Marianne Reinkingh, MD1, Heleen A. Reinders-Messelink, MSc, PhD1, Pieter U. Dijkstra, PhD1,2, Karel G. B. Maathuis, MD PhD1 and Corry K. van der Sluis, MD PhD1
From the 1Department of Rehabilitation Medicine and 2Department of Oral and Maxillofacial Surgery, University of Groningen, University Medical Center Groningen, Groningen, The Netherlands
OBJECTIVES: To compare stump sensibility in children with upper limb reduction deficiency with sensibility of the unaffected arm and hand. In addition, to evaluate the associations between stump sensibility, stump length and activity level.
DESIGN: Cross-sectional study.
SUBJECTS: Children and young adults aged 6–25 years with upper limb reduction deficiency.
METHODS: Threshold of touch was measured with Semmes-Weinstein monofilaments, stereognosis was measured with the Shape-Texture Identification test and kinaesthesia and activity level was measured with the Child Amputee Prosthetics Project – Functional Status Inventory and the Prosthetic Upper Extremity Functional Index.
RESULTS: A total of 31 children with upper limb reduction deficiency (mean age 15 years, 3 prosthesis wearers) were investigated. The threshold of touch of the stump circumference was lower (indicating higher sensibility) than of the unaffected arm (p = 0.006), hand (p = 0.004) and stump end-point (p = < 0.001). Long stumps had higher threshold of touch (indicating lower sensibility) than short stumps (p = 0.046). Twenty-nine children recognized 1 or more shapes or textures with the stump. Kinaesthesia in the affected and unaffected sides was comparable. Sensibility was not correlated with activity level.
CONCLUSION: Threshold of touch, stereognosis and kinaesthesia of the affected sides were excellent. Threshold of touch of the stump circumference was lower (indicating higher sensibility) than of the unaffected arm and hand. High stump sensibility may clarify good functioning in the children without prostheses and contribute to prosthesis rejection.
Key words: child; upper limb reduction deficiency; sensibility.
J Rehabil Med 2013; 45: 00–00
Correspondence address: Corry K. van der Sluis, Department of Rehabilitation Medicine, Center for Rehabilitation, University Medical Center Groningen, PO Box 30.001, NL-9700 RB, Groningen, The Netherlands. E-mail: c.k.van.der.sluis@umcg.nl
Accepted May 31, 2013; Epub ahead of print Sep 16, 2013
Introduction
Children with upper limb reduction deficiency (ULRD) have many options to achieve the same level of function as their peers (1). Some children use prostheses, while others function adequately without them (1, 2). Prosthetic use does not appear to be associated with relevant functional differences in daily activities or quality of life when children who use them are compared with those who do not (1). Prosthesis rejection rates in children with ULRD vary from 10% to 58% (3–7). The main reasons for prosthesis rejection are lack of function and comfort (4) or, possibly, lack of sensory feedback from the stump (3–5). Surprisingly little information on stump sensibility in ULRD is available to date.
A higher level of sensibility of the stump was found compared with that of the unaffected side in a group of 13 children with ULRD (8). Two-point discrimination of the stump in 5 congenital amputees was comparable to that of the intact arm of healthy controls (9). Significantly lower threshold of touch, indicating higher sensibility, at the stump of the deficient limb was found compared with the intact limb (10). However, in that study no association between threshold of touch and either functional activities or prosthetic use was found. One of the limitations of the latter study was that using pre-defined testing points did not allow individual differences to be measured. Measuring the area that children prefer using for functional activities and examining the corresponding points of the intact arm could provide more meaningful information (10).
Different modalities of sensibility exist; for instance, threshold of touch, 2-point discrimination, kinaesthesia and stereognosis are used to measure sensibility. Stereognosis plays an important role in the hand function of children with cerebral palsy (11, 12). Impairments in stereognosis are correlated with motor function impairments (11). Children with a neurological motor disorder were found to have poorer stereognosis than healthy children (13). Because minor neurological disorders have been associated with ULRD (14), it is interesting also to investigate stereognosis in these children. Stereognosis has not yet been investigated in ULRD.
Children with longer stumps have been shown to make more use of the stump as a sensory tool (3, 7). These children use their stump for fixating and supporting. As such, they appear to make use of various biomechanical advantages of the stump length. Stump length is associated with prosthesis rejection; children with a shorter stump reject prostheses less frequently (13%) than children with a longer stump (45%) (3). However, information on the relationship between sensibility and stump length has not been available to date.
The primary aim of our study is to evaluate differences in sensibility of the stump in children with ULRD compared with the unaffected arm and hand. The secondary aim is to evaluate the associations between stump sensibility, stump length and activity level.
Methods
Children and young adults with ULRD aged 6–25 years were asked to participate. The participants were identified using local databases from the Center for Rehabilitation of the University Medical Center Groningen (UMCG) and the Centre for Rehabilitation “Vogellanden” Zwolle, the Netherlands. Children with bilateral upper limb deficiency, peripheral nerve damage, neurological disease, other hand impairment, mental retardation or insufficient understanding of the Dutch language were excluded. This study was approved by the ethics committee of the UMCG (METc 2009/024). Before entering the study, an informed consent form was signed by the parents of children younger than 12 years of age, by the parents and their young adolescent children (if the participating child was 12–17 years of age) or by participants alone if they were 18 years or older.
Measurements were performed by one researcher (MR) at the Centre for Rehabilitation UMCG or at patients’ homes in a quiet, non-distracting environment. Following the World Health Organization (WHO) International Classification of Functioning, Disability and Health system (ICF) we measured the categories body function and activity (15). Body function measurements were collected via sensibility tests (threshold of touch, stereognosis and kinaesthesia) and activities were measured using 2 questionnaires. Different terminology is used to describe sensibility (sensation, sensory, etc.) (16). In our research, we use the term “sensibility”, since “sensation is the central perception of a stimulus, while sensibility is the peripheral manifestation” (16). Stump length was measured in forearm deficiencies from the olecranon to the distal end of the stump using a tape measure. Presence of callus formation on the stump was noted. Parents and participants also completed a questionnaire with general aspects of prosthetic use in the present and past.
Sample size calculations were based on estimated differences in mean threshold of touch values. Raw data of Johnson revealed a difference between stump circumference and the unaffected side of 0.24 (standard deviation (SD) 0.46) (10), which resulted in the need for at least 31 participants (alpha 0.05, power 0.80) (10).
Threshold of touch
Threshold of touch was tested using the Touch-test™ Sensory Evaluator (Semmes-Weinstein Monofilaments; North Coast Medical, Inc., Gilroy, CA, USA). Twenty monofilaments are used to test relative threshold levels of touch. They are numbered from 1.65 ≈ 0.0045 g to 6.65 ≈ 446.7 g (17). Low values (1.65 ≈ 0.0045 g to 2.83 ≈ 0.07 g) indicate normal threshold of touch. Intermediate values (3.22 ≈ 0.17 g to 3.61 ≈ 0.41 g) indicate diminished light threshold of touch. High values (3.84 ≈ 0.69 g – 6.65 ≈ 446.7 g) indicate diminished or loss of protective threshold of touch (hand thresholds; Touch-test™ Sensory Evaluator Chart, 2011 North Coast Medical, Inc. (17)). These values are general values and not specifically established for use in children. The measurement procedure was standardized as recommended (18). The starting point was the 2.83 ≈ 0.07 g filament. If there was no response to the first application, 3 attempts were performed maximally, which is the recommended procedure to ensure that 1 of the 3 stimuli is the intended threshold (18). If the filament could not be sensed by participants, a thicker filament was used, and if the filament could be felt, a thinner filament was used. The thinnest monofilament that could be identified was recorded. In younger children their vision was blocked with a blindfold, whereas older children and young adolescents closed their eyes. Filaments were tested on both arms, alternating between limbs. Testing points were distributed in 4 areas: stump circumference, stump end-point, the unaffected arm (at the same level as the stump circumference) and the intact hand (fingers and palm of the hand) (Fig. 1). If rudimentary fingers were present, they were also tested. Furthermore, children were asked which area of the stump they preferred to use in functional activities, as advised previously (10). That area, and the corresponding area of the unaffected arm, were tested. The Semmes-Weinstein monofilament test has demonstrated high content validity and adequate criterion validity (19). Intra-rater reliability is consistently high, while inter-rater and test-retest reliability are variable across studies and populations (19, 20). The test is suitable for use in children 6 years of age and older (mean intraclass correlation coefficient (ICC) 0.78) (21).
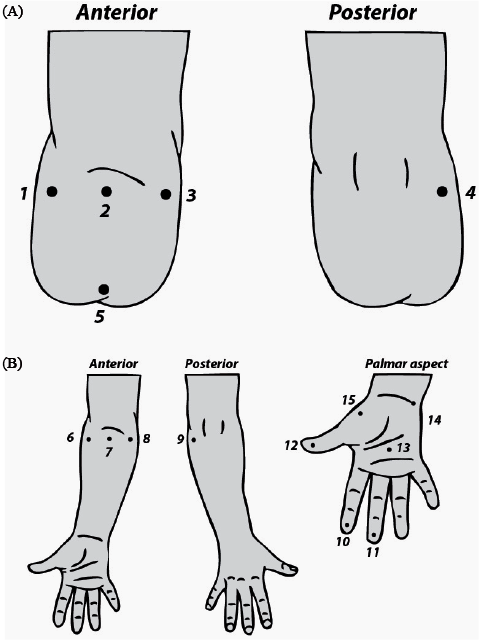
Fig. 1. Threshold of touch testing points (based on: Johnson et al., 2002) (10). (A) 1– 4: testing points on the stump circumference (2.5 cm from stump end-point). 5: testing point on the stump end-point. (B) 6–9: testing points on the unaffected arm; 10–15: testing points on the hand.
Stereognosis
Stereognosis was tested with the Shape-Texture Identification test (STI test™) (22). The STI test™ assesses the ability to identify shapes and textures without visual feedback. The test consists of 6 discs. Three of these discs each contain 3 different shapes (cube, cylinder and hexagon), and 3 of these discs are marked with dots (in groups of 1, 2 or 3 raised metal dots in a row). The discs have 3 degrees of difficulty; decreasing sizes of the shapes (15, 8 and 5 mm) and decreasing distances between the dots (15, 8 and 4 mm). Children were instructed to identify the shape and textures of the exposed objects (22). First, 15-mm sized shapes were randomly exposed to the index finger and then to the stump, followed by 8-mm sized shapes and then 5-mm sized shapes. The next step was exposure to textures, starting with the largest. Each object was presented only once (22). The identification of the 3 different shapes or dots at each degree of difficulty were required to be correct in order to score 1 point and proceed to the next degree of difficulty. The maximum possible score was 6 points, which is also the norm score (22). Stump and index finger were tested. Participants were allowed to use the side of the stump they preferred, including rudimentary fingers. While testing the index finger, participants were not allowed to use their nail. The STI test™ shows a good validity, reliability and responsiveness and is preferred for testing stereognosis (test-retest Kappa 0.79, inter-tester Kappa 0.66) (20). Psychometric properties of the STI test™ in measuring children are not available.
Kinaesthesia
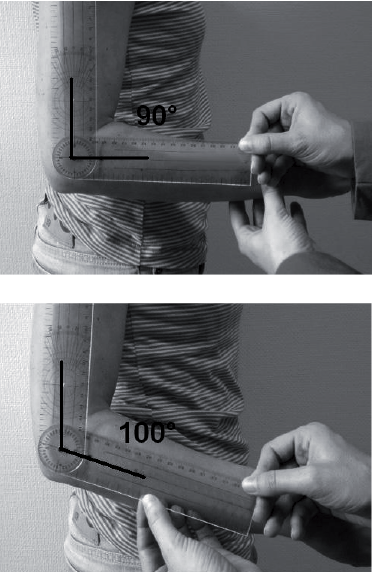
Kinaesthesia was tested based on the procedure described by Thibault et al. (21). The direction of shoulder and elbow joint displacement of unaffected and affected side was measured. The unaffected limb was tested before the affected limb. Limbs were displaced by 10º (Fig. 2). The amount of joint displacement was monitored using a goniometer. The joint was flexed and extended 5 times in a predetermined random order. The participants were asked to identify the direction of the displacement. The number of correct responses was recorded for each joint. The maximum score possible for each joint was 5 points. This procedure is objective, reproducible and suited for use in children aged 6 years and older (21). The reliability of this procedure is excellent (mean Kappa 0.81) (21).
Fig. 2. Kinaesthesia: the elbow is displaced by 10 degrees.
Activities: CAPP-FSI and CAPP-FSIP
To measure children’s level of activities, the Child Amputee Prosthetics Project – Functional Status Inventory (CAPP-FSI) (23) and the Child Amputee Prosthetics Project – Functional Status Inventory for Preschool children (CAPP-FSIP) (24) were used. The CAPP-FSI is designed for children aged 8–17 years who have either an upper or a lower limb deficiency. The CAPP-FSIP is an instrument used to test preschool-aged children who range in age from 4 to 7 years. Both questionnaires are parent-reported ratings of the child’s performance in everyday behaviours including self-care tasks and other developmentally appropriate activities. Adolescents aged 18 years or more completed the version used for older children. Tasks are rated on 2 scales, “Does the activity” and “Uses prosthesis”, using a 5-point Likert scale. Scores vary between 0 and 4 points; higher scores reflect greater independence in performance and higher frequency of prosthesis use. Only the upper extremity items were used. These questionnaires have demonstrated internal consistency, content and construct validity (23, 24).
Activities: PUFI
The Prosthetic Upper Extremity Functional Index (PUFI) (25) was specifically developed for use in children with ULRD and was used to evaluate the extent to which children use the deficient limb for daily activities, the comparative ease of task performance with and without prosthesis and the perceived usefulness of the prosthesis. The children were asked to answer 5 questions per specific activity: (A) Do you do the activity; (B) Method of performance; (C) Ease of performance with prosthesis; (D) Usefulness of prosthesis; and (E) Ease of performance without prosthesis. The answers resemble a Likert scale and range from low to high performance. A score of 100% means that all of the activities were performed according to the “best” method of performance. Children who did not wear a prosthesis only answered questions A, B and E. Versions for younger (age ≤ 6 years) and older children (7–18 years) are available. Adolescents aged 18 years and older completed the version for older children. The PUFI has shown good test-retest reliability (ICC > 0.65) and acceptable validity (25, 26).
Statistical analysis
A multi-level data analysis was performed in MLwiN (version 2.22), in which all threshold of touch observations (Fig. 1) were analysed, while taking into account autocorrelation due to multiple observations within participants. The results of the threshold of touch tests was the outcome variable. Initially the analyses were performed with the threshold of touch values in g. The residuals, however, were not normally distributed, therefore the analyses were performed with the handle markings (residuals were then normally distributed). Predictor variables included the site of testing (i.e. stump circumference, stump end-point and the corresponding points on unaffected arm and hand), rudimentary fingers, stump length, age and gender (men = 0, women = 1). The site of testing was entered as a categorical variable with the stump circumference measurements as a reference category. Rudimentary fingers were used as a reference category to compare sensibility of the rudimentary fingers with the other testing sites.
Predictors were entered into the model in a stepwise fashion. If the model fit increased significantly or beta was significant, predictors remained in the model. Random intercepts and random slopes were explored. If the model fit improved significantly, random effects were retained in the model. During data exploration, it became evident that one person exhibited extreme threshold of touch values for the stump circumference (4.56 ≈ 3.6 g to 6.10 ≈ 125.9 g), probably as a result of callus formation on the stump. Therefore, two multi-level analyses were performed, one including the data of this person and one excluding the data of this person.
A Wilcoxon signed-rank test was performed in Predictive Analytics Software Statistics 18 to analyse differences in threshold of touch of the area of the stump preferred in functional activities and the corresponding area on the unaffected arm, as well as differences in stereognosis and kinaesthesia.
Children’s total CAPP-FSI and CAPP-FSIP scores were divided by the number of applicable items. Note that not all of the children performed each of the activities.
To analyse PUFI results, percentages were calculated according to maximum performance scores or usefulness scores. A Spearman correlation was performed to relate the CAPP-FSI, CAPP-FSIP and PUFI scores to threshold of touch sensibility of the stump circumference.
Results
Participants
A total of 51 children and young adults met the inclusion criteria. Six of the children could not be contacted and 14 children refused to participate. A final total of 31 children and young adults (18 boys and 13 girls) participated in the study and completed all of the test procedures (Table I). The mean age was 15 years. Only 3 children wore a prosthesis (1 myo-electric prosthesis, 1 cosmetic prosthesis and 1 passive prosthesis used during eating) (Table II). Of the group of non-wearers, 24/28 had used a prosthesis in the past. Feeling clumsy with the prosthesis and a lack of functional improvement were the main reasons for prosthesis rejection (Table II). For the child with the upper arm deficiency, stump length was not measured. This child was excluded from the analyses regarding stump length. Five children had some callus formation on their stump.
An overview of the results for the total group, prosthesis wearers and prosthesis non-wearers and different levels of deficiency is presented in Table III.
|
Table I. Patient characteristics (n = 31) |
|
|
Characteristics |
|
|
Gender, boys, n |
18 |
|
Age, years, mean (SD) |
15 (5.8) |
|
Side of deficiency, left, n |
19 |
|
Level of deficiency |
|
|
Carpus |
8 |
|
Below elbow |
21 |
|
Trough elbow |
1 |
|
Upper arm |
1 |
|
Stump length, cma, median (IQR) |
10.3 (9.0–21.3) |
|
Rudimentary fingers |
|
|
0 |
3 |
|
≥ 1 |
28 |
|
aFor the one subject with an upper arm deficiency, stump length was not assessed. SD: standard deviation; IQR: interquartile range. |
|
|
Table II. Prosthesis use in the present and past (n = 31) |
|
|
|
n |
|
Currently wearing prosthesis |
3/31 |
|
Prosthesis use in the past (non-wearers) |
24/28 |
|
Reasons for prosthesis rejection (more than one answer possible) |
24/28 |
|
Clumsy |
17 |
|
No functional gain |
15 |
|
Heavy |
3 |
|
Sweating |
2 |
|
Pain |
2 |
|
Sensibility |
2 |
|
Skin irritation |
1 |
|
Other |
6 |
|
Table III. Results of threshold of touch (grams) (17). Shape Texture Identification test, kinaesthesia and activities levels (CAPP-FSI, CAPP-FSIP, PUFI) |
||||||
|
Total group Median (IQR) |
Prosthesis non wearers Median (IQR) |
Prosthesis wearers Median (IQR) |
Level of deficiency: carpus Median (IQR) |
Level of deficiency: lower arm Median (IQR) |
Level of deficiency: through elbow, upper arm Median (IQR) |
|
|
Threshold of touch |
||||||
|
Number of patients |
31 |
28 |
3 |
8 |
21 |
2 |
|
Stump circumference |
0.045 (0.020–0.142) |
0.068 (0.022–0.167) |
0.025 (0.018–0.045) |
0.100 (0.081–0.356) |
0.035 (0.020–0.107) |
0.025 (0.018–0.031) |
|
Stump end-point |
0.166 (0.023–0.407) |
0.166 (0.025–0.407) |
0.005 (0.005–0.068) |
0.287 (0.166–0.407) |
0.068 (0.005–0.407) |
0.117 (0.068–0.166) |
|
Hand |
0.080 (0.033–0.104) |
0.080 (0.033–0.104) |
0.097 (0.034–0.097) |
0.084 (0.054–0.103) |
0.083 (0.033–0.104) |
0.028 (0.022–0.034) |
|
Arm |
0.085 (0.021–0.215) |
0.121 (0.020–0.221) |
0.067 (0.035–0.085) |
0.136 (0.097–0.188) |
0.077 (0.020–0.251) |
0.028 (0.021–0.035) |
|
Rudimentary fingers |
0.078 (0.023–0.274) |
0.088 (0.023–0.287) |
0.028 (0.023–0.101) |
0.274 (0.112–0.940) |
0.028 (0.023–0.166) |
0.058 (0.016–0.101) |
|
STI, total score |
||||||
|
Number of patients |
30a |
27 |
3 |
8 |
20a |
2 |
|
Stump |
4.0 (3.0–6.0) |
4.0 (3.0–6.0) |
3.0 (0–3.0) |
6.0 (5.0–6.0) |
3.0 (3.0–5.0) |
5.0 (3.0–6.0) |
|
Index finger |
6.0 (6.0–6.0) |
6.0 (6.0–6.0) |
6.0 (5.0–6.0) |
6.0 (6.0–6.0) |
6.0 (6.0–6.0) |
6.0 (6.0–6.0) |
|
Kinaesthesia |
||||||
|
Number of patients |
30a |
27 |
3 |
8 |
20a |
2 |
|
Affected shoulder |
5.0 (5.0–5.0) |
5.0 (5.0–5.0) |
5.0 (4.0–5.0) |
5.0 (5.0–5.0) |
5.0 (5.0–5.0) |
5.0 (5.0–5.0) |
|
Affected elbow |
5.0 (5.0–5.0) |
5.0 (5.0–5.0) |
5.0 (5.0–5.0) |
5.0 (5.0–5.0) |
5.0 (5.0–5.0) |
|
|
Unaffected shoulder |
5.0 (5.0–5.0) |
5.0 (5.0–5.0) |
5.0 (5.0–5.0) |
5.0 (5.0–5.0) |
5.0 (5.0–5.0) |
5.0 (5.0–5.0) |
|
Unaffected elbow |
5.0 (5.0–5.0) |
5.0 (5.0–5.0) |
5.0 (5.0–5.0) |
5.0 (5.0–5.0) |
5.0 (5.0–5.0) |
|
|
Activities |
||||||
|
Number of patients |
30a |
27 |
3 |
8 |
20a |
2 |
|
CAPP-FSI and CAPP-FSIP “does the activity” |
3.71 (3.48–3.92) |
3.70 (3.45–3.92) |
3.75 (3.55–3.96) |
3.86 (3.68–3.96) |
3. 64 (3.40–3.88) |
3.35 (3.16–3.55) |
|
PUFI items A (does the activity %) |
82 (76–90) |
82 (76–90) |
79 (74–82) |
82 (77–88) |
83 (77–90) |
76 (74–79) |
|
PUFI items B (method of performance %) |
93 (84–98) |
94 (90–98) |
72 (56–75) |
99 (96–100) |
91 (83–94) |
65 (56–74) |
|
PUFI items E (ease of performance without a prosthesis %) |
90 (83–95) |
91 (83–95) |
85 (79–87) |
96 (85–99) |
90 (83–93) |
80 (73–87) |
|
aOne person with extreme measurement results was excluded. IQR: interquartile range; CAPP-FSI: Child Amputee Prosthetics Project – Functional Status Inventory; CAPP-FSIP: Child Amputee Prosthetics Project – Functional Status Inventory for Preschool children; PUFI: Prosthetic Upper Extremity Functional Index. |
||||||
Threshold of touch
The results of the multi-level analyses showed that the influence of the outlier on the outcome measures was considerable (Table IV). Including the outlier in the analyses, the threshold of touch of the stump circumference was better than at the stump end-point. Excluding the outlier, threshold of touch of the stump circumference was better than either at the stump end-point or in the unaffected arm and hand. In both analyses, stump length was significantly related to threshold of touch: children with a longer stump had higher threshold of touch scores (indicating lower sensibility). Age and gender did not significantly contribute to the model. Because of the influence of the person with the extreme measurements on the results, we decided to exclude this case in further analyses.
Rudimentary fingers had significantly higher threshold of touch scores (indicating lower sensibility) than the stump circumference and unaffected arm and hand, but no difference between rudimentary fingers and the stump end-point was found (Table IV).
|
Table IV. Results of multi-level analyses of the threshold of touch |
||||||
|
Predictors |
All data |
Extreme values excludeda |
||||
|
(n = 31) β (SE) |
p β |
Mean threshold of touch, g |
(n = 30) β (SE) |
p β |
Mean threshold of touch, g |
|
|
Stump circumference (ref), r |
2.412 (0.159) |
< 0.001 |
0.026 |
2.303 (0.138) |
< 0.001 |
0.020 |
|
Hand, r |
0.125 (0.108) |
0.247 |
0.034 |
0.210 (0.072) |
0.004 |
0.033 |
|
Arm, r |
0.096 (0.111) |
0.387 |
0.032 |
0.188 (0.068) |
0.006 |
0.031 |
|
Stump end-point, r |
0.382 (0.108) |
< 0.001 |
0.062 |
0.368 (0.111) |
< 0.001 |
0.047 |
|
Stump length, fb |
0.014 (0.007) |
0.046 |
0.027 |
0.016 (0.008) |
0.046 |
0.021 |
|
Rudimentary fingers (ref), f c |
3.107 (0.092) |
< 0.001 |
0.128 |
|||
|
Stump circumference, f |
–0.509 (0.111) |
< 0.001 |
0.040 |
|||
|
Hand, f |
–0.389 (0.105) |
< 0.001 |
0.052 |
|||
|
Arm, f |
–0.419 (0.111) |
< 0.001 |
0.049 |
|||
|
Stump end-point, f |
–0.110 (0.154) |
0.475 |
0.099 |
|||
|
Based on the regression coefficients (of the handle markings) the threshold of touch was transformed to grams (g) (17). aOne person with extreme measurement results was excluded. bOf the 1 person with an upper arm deficiency, no stump length data were available because measurements were performed from the olecranon distally. cn = 28; The participant with extreme measurements did not have rudimentary fingers. Β: regression coefficient; SE: standard error of β; r: random effect; f: fixed effect. |
||||||
Sixteen children had an area of the stump that they preferred to use in functional activities. In 14 children, the comparable location on the unaffected arm was tested. In 2 cases the preferred area was the stump end-point, which could not be tested on the unaffected arm. No significant differences were found between the threshold of touch (in g) of this preferred area (median (IQR): 0.028 (0.004–0.068)) and either the stump circumference (0.031 (0.011–0.085) p = 0.532)) or the comparable location of the unaffected arm (0.068 (0.017–0.166) p = 0.256)).
Stereognosis
Only one child was unable to recognize any shapes and textures with the stump. Twenty-nine children could recognize 1 or more shapes or textures with the stump. All children could feel the textures of the STI test with their index finger. Nearly all (29 out of 30) children could feel all of the shapes with the index finger (Table V). A significantly higher level of stereognosis was found on the side of the index finger for both shapes and textures compared with the stump (p < 0.001).
|
Table V. Shape Texture Identification test scores |
|||
|
n = 30 |
Index finger Median (IQR) |
Stump Median (IQR) |
p-value |
|
Texture |
3.0 (3.0–3.0) |
2.5 (1.8–3.0) |
0.001 |
|
Shape |
3.0 (3.0–3.0) |
2.0 (1.0–3.0) |
< 0.001 |
|
Total |
6.0 (6.0–6.0) |
4.0 (3.0–6.0) |
< 0.001 |
|
IQR: interquartile range. |
|||
Kinaesthesia
The kinaesthesia results (n = 30) did not differ between the unaffected and affected shoulder (p = 0.317), nor were differences found between the unaffected and affected elbows (p = 1.000).
Activities: CAPP-FSI and CAPP-FSIP
In the category “does the activity”, a median score of 3.71 (IQR 3.48–3.92) was found (n = 30). This result indicated that all children were highly independent in activities. No significant correlation was found between threshold of touch and activity level (Spearman’s rho; r = 0.268, p = 0.152). All children had median values in the upper quartile of the scale, reflecting a ceiling effect of the questionnaire (Table III). The question “uses prosthesis” was not taken into account in the analysis because there were only 3 prosthesis wearers included in the study.
Activities: PUFI
All children were able to complete the PUFI on their own. The children had a high activity level, they mostly used the best method of performance and had a high ease of performance in the activities (Table VI). Higher threshold of touch test scores (meaning lower sensibility) were correlated with higher activity levels according to PUFI items B (method of performance, r = 0.378, p = 0.039) and E (ease of performance without a prosthesis, r = 0.446, p = 0.014) (Table VI). Categories C and D were not taken into account for the analysis due to the low number of prosthesis wearers.
|
Table VI. Prosthetic Upper Extremity Functional Index (PUFI) scores and the correlation between threshold of touch of the stump and the PUFI (Spearman’s rho) |
|||
|
PUFI items |
|||
|
(A) Does the activity Median % (IQR) |
(B) Method of performance Median % (IQR)a |
(E) Ease of performance without prosthesis Median % (IQR) |
|
|
Total group, n = 30 |
82 (76–90) |
93 (84–98) |
90 (83–95) |
|
Non-wearers, n = 27 |
82 (76–90) |
94 (90–98) |
91 (83–95) |
|
Prosthesis wearers, n = 3 |
79 (74–82) |
72 (56–75) |
85 (79–87) |
|
Threshold of touch (stump), n = 30 |
r = 0.056 p = 0.768 |
r = 0.378 p = 0.039 |
r = 0.446 p = 0.014 |
|
a% method of performance: a score of 100% means that all activities were performed according to the “best” method of performance. IQR: interquartile range; r: Spearman’s rho. |
|||
Discussion
The threshold of touch of the stump circumference was significantly better than that of the stump end-point and the unaffected arm and hand after one individual with extreme sensibility measurements was excluded. These findings are in accordance with Johnson et al. (10). It is remarkable that we confirmed previous results of better threshold of touch using a more complex analysis. Reference values for threshold of touch in healthy children are not known. It would be interesting to compare our results with normative values measured in healthy children in different age categories.
A clear explanation for higher sensibility of the stump is unknown; previously, the “differential input hypothesis” has been used to explain this phenomenon (8). This hypothesis claims that the loss of a limb reduces the input into the somatosensory cortex. Neural impulses arising from stimulation of the stump enter the somatosensory cortex against a reduced background level of nervous activity compared with an undiminished level of activity on the unaffected side. As such, stimuli applied to the stump will be more readily discriminated than stimuli applied to the intact limb (8). It would be interesting to further investigate changes that occur in the somatosensory cortex of patients with ULRD in relation to stump sensibility.
Stump length contributed to sensibility differences. Distally, sensibility was lower (higher threshold of touch scores) than proximally. However, this result was the same for both arms. Our results also revealed that children with longer stumps obtained threshold of touch scores that were mostly within the normal range (< 3.22 ≈ 0.17 g, hand thresholds; Touch-test™ Sensory Evaluator Chart, 2011 North Coast Medical, Inc. (17)), therefore this difference is probably not clinically relevant. It would be interesting to compare our results with reference values for threshold of touch in healthy children. We cannot make a complete interpretation of stump length and sensibility because in our study, only the stump length of forearm deficiencies was taken into account.
Surprisingly, rudimentary fingers had significantly higher threshold of touch scores (indicating lower sensibility) than the stump circumference and the unaffected arm and hand. Nail formation on rudimentary fingers might explain this difference, since sensibility measured on nails may show reduced values, comparable to measurements on callus. A further explanation could be that rudimentary fingers are localized in an area that is used less for touching. No information in the literature could be found concerning the sensibility or the functionality of rudimentary fingers. Our observations during the stereognosis test showed that the children used rudimentary fingers to recognize shapes and textures. It is possible that rudimentary fingers play a more important role in stereognosis than in threshold of touch. As long as the role of the rudimentary fingers remains unclear, clinicians should be reluctant to recommend their removal.
It has been suggested to measure threshold of touch of the stump area that children prefer using during functional activities (10). However, we did not find differences in threshold of touch between the preferred area and the stump circumference or the corresponding area on the unaffected arm. Other sensibility modalities might play an important role (stereognosis, 2-point discrimination, vibration sense, temperature sense), which should be a topic of further research.
Stereognosis on the side of the stump was remarkably good. Recognizing shapes and textures is blocked while wearing a prosthesis, which might explain the high rate of prosthesis rejection. Stereognosis has not been investigated before in ULRD, and it might be important to take into account in future research.
Kinaesthesia, the movement sense, is a part of proprioception. It plays an important role in motor function, and is especially important in perceiving hand position and movements (27). Not only stereognosis, but also kinaesthesia, can be affected in children with cerebral palsy (28) and developmental coordination disorders (29, 30). A recent study demonstrated a relationship between minor neurological dysfunction and ULRD (14). However, we did not find differences in kinaesthesia between the affected and unaffected sides in URLD, confirming previous results (10). As such, kinaesthesia does not appear to play a different role in children with ULRD when compared with children without this condition.
Participants had very high levels of independence in activities, which is in accordance with the literature (1, 2, 31). We were probably unable to measure a correlation between sensibility and activity levels due to ceiling effects of the measurement instruments and the use of a relatively small study population. To gain more insight into this association, a larger study population comprising participants with more variability in sensibility and functioning is needed. Remarkably, sensibility was negatively correlated with the method and ease of performance scales of the PUFI items. The relationship between stump length and activity level might contribute to this finding. Further research is needed into the associations between sensibility, stump length and activity levels.
Although we did reach the number of participants needed for sufficient statistical power, the relatively small study population is a limitation of the study. A larger sample size may have given more robust results. A further limitation is that only a few children in our study population wore prostheses. As such, comparisons between prosthesis wearers and non-wearers could not be made. Furthermore, our study population consisted predominantly of individuals with forearm deficiencies, prohibiting generalization of our results to more proximal ULRDs.
Children with ULRD have significantly lower thresholds of touch (higher sensibility) of the stump circumference compared with the stump end-point and the unaffected arm and unaffected hand. Longer stumps showed higher threshold of touch (lower sensibility) than shorter stumps; however, this result may not be clinically relevant. Remarkably, children showed excellent stereognosis on the side of the stump. Rudimentary fingers were specifically used for stereognosis. Kinaesthesia was comparable between affected and unaffected sides. Children showed high levels of functionality in daily activities and, as such, no correlation between sensibility and higher activity level was found. Excellent stump sensibility may be an important finding to explain why children with ULRD function adequately without prostheses and have a high rate of prosthesis rejection.
Acknowledgements
The authors would like to acknowledge S. E. Nawijn MD from the Center for Rehabilitation “De Vogellanden”, Zwolle, for her help in patient recruitment.
Conflict of interest: The authors have no financial or personal conflicts of interest to report.
References

