Masahiko Mukaino, MD, PhD1,2*, Takashi Ono, MD, PhD3*, Keiichiro Shindo, MD, PhD1,4, Toshiyuki Fujiwara, MD, PhD4, Tetsuo Ota, MD, PhD1,2, Akio Kimura, MD, PhD1,4, Meigen Liu, MD, PhD4 and Junichi Ushiba, PhD3
From the 1Department of Rehabilitation Medicine, Keio University Tsukigase Rehabilitation Center, Tokyo, 2Department of Rehabilitation Medicine, Asahikawa Medical University Hospital, Asahikawa, 3Department of Biosciences and Informatics, School of Fundamental Science and Technology, Graduate School of Keio University, Yokohama and 4Department of Rehabilitation Medicine, Keio University School of Medicine, Tokyo, Japan. *Both of these authors contributed equally to this work.
OBJECTIVE: Brain computer interface technology is of great interest to researchers as a potential therapeutic measure for people with severe neurological disorders. The aim of this study was to examine the efficacy of brain computer interface, by comparing conventional neuromuscular electrical stimulation and brain computer interface-driven neuromuscular electrical stimulation, using an A-B-A-B withdrawal single-subject design.
METHODS: A 38-year-old male with severe hemiplegia due to a putaminal haemorrhage participated in this study. The design involved 2 epochs. In epoch A, the patient attempted to open his fingers during the application of neuromuscular electrical stimulation, irrespective of his actual brain activity. In epoch B, neuromuscular electrical stimulation was applied only when a significant motor-related cortical potential was observed in the electroencephalogram.
RESULTS: The subject initially showed diffuse functional magnetic resonance imaging activation and small electroencephalogram responses while attempting finger movement. Epoch A was associated with few neurological or clinical signs of improvement. Epoch B, with a brain computer interface, was associated with marked lateralization of electroencephalogram (EEG) and blood oxygenation level dependent responses. Voluntary electromyogram (EMG) activity, with significant EEG–EMG coherence, was also prompted. Clinical improvement in upper-extremity function and muscle tone was observed.
CONCLUSION: These results indicate that self-directed training with a brain computer interface may induce activity- dependent cortical plasticity and promote functional recovery. This preliminary clinical investigation encourages further research using a controlled design.
Key words: brain computer interface; stroke; hemiparesis; neuromuscular electrical stimulation; rehabilitation.
J Rehabil Med 2014: 46: 00–00
Correspondence address: Junichi Ushiba, School of Fundamental Science and Technology, Graduate School of Keio University, Room 404, Building 14, 3-14-1 Hiyoshi, Kohoku, Yokohama, Kanagawa 223-8522, Japan. E-mail: ushiba@brain.bio.keio.ac.jp
Accepted Nov 18, 2013; Epub ahead of print Feb 28, 2014
INTRODUCTION
Brain-computer interface (BCI) technology is a newly developed technique that is attracting much attention. Recent studies have shown that brain signals measured using electroencephalography (EEG) or magnetoencephalography (MEG) provide information for the presumption of motor intention (1). Using BCI technology, real-time feedback concerning cortical activity can be provided to the patient through visual and somatosensory information.
In the present study, we developed a BCI system controlling neuromuscular electrical stimulation (BCI-driven NMES) as a closed-loop feedback system for use with severe paresis, and examined whether there were advantages of a closed-loop BCI system compared with an open-loop NMES system to restore motor ability. We used a single-subject A-B-A-B experimental design, and employed a series of neurological and clinical assessments to comprehensively evaluate improvement of the motor system. Upstream to downstream measures were used, including regional cerebral electric and blood oxygenation responses, corticospinal connectivity, voluntary muscle activity, kinetic performance, and muscle tone. The reproducibility of neurophysiological changes simulated by BCI was also evaluated.
CASE REPORT
A 38-year-old right-handed Japanese male, with severe chronic left hemiplegia due to right putaminal haemorrhage 14 months earlier, was the subject of this study. The patient had already received 7 months of inpatient rehabilitation after the onset of putaminal haemorrhage, including the last 2 months in Keio Tsukigase Rehabilitation Center (KTRC), and following 7 months of outpatient rehabilitation. Rehabilitation examination at hospital admission revealed that the patient’s upper limb section of the Fugl-Meyer assessment (FMA) score for testing physical motor performance at the paralysed upper extremity was 27 (range 0–66), and his modified Ashworth scale (MAS) score for testing muscle spasticity at the paralysed finger was 2 (range 0–4). These scores were unchanged from those acquired 8 months prior to admission to the present study, including 30 days of previous inpatient rehabilitation in KTRC. His hand function was severely impaired, and surface electromyogram (EMG) activity from the affected extensor digitorum communis (EDC) was absent. Sensory examination showed a mild decrease in position sense in all fingers. Pin-prick and touch senses were also mildly impaired. He was independent in activities of daily living, and used a T-cane and plastic ankle-foot orthosis. His cognitive abilities were intact. Before the experiment, the patient gave written informed consent to participate in this study. The only medication that the patient received was hypnotic, and no anti-spasticity drugs were used during inpatient rehabilitation.
The experimental design described below followed the Declaration of Helsinki on medical protocol and ethics, and was approved by the Keio University School of Medicine ethics committee.
Experimental design
The study incorporated a within-subject A-B-A-B withdrawal design in which we alternated epochs A (control) and B (BCI). During epoch A, the patient was asked to attempt finger opening for 3 s at maximal voluntary effort. During this period, simultaneous NMES (see Appendix S11) was applied to the paralysed finger-opening muscle. Next, a 3-s rest period was given, and stimulation was halted. The trial lasted for 6 s and was repeated for 60 min, and was conducted on weekdays for 2 weeks (10 days in total).
During epoch B, the patient was similarly asked to attempt finger opening for 3 s at maximal voluntary effort. The BCI monitored motor-related cortical potential in the electroencephalogram (EEG) recorded over the sensorimotor area in the affected hemisphere, and NMES was given only if the amplitude of motor-related cortical potential reached a pre-determined threshold, and amplitude was maintained for 1 s (Fig. 1). A relative power decrease in the sensorimotor rhythm from baseline, called event-related desynchronization (ERD), is known as a biomarker of the excitability of the primary motor area (2). We used ERD as a trigger source of NMES to form the closed-loop structure, which couples continuous motor-related brain activity with somatosensory activity by NMES. The detailed settings for the EEG recordings and the calculation have been described previously (3), and are summarized in Appendix S11. As the training settings of the BCI-NMES and the NMES were different, the subject was not blinded to the training contents.
The experiment was discontinued for the day if the patient reported exhaustion. The subject ended the treatment early on 3 days: 2 in the first BCI epoch and 1 in the second BCI epoch. In both epochs, traditional occupational therapy (OT) was performed 40 min/day after each intervention, which included thermotherapy, continuous muscle stretch, and practicing functional activities (i.e. wiping or holding paper down). The patient cancelled OT only once, in the first BCI epoch; he did not end OT early during the NMES epochs. No additional exercise apart from OT was performed during the epochs.

Outcome measures
The following functional magnetic resonance imaging (fMRI), EEG, surface EMG of the affected EDC muscle, and clinical evaluations were performed before the first session and at the end of each training epoch. The researchers involved in the analyses of fMRI, EEG and EMG were blinded as to the training contents.
fMRI data acquisition. Whole-brain fMRI (Excelart/Vantage, Toshiba Medical Systems, Tokyo, Japan) was performed at 1.5 T, with standard scanning software, on the day of admission and the last days of each training period. The following parameters were used for fMRI experiments: repetition time (TR)/echo time (TE)/flip angle 3000 ms/40 ms/90º; field of view 256 mm; matrix size 96 × 96; and slice thickness 5 mm (slice gap 1 mm). Between repetitions, 23 axial sections (slices) were acquired in a continuous manner (i.e. 23 slices per 3 s).
Motor task paradigm. The paradigm was a block design (5 rest and 5 task blocks, 30 s each). We employed a self-paced movement paradigm at 1 Hz, in which the subject was directed to employ self-paced finger-extension movements with the affected hand for 30 s with maximal effort (4). To observe unintentional movement of other muscles, direct observation was performed, as described previously.
fMRI data analysis. Data were processed using a general linear model using Statistical Parametric Mapping software (SPM8; Wellcome Department of Cognitive Neurology, London, UK). The detailed methods for fMRI data analysis are shown in Appendix S11.
EMG analysis. Surface EMG was measured using electrodes on the EDC. The percent change in root mean square (RMS) after the task cue to reference (pre-task) RMS was calculated. To examine the change in the RMS ratio, we used the Kruskal-Wallis and Mann-Whitney U tests and applied Bonferroni’s correction for multiple comparisons.
Corticomuscular coherence. Corticomuscular coherence (CMC) measures the functional coupling between the cortex and muscle. (5) The details of the coherence calculation are shown in Appendix S11. Coherence is expressed as a real number between 0 and 1, with 1 indicating a perfect linear association. EEG-EMG coherence was considered significant when it was within > 95% confidence limits computed from the number of epochs (epochs 100; limit 0.030).
Clinical evaluation. For evaluation of motor function, the upper extremity section of FMA was performed. Finger spasticity was measured using the MAS. Evaluation was performed by a physician and an occupational therapist who were both blinded to the experimental design.
RESULTS
Functional magnetic resonance imaging changes
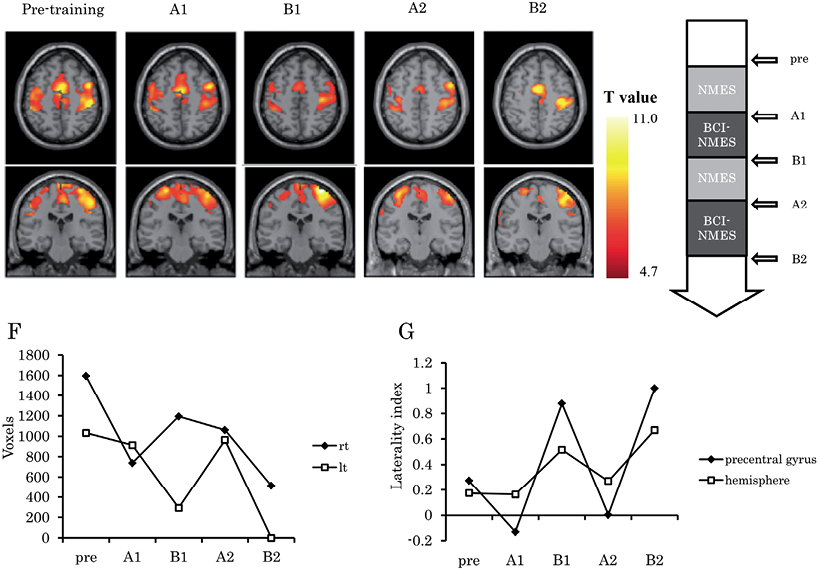
fMRI activation during affected hand movement prior to training sessions was associated with extensive participation of active areas in both hemispheres, including the bilateral primary motor cortex, primary sensory cortex, supplementary motor area (SMA), and the bilateral premotor cortices (Fig. 2A). The total activated area gradually decreased through the training epochs, and in the BCI-NMES epochs (B1 and B2), lateralization of the activated area was observed. The calculated laterality index (LI) of voxels in the bilateral precentral gyrus and hemisphere was unchanged or decreased during the NMES epoch, while it was markedly increased during the BCI-driven NMES epoch (Fig. 2B–G).
Neurophysiological changes
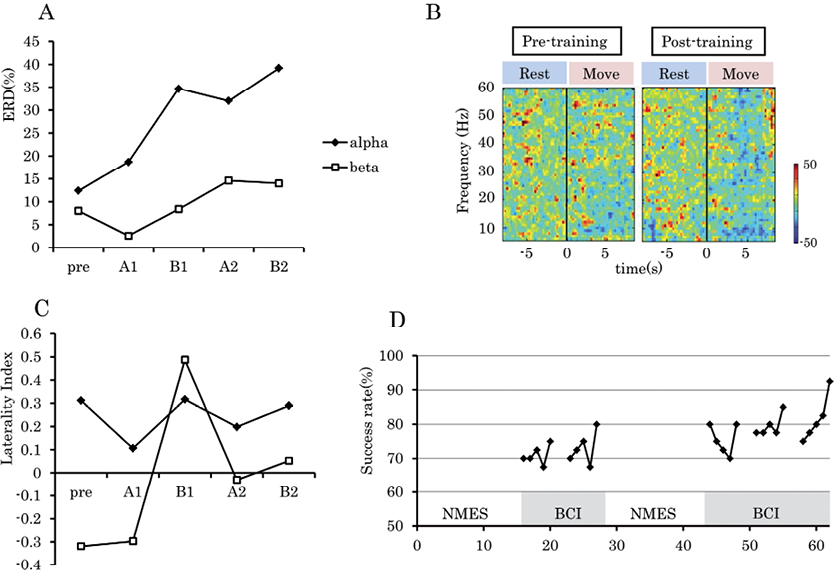
The ERD in the right primary sensory-motor cortex (SM1) gradually increased during the training epochs, both in the alpha (mu) and beta bands (Fig. 3A). In the time-frequency map before the training epochs, the generation of ERD was not evident by motor intention. In contrast, the time-frequency map on the last day clearly showed ERD in alpha (mu) and beta bands (Fig. 3B). Similar to the fMRI study, the LI of the bilateral SM1 markedly increased only during the BCI-NMES epoch (Fig. 3C). The success rate of triggering NMES by ERD gradually increased during the BCI-NMES epoch (Fig. 3D).
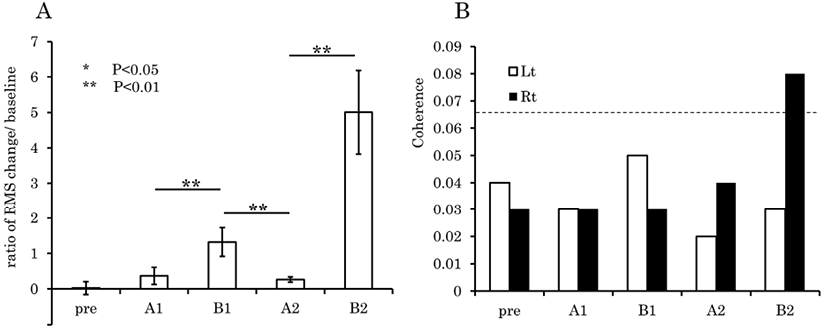
The change in the averaged ratio of RMS of surface EMG activity on the EDC during the task to initial baseline was calculated (Fig. 4A). There was very little increase (3%) in EMG activity of the EDC by the “extend finger” instruction on the day before training started. After the first NMES epoch, there was a 37% increase in RMS value. After the first BCI epoch, the value reached a 132% increase compared with baseline. However, the RMS ratio on the last day of the second NMES epoch decreased to 27%. Finally, after the second BCI session, the ratio was increased to 500% relative to the reference EMG.
The CMC in the beta band was calculated using EEG and EMG of the affected EDC (Fig. 4B). The coherence of the EEG in contralateral SM1 and the EMG of upper limb muscles have been shown to be related to functional recovery after stroke (6). Before the sessions started, CMC was not significant. At the end of all sessions, CMC of the left EDC and EEG of the contralateral SM1 exceeded the 95% confidence level.
Clinical changes
The result of the clinical examination of motor function is shown in Table I. The FMA score increased to 34 in the final evaluation, which was mostly achieved during BCI-NMES epochs. This increase in FMA score was not due to improvement in finger function, but was mostly due to improvement in proximal muscle movement in the paretic limb, which was not directly involved in the experimental design. Despite improvement in EMG and EEG activity, no practical finger movement was regained. However, the patient was able to keep his fingers extended and to hold paper down while writing, which was not possible before the intervention. Finger spasticity was reduced from 2 to 1 on the modified Ashworth scale, and this improvement was seen during BCI-driven NMES epochs.
|
Table I. Clinical scores during conventional neuromuscular electrical stimulation and brain computer interface–neuromuscular electrical stimulation (BCI-NMES) training |
|||||
|
|
Before |
A1 |
B1 |
A2 |
B2 |
|
MAS |
2 |
2 |
1+ |
1+ |
1 |
|
FMA U/E |
26 |
27 |
31 |
31 |
34 |
|
MAS: modified Ashworth Scale; FMA U/E: upper extremity section of Fugl-Meyer assessment; Before the start of intervention; A1: after the first epoch A (NMES); B1: after the first epoch B (BCI-NMES); A2: after the second epoch A; B2: after the second epoch B. |
|||||
DISCUSSION
The effect of BCI training is often explained by the mechanism of motor learning with closed-loop feedback (7). In our model, the real-time feedback of brain activity was provided with NMES as strengthened proprioceptive feedback. Temporary re-establishment of closed-loop feedback by a BCI system may support the retention of motor-related brain activity after corticospinal tract injury. Furthermore, this BCI-driven NMES system, without visual feedback of brain activity, may indicate the importance of proprioceptive feedback contingent on motor-related brain activity.
Recently, several studies have shown a robust effect of EMG-triggered NMES, which provides closed-loop biofeedback for paralysed limbs (8–10). However, severely hemiplegic patients who show less voluntary EMG cannot use this method. The BCI-NMES could be a substitute for those patients, and may allow some restoration of motor control.
It is possible that the observed changes in EEG or fMRI reflect the simple learning of emerging ERD-like activity, which is independent of practical motor function. However, the observed lateralization of brain activity without any laterality feedback implies that such a simple biofeedback mechanism is not enough to explain the observed changes.
In conclusion, BCI-driven NMES was associated with improvement in motor function and plasticity of the motor cortex in our patient, which was superior to that achieved by NMES only. Although this was a single-subject study, the present data strongly suggest the feasibility of using BCI technology, which accesses the plasticity of the motor system as a whole, from brain to muscle, in stroke rehabilitation. These results encourage further examination with more controlled studies for training with BCIs, especially for severe motor paresis.
ACKNOWLEDGEMENTS
This study was supported by “Brain Machine Interface Development” under the Strategic Research Program for Brain Sciences by the Ministry of Education, Culture, Sports, Science and Technology of Japan.

1http://www.medicaljournals.se/jrm/content/?doi=10.2340/16501977-1785
REFERENCES


