevertheless, there are significant barriers to gaining and maintaining employment (7, 8). Employment figures range from 21% to 67% (7) and a mean of only 35–40% of individuals with SCI are in paid employment (6). This situation has not changed significantly in the last 20 years (2).
Previous studies have focused extensively on demographic and injury characteristics associated with return to work (RTW) in SCI (2, 6–9), which are mostly non-modifiable and leave few opportunities to identify targets of vocational rehabilitation (VR) interventions. Only a few studies have demonstrated associations between psychological factors and employment status in SCI (9, 10), and even fewer have focused on perceived self-efficacy (11). Self-efficacy refers to a person’s confidence to perform specific behaviour required to produce a desired outcome (12). In relation to RTW, individuals with high self-efficacy have more confidence in their ability to make successful efforts to achieve RTW, so are more likely to make these efforts, and thereby show higher rates of RTW. Self-efficacy is associated with early work reintegration in workers across various health conditions (13). However, evidence about the association between self-efficacy and RTW in SCI is mixed (14).
In designing VR interventions, it is important to identify pre-injury vocational potential that can influence post-injury employment outcomes. However, there is little evidence for the role of pre-injury work characteristics (15, 16). Having a professional occupation prior to the injury is associated with a shorter time to obtaining a post-injury job (17). A Dutch study found that the level of physical demands of pre-injury occupations was related to post-injury employment status (18). However, this study was conducted more than 10 years ago, and since then there have been many changes in the social and healthcare systems and the workplace, e.g. advances in information technology (7), which may have improved the employment achievement. Moreover, little is known about whether individuals with SCI receive adequate RTW support and whether such support contributes to employment outcomes (19).
Previous studies on RTW among individuals with SCI have had a cross-sectional design and have involved individuals with heterogeneous injury duration (8). Existing longitudinal studies have a short follow-up time (20–22), during which vocational functioning could not be expected to be fully regained. In addition, RTW rates are mostly described without exploring the current work characteristics, such as occupational level, working hours, physical intensity or job satisfaction (8). Individuals with SCI who returned to work may experience work limitations due to their condition or may be unhappy with their work situation. Insight into these factors can help to address the specific needs of workers with SCI and to ensure sustainable work participation and work functioning.
The present study aims: (i) to determine the RTW rate 5 years after discharge from SCI rehabilitation; (ii) to describe the employment situation among those who returned to work; and (iii) to identify pre-injury work and psychological predictors of RTW independent of demographic, injury-related and functional independence factors.
Material and Methods
Sample
This study was conducted within the sampling frame of Dutch research project “Restoration of Mobility in the Rehabilitation of Persons with a Spinal Cord Injury”, a prospective cohort study involving 8 SCI rehabilitation centres in the Netherlands. The main aim in this cohort was to study wheelchair capacity and wheelchair mobility of individuals with SCI; thus, only wheelchair users were included. A detailed description of the design is given elsewhere (23). Inclusion criteria of the cohort study were: (i) having an acute SCI, (ii) age range at onset of injury 18–65 years, (iii) expected to remain wheelchair-dependent, (iv) no history of progressive diseases or psychiatric disorders, and (v) able to understand written and oral Dutch. For the present study, we included individuals who worked at the time of the injury.
Potential participants were invited for the study by their attending physician. The inclusion period was from August 2000 to July 2003. Ethical approval was obtained from the medical ethics committee of the iRv/SRL Hoensbroek for the initial cohort study, and of the University Medical Center Utrecht for the 5-year follow-up measurement. All participants provided written informed consent.
Procedure
Data collection was performed at the start of active rehabilitation (i.e. when the patient was able to sit for 3–4 h), at discharge from rehabilitation (approximately 9 months after admission) and at 5 years after discharge. These measurements included a physical examination by a rehabilitation physician, an oral interview with a trained research assistant and a self-report questionnaire. Trained research assistants were responsible for all measurements.
Variables
Demographic characteristic. Demographic data were collected at the start of active inpatient rehabilitation and included age, gender, and secondary education.
Injury characteristics. Injury characteristics were age at onset, cause of SCI (traumatic/non-traumatic), and injury severity (neurological level and completeness of injury, both assessed by the rehabilitation physician at discharge). Neurological level of injury was classified as paraplegia (lesion below T1) and tetraplegia (lesion at or above T1) using the American Spinal Injury Association (ASIA) classification (24). Completeness of injury was assessed using the ASIA Impairment Scale (AIS) and categorized as motor complete (AIS A and B) or motor incomplete (AIS C and D) (24).
Functional independence. Functional independence level was measured as part of the oral interview at discharge using the motor score of the Functional Independent Measure (FIM-motor score) (25), which has total score range of 13–91.
Pre-injury work characteristics. Pre-injury work characteristics were assessed using a questionnaire at the start of rehabilitation. Occupational level was classified into low, middle and high using the Dutch Standard Classification of Occupations (26) based on the educational/training qualification that is needed to perform the work tasks. Physical intensity of pre-injury occupation was classified into low and moderate/high using adapted definitions from Tomassen et al. (18). Occupations with low physical intensity mainly involved sedentary work, carrying only light weights and little movement. Moderate/high physical intensity involved moving, carrying weights/heavy objects and climbing stairs. Three researchers independently reviewed and classified the list of occupations based on these criteria. In case of a discrepancy, an occupational physician was consulted in order to reach consensus.
RTW support. RTW support was defined as any support received by participants aiming at RTW (yes/no) and assessed at 5-year follow-up. Participants were asked to identify the sources of RTW support (from the rehabilitation centre or other institutions) and whether the support was sufficient (yes/no). Participants were also asked whether they were undergoing education or retraining at the time of the study (yes/no).
Self-efficacy. Self-efficacy was measured at discharge using the Dutch version of the Sherer General Self-Efficacy Scale (27), which contains 16 items rated on a 5-point Likert scale (totally disagree to totally agree) and measures belief in one’s efficacy to cope with a broad range of challenging tasks. The total score range is 16–80, with higher scores indicating higher general self-efficacy.
Main outcome measure
Employment was assessed by 1 questionnaire item on the number of hours of paid work per week. Participants were classified as working if they had a paid work of ≥ 1 h/week, in line with the criterion in a previous study (28). The criterion of ≥ 12 h/week paid work was also used, in accordance with the Dutch Central Statistic Bureau’s definition of employment (29).
Employment situation at 5-year follow-up
The employment situation at 5-year follow-up was assessed by a questionnaire administered at the 5-year follow-up, which included the following questions: time needed to obtain work (in months), changes in work situation (ranging from fewer working hours to changes not related to SCI), satisfaction with work (satisfied/not satisfied), impact of SCI on work (yes, a lot/yes, a little bit, none), and sick leave during the past year (> 1 month/approximately 1 month/approximately 1 week/none. Those who did not work were asked about their reasons for not working. Sources of supplementary income were classified based on the Dutch social security system: (i) permanent disability benefit, for those with 80% incapacity to work; (ii) partial or temporary disability benefit for those with 35%–79% incapacity to work; (iii) old age pension/early retirement benefit; and (iv) life annuity. The amount of monthly income, both individual and with-partner, was categorized into < 1000 and ≥ 1000 Euros/month. The number of working hours was categorized into: (i) ≤ 12; (ii) 13–23; (iii) 24–34; and (iv) ≥ 35 h/week.
Analysis
The results are presented as absolute numbers and percentages for categorical variables, mean (standard deviation; SD) for normally-distributed continuous variables and median (range) for continuous variables with a skewed distribution. Student t-tests and χ2 tests were used as preliminary analysis to test significant differences between the RTW and non-RTW groups.
Logistic regression was used to examine the influence of a range of variables with different nature (continuous, categorical, etc.) on a dichotomous outcome (30). Bivariate logistic regression analyses were conducted to examine the relationship between employment status of ≥ 1 h/week and each predictor, which included: occupational level (middle/high = 1, basic/low = 0), physical intensity of pre-injury occupation (low = 1, moderate/high = 0), RTW support (yes = 1, no = 0) and self-efficacy. Age at onset (in years), gender (male = 1, female = 0), secondary education (yes = 1, no = 0), injury level (paraplegia = 1, tetraplegia = 0), injury completeness (incomplete = 1, complete = 0), and FIM motor-score were included as potential confounders based on previous literature. Multivariable logistic regressions were performed to identify the associations between the predictor and the outcome independent of all confounders. The models were fitted on the basis of multiple imputed data sets. Missing values ranged from 4.4% (RTW support) to 16.7% (self-efficacy). The highest percentage of missing values was nearly 20%; therefore, we generated 20 sets of multiple imputed data, in which the variables with missing values were predicted by all other variables. All analyses were repeated for employment status ≥ 12 h/week. Analysis was performed using SPSS version 20.0.
Results
Sample
The initial study sample included 225 participants, of whom 177 were in paid work pre-SCI. Fifty-seven participants were lost to follow-up and 6 were over the legal retirement age. A final total of 114 participants were included in our analysis. The study flow diagram is illustrated in Fig. 1. A non-responder analysis was conducted by comparing the demographic and injury-related characteristics of the 114 participants with the 57 individuals who were lost to follow-up. Those who were lost to follow-up were significantly older than the participants. There were no differences in injury characteristics between the 2 groups.
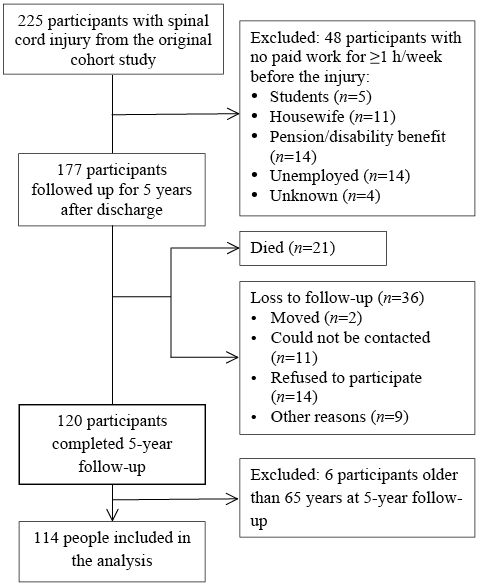
Fig. 1. Participants from initial sample to analytic sample.
Table I summarizes the characteristics of participants and the comparisons between those who returned to work and those who did not. Mean age at follow-up was 42.1 (11.6) years. Mean time after injury was 6.6 (0.8) years.
|
Table I. Baseline characteristics of participants |
||||
|
Variables |
Total (n = 114) |
RTW at 5-year follow-up (n = 58) |
No RTW at 5-year follow-up n = 56 |
p-value |
|
Males, n (%) |
87 (76.3) |
46 (79.3) |
41 (73.2) |
0.444 |
|
Secondary education, n (%) |
69 (60.5) |
41 (70.7) |
28 (50.0) |
0.024 |
|
Traumatic cause, n (%) |
98 (86.0) |
51 (87.9) |
47 (83.9) |
0.539 |
|
Paraplegia, n (%) |
67 (58.8) |
38 (65.5) |
29 (51.8) |
0.136 |
|
Motor incomplete, n (%) |
57 (50.0) |
29 (50.0) |
28 (50.0) |
0.574 |
|
Pre-injury occupational level, n (%) Basic/low Middle/high |
42 (39.3) 65 (60.7) |
16 (29.1) 39 (70.9) |
26 (50.0) 26 (50.0) |
0.027 |
|
Physical intensity of pre-injury occupation, n (%) Low Moderate/high |
36 (33.6) 71 (66.4) |
25 (45.5) 30 (54.5) |
11 (21.2) 41 (78.8) |
0.008 |
|
RTW support, n (%) |
48 (44.0) |
21 (40.4) |
27 (47.4) |
0.463 |
|
Education/training at 5-year follow-up, n (%) |
14 (13.1) |
8 (15.7) |
6 (10.7) |
|
|
Age at onset, years, mean (SD) |
35.5 (11.6) |
34.7 (10.8) |
36.3 (12.5) |
0.496 |
|
FIM motor-score at discharge (13–91), mean (SD) |
67.5 (22.3) |
74.1 (18.4) |
60.4 (23.8) |
0.001 |
|
Self-efficacy at discharge (16–80), mean (SD) |
53.4 (24.5) |
50.2 (21.1) |
56.4 (27.0) |
0.224 |
|
FIM: Functional Independence Measure; RTW: return to work. |
||||
RTW at 5-year follow-up
At 5-year follow-up, 58 out of 114 participants who worked before the injury (50.9%) had returned to work for ≥ 1 h/week. Using the criterion of ≥ 12 h/week, 108 out of 114 participants (94.7%) worked before the injury and 46 (42.6%) had returned to work at 5-year follow-up. Compared with participants who did not return to work, those who returned to work for ≥ 1 h/week were more likely to have a secondary education, a middle/high occupational level, less physically demanding work and a higher FIM motor-score at discharge (Table I).
A total of 23 participants (47.9%) were able to return to work for ≥ 1 h/week within the first year after discharge. Eleven participants (22.9%) returned to work within 2 years after discharge, and 14 participants (29.2%) needed more than 2 years to return to work. The median time to return to work after discharge from rehabilitation was 13 months (range 0–72 months).
Of the 56 participants who did not return to work for ≥ 1 h/week, 20 were not employed due to SCI-related reasons, 8 were homemakers, 6 were students, 2 had early retirement, 3 were unemployed for other reasons and 17 did not give a reason.
Employment situation at 5-year follow-up
Table II shows the changes in employment situation at 5-year follow-up compared with before the injury among the 58 participants who returned to work for ≥ 1 h/week. The mean working hours per week decreased significantly, from 44.1 (SD 15.8) to 22.6 (SD 12.2) h/week. The proportion of participants working for ≥ 35 h/week decreased from 81% before SCI to 22.4% after SCI. The proportion of participants in middle/high occupational level occupations was 13.6% higher after SCI. Professions in this category included administrator, information technology analyst, engineer, manager and web designer. The proportion of participants with moderate/high physical intensity occupations was 27.8% lower. This category included professions such as logistic workers and expedition employees.
The majority of participants were satisfied with their work (Table II). Dissatisfied participants attributed their work dissatisfaction to having an SCI. A few participants felt that the SCI hampered much of their work activities.
|
Table II. Work situation before injury and 5 years after discharge from rehabilitation in participants who returned to work for ≥ 1 year at 5-year follow-up (n = 58) |
||
|
Variables |
Before injury |
5-year follow-up |
|
Working hours, mean (SD) |
44.1 (15.8) |
22.6 (12.2) |
|
Working hours, n (%) ≤ 12 hours 13–23 hours 24–34 hours ≥ 35 hours |
2 (3.4) 5 (8.6) 4 (6.9) 47 (81.0) |
13 (22.4) 15 (25.9) 17 (29.3) 13 (22.4) |
|
Occupational level, n (%) Basic/low Middle/high |
16 (29.1) 39 (70.9) |
7 (15.6) 39 (84.4) |
|
Physical intensity of occupation, n (%) Low Moderate/high |
25 (45.5) 30 (54.5) |
33 (73.3) 12 (26.7) |
|
Work satisfaction, n (%) Satisfied Not satisfied |
42 (85.7) 7 (14.3) |
|
|
Work activities were hampered by SCI, n (%) Yes, a lot Yes, a little bit No |
7 (13.2) 30 (56.6) 16 (30.2) |
|
|
Sick leave in the past year because of SCI, n (%) |
||
|
More than 1 month Approximately 1 month Approximately 1 week None Changes in work situation, n (%) Less working hours Change to other function, lower level Transferred to other function, same level Changes not related to SCI |
7 (12.1) 3 (5.2) 22 (37.9) 26 (44.8) 25 (43.1) 7 (12.3) 1 (1.8) 8 (13.8) |
|
|
SCI: spinal cord injury. |
||
Out of all participants, 93 (86.9%) did not follow any training or education for RTW at 5-year follow-up. Forty-eight out of all participants (44%) received RTW support at any time after discharge from inpatient rehabilitation, 27 of whom were able to return to work at 5-year follow-up. There was no significant relationship between RTW status and receiving RTW support. Fourteen participants received RTW support from the rehabilitation centre, 16 from a specialized organization and 8 from both. Out of the 14 participants who received RTW support from the rehabilitation centre, 13 reported that this support had not been sufficient. Of 16 participants who received RTW support from specialized organizations, 10 reported that it had not been sufficient.
At 5-year follow-up, 79 (81.4%) of participants received a supplementary income (Table III): 41 (51.9%) a permanent disability benefit, 21 (26.6%) a temporary disability benefit, 2 (2.5%) an old age/early retirement pension, 2 (2.5%) a life annuity, and 13 (16.5%) an income from other sources. The majority (72.2%) had a monthly income of > 1,000 Euros/month. The proportion of participants who had an income < 1,000 Euro per month (both individual income and income with partner) was higher in the group of participants who did not return to work. The number of supplementary income recipients was higher in participants who did not return to work, but also in the group who returned to work, almost 70% received supplementary income.
|
Table III. Income and supplementary income at 5-year follow-up (n = 114) |
||||
|
Total n (%) |
RTW at 5-year (n = 58) n (%) |
No RTW at 5-year (n = 56) n (%) |
p-value |
|
|
Income < 1,000 Euros |
30 (27.8) |
8 (14.5) |
22 (41.5) |
0.002 |
|
Income with partner < 1,000 Euros |
20 (22.0) |
6 (12.5) |
14 (32.6) |
0.021 |
|
Received supplementary income |
79 (81.4) |
35 (68.6) |
44 (95.7) |
0.001 |
|
RTW: return to work; SCI: spinal cord injury. |
||||
Predictors of RTW at 5-year follow-up
Table IV shows the bivariate associations between predictor variables with RTW ≥ 1 h/week and ≥ 12 h/week at 5-year follow-up. Participants who had a middle/high level pre-injury occupation had 2.39 times higher odds (95% CI 1.07–5.30) of returning to work ≥ 1 h/week at 5-year follow-up compared with those with low level pre-injury occupation. Odds of returning to work ≥ 1 h/week at 5-year follow-up was 3.01 times higher (95% 1.31–6.91) in participants whose pre-injury occupation involved low physical intensity compared with those whose pre-injury occupation involved moderate/high physical intensity. Physical intensity of pre-injury occupations was significantly associated with RTW ≥ 12 h/week (OR = 2.67, 95% CI = 1.18–5.96) RTW support and self-efficacy did not show significant associations with both RTW ≥ 1 h/week and RTW ≥ 12 h/week at 5-year follow-up.
|
Table IV. Bivariate logistic regression between predictor variables and return to work ≥ 1 h/week and ≥ 12 h/week at 5-year follow-up |
||
|
Variables |
RTW ≥ 1 h/week OR (95% CI) |
RTW ≥ 12 h/week OR (95% CI) |
|
Occupational level Low Middle/high |
1 2.39 (1.07–5.30) |
1 2.13 (0.94–4.81) |
|
Physical intensity of pre-injury work Moderate/high Low |
1 3.01 (1.31–6.91) |
1 2.67 (1.18–5.96) |
|
RTW support No Yes |
1 1.36 (0.64 –2.89) |
1 1.55 (0.73–3.33) |
|
Self-efficacy |
0.99 (0.97–1.01) |
0.99 (0.97–1.01) |
|
CI: confidence interval; OR: odds ratio; RTW: return to work. |
||
When adjusted for potential confounders, none of the predictors was significantly associated with RTW ≥ 1 h/week and RTW ≥ 12 h/week (see Table V).
|
Table V. Multivariable logistic regression between predictor variables and return to work ≥ 1 and ≥ 12 h/week at 5-year follow-up |
||
|
Variables |
RTW ≥ 1 h/week OR (95% CI) |
RTW ≥ 12 h/week OR (95% CI) |
|
Age at onset, years |
0.98 (0.94–1.02) |
0.96 (0.93–1.00) |
|
Gender Female Male |
1 1.51 (0.53–4.28) |
1 1.87 (0.65–5.41) |
|
Secondary education No Yes |
1 1.88 (0.71–5.03) |
1 2.15 (0.79–5.80) |
|
Neurological level of injury Tetraplegia Paraplegia |
1 0.57 (0.16–2.01) |
1 0.73 (0.21–2.54) |
|
Completeness of injury Complete Incomplete |
1 0.84 (0.32–2.21) |
1 1.13 (0.43–2.97) |
|
FIM at discharge |
1.04 (1.01–1.07) |
1.03 (0.99–1.05) |
|
Occupational level Low Middle/high |
1 1.61 (0.56–4.65) |
1 1.44 (0.48–4.29) |
|
Physical intensity of pre-injury work |
||
|
Moderate/high Low |
1 2.33 (0.80–6.78) |
1 2.25 (0.78–6.41) |
|
RTW support No Yes |
1 1.71 (0.67–4.33) |
1 1.77 (0.71–4.44) |
|
Self-efficacy |
0.99 (0.97–1.01) |
0.99 (0.98–1.02) |
|
CI: confidence interval; FIM: Functional Independence Measure; OR: odds ratio; RTW: return to work. |
||
Discussion
Five years after discharge from inpatient rehabilitation, 50.9% of participants had returned to work for ≥ 1 h/week and 42.6% had returned to work for ≥ 12 h/week. Compared with a previous study in the same cohort (28), a higher RTW rate was found because more information regarding employment status could be obtained after completion of the previous study.
The RTW rate in this study was higher than that found in an earlier Dutch study (37%) (18), which used a cross-sectional design and included participants with a shorter post-injury duration. Another Dutch study found that 60% of individuals with SCI worked for at least 4 h/week (31); however, this study involved a small number of participants with a longer post-injury duration. Post-injury employment rates typically improve 5–10 years after injury (2). Over time, individuals with SCI may have become better adjusted to their functional limitations and enhanced their skills in using the remaining physical capacity, acquired new skills or qualifications suitable for a new job, or overcome barriers to work.
It is difficult to compare the RTW rate in our study with the rates reported in the international literature because of the variability in the definition of employment. In addition, our study was limited to individuals with SCI who were wheelchair-dependent. As previous studies often did not provide explicit information about wheelchair dependency, direct comparisons are hindered. Studies with a similar post-injury duration of 5–6 years found lower employment rates, i.e. 12.4% in Spain (6), and 29.5% in Italy (32), and 24.3% in the USA (33). This discrepancy may be attributed to a range of structural factors, such as uptake and effectiveness of vocational rehabilitation services, job availability and the existing social security and welfare system (3, 8). Dutch employers are obliged to support RTW in employees with sickness absence. The Dutch social security system also promotes work participation by allocating additional benefits for workers with disability who work for more than 50% of work capacity. Studies from other countries suggested that disability benefits are employment disincentives, being one of the important barriers to RTW (34).
The first year after discharge seemed to be the critical time for RTW, as almost half of participants returned to work within this time. Krause et al. (17) found that the mean time to the first a post-injury job was 4.8 years, but this time was much shorter for individuals who returned to the same job and who had a professional occupation (e.g. managers).
Concurrent with previous studies (15, 31), we found that participants who returned to work experienced considerable changes in their work, including reduced working hours. Working fewer hours may allow more time for individuals with SCI for personal care and also for travel to and from work, or may be caused by secondary complications (35). Although a non-monetary benefit of employment, such as psychological well-being, did not differ between part- and full-time employment (1), a part-time job is usually associated with lower income, less benefit and less possibility of having career advancement and job tenure (1,2), which may affect job retention (36). Further research is needed to investigate the reasons and advantages of part-time work for individuals with SCI.
We found that work satisfaction among those who returned to work was high. Moreover, SCI seemed to exert little interference with work, which is plausible because persons who experience high work interference due to their SCI are not likely to continue performing that work. We found that those who did not return to work were more economically disadvantaged, as more of them lived on income of less than 1,000 Euros/month and were dependent on supplementary income. Nevertheless, most of those who returned to work received supplementary income. Individuals in the Netherlands who experience substantially decreased income due to disability, e.g. working fewer hours or at a lower level, are eligible for benefits. To ascertain the actual financial benefits of RTW, further research is needed to calculate the income fraction of RTW from the total income after the injury.
An increased proportion of participants was engaged in middle/high level occupations and less physical demands after the injury, which confirms previous findings (16, 18, 28, 31). Significant physical limitations due to SCI prevent individuals from performing physically intense occupations and often require them to change to administrative and clerical types of work (15, 18, 37). These types of occupation are often associated with middle/high occupational level and require higher qualifications, such as college and university level qualifications (37) and further education and training. At the time of the study, however, very few of the participants in the current study were undergoing further education or training that might have increased their qualifications and opportunity for RTW.
Unlike other studies, which found that provision of RTW support and counselling positively influenced post-injury vocational outcomes (18, 19), we did not find such a relationship. However, the level of RTW support in our study was low, as only 40% of the participants received RTW support from the rehabilitation centres or other institutions. Lack of information about available vocational support may be one of the explanatory factors for this substantial unmet need for RTW support (2, 8). Alternatively, the long response-period of 5 years may have resulted in under-reporting of RTW support.
Perceived self-efficacy at discharge was not related to RTW in our study. Previous studies have shown that self-efficacy plays an important role in participation after SCI (14, 38); however, the association between self-efficacy and employment status has been inconsistent (14, 21). Future studies should consider measuring RTW self-efficacy, which has been shown to predict higher and faster work reintegration in workers with musculoskeletal disorders (13).
Finally, we found that FIM motor-score at discharge was the only significant variable for employment status in the multivariable model. This emphasizes the role of physical rehabilitation in improving functional independence level (16). However, to achieve RTW at a level of 12 h/week, FIM motor-score was less important, indicating that there are factors other than independence level that influence RTW at this level.
Study strengths and limitations
The strength of the current study was the detailed description of the nature of employment before and after the injury and a sufficient length of follow-up of 5 years. The duration of SCI was relatively homogeneous, which may reduce bias in determining the rate of RTW. Unlike previous studies, which have focused on traumatic SCI (6), we also included non-traumatic SCI.
The generalization of our findings may be limited to individuals with SCI who survive the first 5 years after injury and are wheelchair-dependent. The RTW rate may be an underestimation of the actual RTW rate among individuals with SCI, since autonomy in ambulation is associated with RTW (39). However, the demographic and clinical characteristics of our cohort are comparable to data from other studies (23). We did not have information about whether the participants returned to their pre-injury occupation, and this may have influenced the likelihood and time to RTW. Information on job retention during the 5-year period was not available, and this is important because individuals with SCI often have secondary complications that need hospitalization and prevent them from maintaining work (40). Lastly, our analyses did not take into account other factors important to RTW, such as assistive technology (7, 28, 39) and environmental variables (2, 7, 21).
Implication
Our findings demonstrated that individuals with SCI whose pre-injury work involved moderate or high physical intensity should be provided with more support during or after inpatient rehabilitation. For example, further education and vocational retraining may enhance skills and qualifications to access more suitable occupations, particularly occupations with lower physical demands. Workplace modifications may be needed to broaden the range of jobs available for individuals with SCI regardless of their physical limitation. Future research and VR interventions should focus not only on returning individuals with SCI into the labour market, but also on the quality of employment, including opportunity to pursue full-time work and obtain greater benefits from work.
Conclusion
Five years after discharge, 50.9% of our participants who worked before SCI had returned to work. Post-injury occupations typically involved reduced working hours, lower physical intensity and a middle/high occupational level. Individuals who returned to work were financially better-off than those who did not, yet the majority was still dependent on supplementary income. RTW was associated with physical intensity and occupational level of pre-injury work.
These results emphasize the importance of rehabilitation in enhancing the skills and qualifications of individuals in order to increase access to suitable jobs post-injury and improve ability to secure sustained and rewarding employment.
References

