Flavie Frémondière, MD1, Virginie Saoût, MD2, Franck Lacœuille, PhD3, Anne-Laure Ferrapie, MD2, Philippe Menei, MD, PhD4, Olivier Couturier, MD, PhD3, Isabelle Richard, MD, PhD1 and Mickaël Dinomais, MD, PhD1
From the Departments of 1Physical Medicine and Rehabilitation, 3Nuclear Medicine and 4Neurosurgery, LUNAM, Université d’Angers, CHU Angers and 2Deprartment of Physical Medicine and Rehabilitation, Educational Centre Les Capucins, Angers, France
BACKGROUND: Intrathecal baclofen infusion is an established method for the treatment of generalized and disabling spasticity. The most frequent technical problems are due to catheter /pump disconnections, but diagnosis of dysfunction may be difficult.
CASE REPORT: We report here the case of a 53-year-old woman with spastic paraplegia treated with intrathecal baclofen. Spasticity remained uncontrolled despite a gradual increase in baclofen dosage. On plain radiographs the distal end of the catheter was found to be pointing downwards with the catheter tip at level L5 and no apparent disconnection or failure. Indium111 diethylenetriamine penta-acetic acid (DTPA) scintigraphy combined with computed tomography revealed that the activity of the radioisotope was highest next to the first sacral vertebra and that there was no leakage. Radioisotope activity above the lumbar level was very low. The catheter tip was therefore repositioned to level T7. One month later, spasticity was well controlled and a second scintigraphy confirmed high activity of intrathecal radioisotope up to the basal cisterns.
Discussion: The combination of Indium111 DTPA scintigraphy with computed tomography allows anatomical and functional investigation of intrathecal drug administration. In this case report this approach showed that the inefficiency of intrathecal baclofen was due to the caudal orientation of the catheter.
Key words: spasticity; multiple sclerosis; intrathecal baclofen pump; scintigraphy; complications; cerebrospinal fluid flow dynamics.
J Rehabil Med 2014; 46: 00–00
Correspondence address: Flavie Frémondière, Centre de rééducation Les Capucins, 49000 Angers Cedex, France. E-mail: flaviefremondiere@yahoo.fr
Accepted Feb 4, 2014; Epub ahead of print Apr 8, 2014
Introduction
The use of an intrathecal baclofen (ITB) pump has proved efficient for the treatment of generalized and disabling spasticity (1, 2). However, the rate of complications or incidents related to this technique can be as high as 40% (3, 4). In cases of suspected malfunction (5, 6) a number of investigations allow evaluation of the catheter-pump system. When plain radiographs of the device and contrast injection by the accessory pump port are inconclusive, scintigraphy after Indium111 diethylenetriamine penta-acetic acid (DTPA) injection in the pump reservoir is a valuable method to investigate catheter dysfunction (7–9). Slow infusion of the tracer allows improved detection of small cracks in the catheter compared with contrast injection by the accessory pump port (5). We report here a case of a woman receiving ITB, in whom Indium111 DTPA scintigraphy associated with computed tomography documented the relationship between clinical effect, diffusion of the tracer and placement of the catheter tip.
Case Report
A 53-year-old woman presented with T10 spastic paraplegia (Modified Ashworth Scale 4/5 in the lower limbs) due to secondary progressive multiple sclerosis. Magnetic resonance imaging (MRI) revealed a cervical spinal cord lesion. An ITB trial, with injection of 100 µg baclofen by lumbar puncture, was performed, and this reduced the Modified Ashworth Scale to 2/5. The patient was referred for ITB treatment, and an ITB pump was implanted in December 2010 (initial dosage 200 µg per day). The neurosurgeon could not place the distal end of the catheter at the lower thoracic level as planned, and the catheter was located at L5. MRI did not reveal any malformation or anatomical cause for this difficulty. The treatment was inefficient despite an increase in the dosage to 550 µg per day. Contrast injection through the accessory pump port revealed catheter obstruction and surgical revision was performed. Clinical improvement was achieved, but lasted for only 4 months despite the increase in the dosage to 850 μg baclofen per day. The patient developed pulmonary and urinary infections, which were treated, but this did not improve her spasticity. The neurological status of the patient remained stable, and cerebral and spinal cord MRI did not show additional lesions. Plain radiographs of the device did not show any kinking or breaking of the catheter or disconnection between the pump and the catheter. The distal end of the catheter was located at vertebral level L5. Direct injection of 150 μg baclofen by lumbar puncture was effective and excluded tolerance to baclofen (1, 10). The question remained whether the non-optimal location of the catheter tip was responsible for the clinical inefficiency and whether it justified surgical replacement.
Isotopic cisternography (injection of 35 MBq Indium111 DTPA in 0.5 ml saline into the pump reservoir) was performed, with acquisitions 30 min, 4, 24, 48 and 72 h after the injection, with anterior and posterior projections focused on the abdomen, chest, head and neck. This examination was combined with computed tomography 48 and 72 h after the injection (Fig. 1). There was no evidence of extravasation or leakage along the catheter. Radioactivity was found in the subarachnoid space with a maximum of activity at 48 and 72 h next to the first sacral vertebra, corresponding to the orifice of the catheter. Activity in the upper part of the spinal canal and at the brain level remained very low at all times (Fig. 2). This examination demonstrated the poor diffusion of baclofen, probably due to the caudal orientation of the catheter. The distal end of the intrathecal catheter was successfully repositioned to vertebral level T7. A month later, the efficiency was clinically obvious with a dosage of 650 μg per day. Modified Ashworth Scale in the lower limbs was 1/5. The patient was very satisfied. Six months after the repositioning of the catheter, the efficiency remained. At 24 h acquisition, second isotope cisternography showed an excellent distribution of tracer in the subarachnoid space and a high level of activity up to the basal cisterns (Fig. 2).
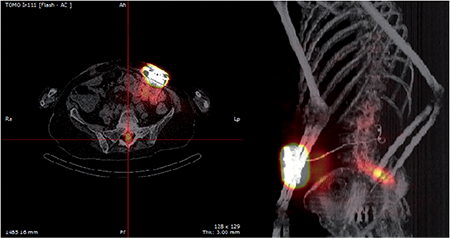
Fig. 1. Indium111 diethylenetriamine penta-acetic acid (DTPA) scintigraphy combined with computed tomography 72 h after isotope injection, showing activity in the subarachnoid space, next to the first sacral vertebra without leakage along the catheter.

Fig. 2. Isotope cisternography showing diffusion of the tracer to the basal cisterns before (left) and after (right) repositioning of the catheter.
Discussion
The initial scintigraphy showed that the radioisotope stagnated at level L5–S1 and did not diffuse upwards, which explained the absence of a clinical effect of ITB. The second scintigraphy, after repositioning the catheter, showed a clear increase in diffusion of the radioisotope along the spinal canal to the basal cisterns, together with satisfactory control of spasticity. To our knowledge this is the first documentation of the association of inefficient ITB administration with abnormal distribution of the drug along the subarachnoid space. For this patient, the distal tip of the catheter was initially located next to vertebra L5. The absence of spinal gamma-aminobutyric acid receptors at this level could explain the inefficiency of baclofen. This case report illustrates the importance of the placement of the distal end of the intrathecal catheter, ideally at a low thoracic or high lumbar level, in treatment of lower limb spasticity.
In this case report, abnormalities of cerebrospinal fluid (CSF) flow dynamics could also contribute to the absence of any therapeutic effect. In a recent review, Beggs (11) reported the mechanisms of CSF flow abnormalities in multiple sclerosis. Multiple sclerosis has been associated with extracranial venous abnormalities known as chronic cerebrospinal venous insufficiency (CCSVI). CCSVI is characterized by multiple extracranial stenoses of the venous-drainage pathways, responsible for venous hypertension in the dural sinuses. These vascular changes result in hydraulic resistance of the cerebral venous drainage system and modifications in flow dynamics of the CSF. Thus, in this patient with multiple sclerosis, misplacement of the catheter together with the resistance of CSF drainage could explain the inefficiency of baclofen. This also could explain why the caudal orientation of the distal end of the catheter leads to inefficiency in some patients, as in this case, and not in others.
The use of Indium111 DTPA cisternography in the evaluation of clinical inefficiency of ITB devices (7–9) has been reported. Here we associated isotopic cisternography with computed tomography. This allowed us: (i) to check the absence of extravasation or leakage of the isotope along the catheter; (ii) to check the location of the distal end of the catheter in the subarachnoid space by overlaying scintigraphic images over computed tomography images; (iii) to confirm that the pump was functioning; (iv) to analyse the diffusion of the tracer, and its distribution in the subarachnoid space. The combination of scintigraphy and computed tomography allows both functional and anatomical analysis of the entire device.
In conclusion, in this case poor clinical efficiency was related to abnormal diffusion of ITB in the subarachnoid space, with stagnation in the dural sac. This abnormal diffusion was probably caused by the location of the tip of the catheter. Indium111 DTPA scintigraphy combined with computed tomography allowed complete analysis of both anatomical and functional aspects. This strategy should be considered in the exploration of dysfunctional intrathecal devices.
The authors declare no conflicts of interest.
References

