Akke Bakker, MSc1–3, Taco J. Blokhuis, PhD1, Michelle D. M. E. Meeks, MSc1–3, Hermie J. Hermens, PhD3,4 and Herman R. Holtslag, PhD2
From the 1Department of Surgery and 2Sports and Rehabilitation Medicine, University Medical Centre Utrecht, Utrecht, 3MIRA Institute, University Twente and 4Roessingh Research and Development, Roessingh Institute, Enschede, The Netherlands
OBJECTIVE: Hip fractures have a high morbidity and mortality in elderly patients. Improving mobility outcomes is crucial in order to decrease the burden of this injury. The objective of this study was to investigate dynamic weight loading in older people with hip fractures using a new device.
DESIGN: In an observational study, low-energy hip fracture patients were monitored one day per week with the FeetB@ck system during their admission. Pain, gait and balance scores were noted. Outcome measures of the FeetB@ck system are steps, walking bouts and loading rate.
RESULTS: A total of 21 patients with hip fracture were included in the study (mean age 80.3 years (standard deviation 8.3 years)). The number of steps, walking bouts and loading rate had a positive linear relationship with rehabilitation (i.e. gait and balance scores) (p < 0.05). These parameters also differed significantly between patients with short (less than 8 weeks, n = 7), intermediate (between 8 and 12 weeks, n = 8) and long (longer than 12 weeks, n = 6) of rehabilitation (p < 0.01).
CONCLUSION: The loading rate is a sensitive weight loading parameter for analysis of dynamic weight loading during rehabilitation in elderly hip fracture patients. This parameter correlates with clinical improvement and can differentiate between fast and slow rehabilitation.
Key words: ambulatory monitoring; hip fractures; rehabilitation; weight-bearing.
J Rehabil Med 2014; 46: 00–00
Correspondence address: Taco J. Blokhuis, Department of Surgery, PO Box 85500, University Medical Centre Utrecht, NL-3508 GA Utrecht, The Netherlands. E-mail: T.J.Blokhuis@umcutrecht.nl
Accepted Dec 16, 2013; Epub ahead of print Mar 28, 2014
Introduction
Hip fractures are among the most common injuries in the elderly population. Patients with a hip fracture have a high morbidity and mortality (1–3) due to the impact of the injury and because of their health status. The costs associated with geriatric hip fractures are very high. Several studies in USA and UK have calculated the annual costs at between 12,562 and 26,545 USD per patient (4–6), and these costs increase substantially when patients are not able to return to their pre-injury place of residence (7). Given the increasing number of elderly people worldwide, the number of hip fractures and their economic consequences are projected to rise substantially (8). Many patients with hip fracture become more dependent and move into residential care, increasing the already significant burden on society. Improving mobility outcomes is key to relieving the burden on individuals, their care providers, and society (9).
The timing and extent of weight bearing depends on the type of fracture, the method of fracture fixation and the patients’ physical and mental state. Therefore there is no general standard for mobilization of patients after a hip fracture. Early mobilization and weight bearing is beneficiary as it stimulates fracture healing (10, 11). Moreover, patients rehabilitating after a fracture may benefit from early weight bearing by maintaining muscle mass, bone mass and avoiding complications due to long immobility (12, 13). On the other hand, fracture-related circumstances could make full weight bearing undesirable, for example a comminuted fracture in patients with poor bone quality. Currently, the amount of weight bearing is prescribed by the surgeon and monitored by the patient and the physical therapist. This monitoring is unreliable (14), which hampers both patient recovery and patient safety.
Currently, data on mobilization after surgical treatment of hip fractures in the elderly are limited due to the quality of the measuring devices. Several studies show improved mortality and functional outcomes of elderly patients with hip fractures by postoperative orthogeriatric collaboration, in which geriatricians participate in the postoperative care and the postoperative regimen is intensified (12). In addition, stimulation of mobility by individualized physiotherapy based on weight bearing on the affected extremity leads to a better outcome (13), suggesting that early weight bearing is beneficiary for these patients. However, because of a lack of objective and quantifiable data on weight bearing, quantification of the rehabilitation process is difficult. For this reason, rehabilitation remains a black box, and it is difficult to achieve improvements.
Axial loading is an important measure of weight bearing. With axial loading the skeleton is stimulated, leading to improved bone quality, muscle mass and coordination. However, axial loading measurement devices are not yet available for widespread use. In addition, direct or constant monitoring with such devices is not yet possible. This study aims to investigate dynamic weight loading in older people with hip fractures using a new measurement device. This device, Feetb@ck (Evalan, Amsterdam, The Netherlands), consists of a sensor placed in a sandal, which continuously registers pressure. The data are sent to a mobile interface, through which data can be seen and analysed. The objectives were to measure steps, walking bouts and loading rate after a hip fracture, and to determine the parameters from these data that show a good correlation with the clinical outcome (mobility scores) and the length of stay in the nursing home after a hip fracture.
Methods
Patients were recruited from the rehabilitation wards of 5 nursing homes (Careyn Maria-Oord, Careyn Snavelenburg, Geinsche Hof, Warande Bovenwegen and Warande Rehabilitation) in the Utrecht area, the Netherlands. Inclusion criteria were: age over 60 years and a low-energy hip fracture. Exclusion criteria were: pathological fractures, co-morbidity that influenced mobility, total hip prostheses, cognitive problems, and lack of informed consent. For a period of one day per week weight bearing was monitored using an ambulant in-sole device, the FeetB@ck system, and the University Medical Centre Utrecht, the Netherlands. It consists of an in-sole pressure sensor, an electronic amplifier and a data collector. It can monitor axial forces for 1 day and sends the results to a server in packages of 10 min. The system measures axial forces with an accuracy of 15%. The system reports the number of steps, the number of periods of walking intermittent with rest (walking bouts), ambulation time, stride time, heel stance time, peak vertical ground reaction force (vGRF), impulse and loading rate, which is the steepness of the loading curve per step. A graphic representation of these parameters is shown in Fig. 1.
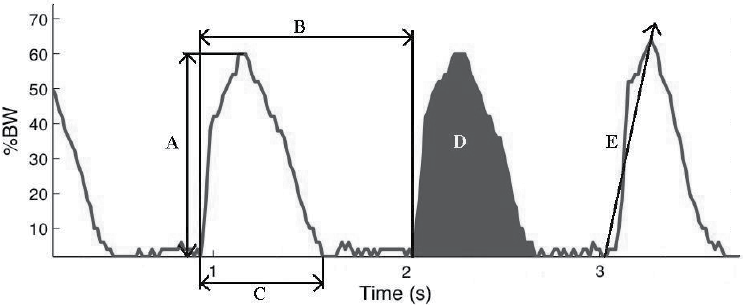
All patients were monitored from 09.30 h to 16.30 h with the FeetB@ck device, under supervision of one investigator (AB). The device was calibrated for each patient. Data generated by the Feetb@ck system, as shown in Fig. 1, were compared with clinical outcome measures for gait, balance and pain. Balance and gait scores were determined with the Tinetti Performance-Oriented Mobility Assessment (POMA) consisting of gait and balance tasks (15). The amount of pain was determined with a visual analogue scale (VAS). Measurements were repeated weekly during the admission in the nursing home. The POMA was obtained by the treating physical therapist and all other measurements were performed by one investigator (AB). In order to link the parameters generated by the Feetb@ck system to the progress of clinical healing, separate groups of short rehabilitation (less than 8 weeks admission to the nursing home), intermediate rehabilitation (between 8 and 12 weeks admission), and long rehabilitation (more than 12 weeks admission) were analysed and data were compared between groups. These groups were grouped retrospectively based on the distribution of duration of admission to the nursing homes of the included group of hip fracture patients. The research protocol was approved by the medical ethics review board of the University Medical Centre Utrecht.
Statistical analysis
For each weight bearing parameter in each subject a linear equation was fitted to the data. Differences in weight bearing parameters in week 1–8 post surgery between short, intermediate and long rehabilitation groups were assessed with one-way unbalanced analysis of variance (ANOVA). Pain and POMA scores were correlated with weight loading parameters. For analysis, the software programs Statistical Package for the Social Sciences (SPSS) 20.0.0 and Matlab R2011b were used.
Results
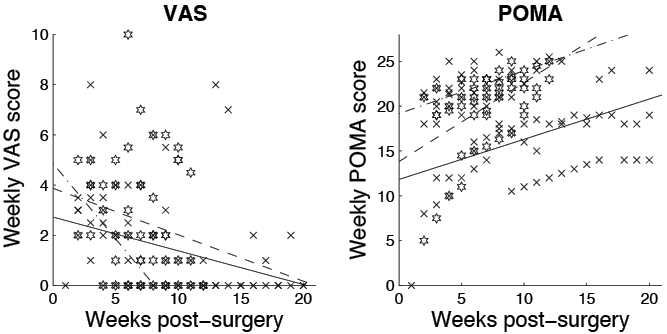
Between February 2012 and September 2012, 44 eligible patients with hip fracture were admitted. Nineteen patients were excluded based on lack of informed consent (n = 15), pathological fractures (n = 2), and cognitive problems (n = 2). Two patients were excluded due to a short (1 week) admission to the nursing home, one patient refused to participate in further measurements and one patient needed revision surgery. In total, 21 patients with a mean age of 80.3 years (standard deviation; SD 8.3) were included in the study (6 men and 15 women). The fractures were proximal neck fractures (n = 15), pertrochanteric fractures (n = 4) and subtrochanteric fractures (n = 2). The operative treatments were hemiarthroplasty (n = 13), proximal femoral nails (n = 4), gamma nail (n = 2), dynamic hip screw (n = 1) and cannulated screws (n = 1). Co-morbidities were cardiovascular in 86% of the patients and diabetes type 2 in 14%. The mean length of rehabilitation was 11 weeks (range 3–19 weeks). Seven patients were admitted for less than 8 weeks, 8 patients between 8 and 12 weeks, and 6 patients more than 12 weeks. There were no significant differences between groups in the amount of pain in the first 8 weeks. The POMA however, did show a significant difference between the short and long rehabilitation groups in the first 8 weeks of rehabilitation (p < 0.001) (Fig. 2). The amount of pain showed no correlation with weight bearing parameters; however, the POMA showed significant correlations with steps, bouts and loading rate (p < 0.001).
In the entire patient group (n = 21), steps, walking bouts and loading rate increased during rehabilitation, as shown in Fig. 3. Patients in the short rehabilitation group took more steps than patients in the intermediate and long rehabilitation groups during the first 8 weeks (mean 748 (SD 407) vs 474 (SD 61) vs 166 (SD 36), respectively, p < 0.01). In addition, the patients with short rehabilitation used more intervals than patients in the intermediate and long rehabilitation group (mean 20 (SD 11) vs 17 (SD 2) vs 3 (SD 1), p < 0.01) and the patients with short rehabilitation had a higher loading rate than patients in the intermediate and long rehabilitation group (mean 181 (SD 83) vs 128 (SD 7) vs 102 (SD 9), p < 0.01). These data are summarized in Table I.
|
Table I. Steps, walking bouts and loading rate in the first 8 weeks for the short, intermediate and long rehabilitation group |
|||
|
Short Mean (SD) |
Intermediate Mean (SD) |
Long Mean (SD) |
|
|
Steps |
748 (407) |
474 (61)* |
166 (36)** |
|
Walking bouts |
20 (11) |
17 (2) |
3 (1)** |
|
Loading rate (%BW/s) |
181 (83) |
128 (7)* |
102 (9)* |
|
*The result is significantly different from the short rehabilitation group (p < 0.01). **The result is significantly different from the short rehabilitation group (p < 0.0001). %BW/s: percentage of bodyweight/s; SD: standard deviation. |
|||
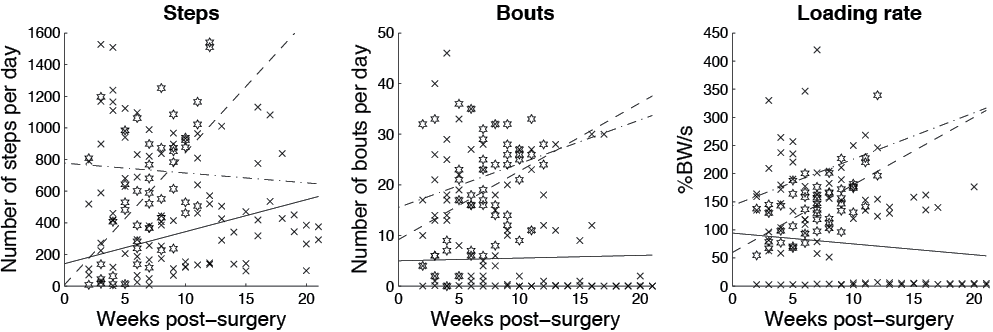
Fig. 3. Weekly weight loading parameters of rehabilitating hip fracture patients. Weight loading parameters of hip fracture patients in the short rehabilitating group are indicated by circles, whereas patients in the intermediate and long group are indicated by stars and crosses, respectively. Best-fit lines for the weekly scores are displayed for all 3 patient groups: dash-dot, dashed or solid for the short, intermediate and long rehabilitation groups, respectively. The graphs represent the number of steps (left-hand side), number of bouts (centre) and the loading rate (right-hand side).
Discussion
This study sets out a new way to monitor weight bearing, which generates parameters that demonstrate the progress of rehabilitation. There is a clear relationship between the parameters derived from monitoring weight bearing and the clinical progress of patients.
The steepness of the initial phase of the pressure wave of every step, i.e. the loading rate, changes during the rehabilitation process. As demonstrated in this study, it is the most reliable parameter to describe the progress of rehabilitation. For patients with a short admission to the nursing home this parameter has a significantly faster increase than for patients who take longer to recover. This difference could be explained by the combination of mobility and pain, which will affect the way the patient will land his or her foot on the ground, or initiate a step. When pain is anticipated or the mobility of the patient is insufficient, the placement of the foot on the ground will be careful or slow. As the patient’s condition improves, the steepness increases, leading to a higher loading rate. In our view this phenomenon is unintentional. This parameter, the loading rate, reflects the end product of the rehabilitation programme, as it represents the landing of the foot on the ground, and is therefore a valuable way to monitor the healing process.
The other parameters that show a significant correlation with the progress of rehabilitation are the number of steps and walking bouts. Although these parameters indicate a difference between groups with short, intermediate and long rehabilitation, their value seems less compared with the loading rate as these parameters are intentional, in contrast to loading rate. The number of steps and walking bouts could be influenced by exercise or by the intervention of nursing staff, whereas the loading rate is determined by the patient himself/herself. At this point in the collection of these new data we therefore give more value to the loading rate for monitoring the rehabilitation process.
Monitoring weight bearing using an ambulant device has several potential benefits. First, patients can monitor their healing process themselves at home following a fracture. Secondly, constant monitoring can be performed without supervision, improving costs and optimizing personnel employment. Remote monitoring of data by physical therapists or other healthcare providers could decrease the contact required in the physical therapy office or outpatient clinic. Thirdly, when the monitoring device is equipped with an intervention programme, mobilization can be optimized per patient. The parameters with the best relation with clinical outcome, steps, walking bouts, and loading rate, are, in our opinion, the first parameters to tailor the intervention. This would improve the rehabilitation programme and patient outcome. Intervention in the rehabilitation has not yet been performed using the device described here, but other studies have shown that patients benefit from specific training programmes after a hip fracture (13). The device used in the current study aims to contribute to these results.
In conclusion, with the current introduction of a new insole device, Feetb@ck, we have shown that weight bearing can be monitored in a geriatric population in a nursing home. The data indicate that it is possible to monitor weight bearing. A clear correlation was seen between the loading rate and the length of stay in a nursing home in the first 8 weeks of rehabilitation.
AcknowledgementS
The authors declare that they have no financial relationship with Evalan, the manufacturer of the FeetB@ck device. Evalan has had no influence on the interpretation of data and the final conclusions drawn. The Feetb@ck device is available for the European market (www.sensistep.com).
References

