Tae-Du Jung, MD1*, Ji -Young Kim, MS2*, Jee-Hye Seo, MS3, Seong-Uk Jin, MS3, Hui Joong Lee, MD4, So-Hyun Lee, MD1, Yang-Soo Lee, MD1 and Yongmin Chang, PhD4,5
From the 1Department of Physical Medicine and Rehabilitation, Kyungpook National University Hospital/Kyungpook National University School of Medicine, 2MD-PhD Program, Department of Medical Science, Kyungpook National University School of Medicine, 3Department of Medical & Biological Engineering, Kyungpook National University, 4Department of Radiology, Kyungpook National University School of Medicine and 5Department of Molecular Medicine, Kyungpook National University School of Medicine, Daegu Korea. *Both authors contributed equally to this work
OBJECTIVE: To investigate the value of combining information from resting-state functional connectivity and passive movements, measured with functional magnetic resonance imaging (fMRI), in acute stroke patients with severe motor impairment.
SUBJECTS: Eight patients with severe left upper limb motor impairment underwent a passive movement task with fMRI and resting-state fMRI, 3 weeks following stroke onset. According to the patterns of motor recovery, patients were divided into groups with, respectively, good or poor motor recovery. Patients with good recovery were further divided into two subgroups: progressive and fast late-onset motor recovery.
Method: Activation and deactivation maps from a passive movement task with fMRI were obtained. Interhemispheric connectivity analysis was conducted using resting-state fMRI.
RESULTS: Interhemispheric connectivity score in patients with progressive motor recovery was much greater than the scores in patients with fast late-onset and poor motor recovery. For passive movement, patients with progressive recovery exhibited activation in the ipsilesional sensorimotor area and no deactivation in the contralesional sensorimotor area. Patients with fast late-onset motor recovery showed strong deactivation in both sensorimotor areas. Patients with poor recovery showed no activation or deactivation in either of the sensorimotor areas.
CONCLUSION: Interhemispheric connectivity alone is not enough to predict delayed motor recovery.
Key words: stroke; motor recovery; functional magnetic resonance imaging.
J Rehabil Med 2013; 45: 546–552
Correspondence address: Yongmin Chang, Department of Molecular Medicine & Radiology, Kyungpook National University School of Medicine, 200 Dongduk-Ro Jung-Gu, Daegu. Korea. E-mail: ychang@knu.ac.kr
Accepted Feb 18, 2013; Epub ahead of print May 17, 2013
Introduction
Severe impairment in motor function is the most frequent complication after stroke (1). For appropriate rehabilitation strategies in individual stroke patients, it is important to differentiate those with the potential for motor recovery from those without such potential. To predict motor recovery after stroke, clinical examinations measuring the degree of motor impairment are the simplest indicators of prognosis. For example, the Brunnström-Fugl-Meyer motor recovery stage (BMS) is a valuable clinical outcome measurement to predict motor recovery (2, 3). In general, greater initial impairment predicts poorer functional recovery (4). However, inter-individual variability in the relationship between initial clinical outcome measurement and subsequent recovery of motor function makes accurate prognosis for each patient difficult (5). A recent study suggests that the absence of motor-evoked potential (MEP) of the affected hand 4 weeks from the onset of stroke might be an indicator of poor prognosis (6).
Based on functional magnetic resonance imaging (fMRI) studies of active and passive movements (7–11), patients with good recovery tend to exhibit a network similar to that of healthy adults. In addition, Rehme et al. (12) found that the reinstatement of effective connectivity in the contralateral (ipsilesional) hemisphere is an important feature for motor recovery after stroke. In addition, an fMRI study involving passive movement has shown the potential of the technique as an alternative paradigm to evaluate possible motor recovery, especially in patients who cannot perform voluntary movements (13). A previous study has demonstrated that a disrupted interhemispheric functional connectivity in the homologous regions around the central sulcus within the sensorimotor network is significantly related to upper extremity impairment (14).
The current study used both resting-state fMRI (rsfMRI) and a passive movement task with fMRI to investigate whether the latter technique can provide additional information on possible motor recovery in patients with severe hemiplegic stroke who are expected to show poor motor recovery based on their interhemispheric functional connectivity (FC) scores from resting-state fMRI measurement. Furthermore, contrary to previous studies of passive movement task with fMRI, we evaluated both cortical activation and deactivation patterns associated with passive hand movements. The fMRI signal decreases (deactivations) during the task period have recently become the focus of interest, because these task-related deactivations may be important for successful task performance.
CASE REPORTS
Eight patients with severe hemiplegic stroke were recruited to the study. Patients with severely impaired cognitive function (Mini-Mental State Examination (MMSE) score < 24), severe visual, or perceptual impairment, previous musculoskeletal abnormality or damage to the upper limb were excluded. Their demographic and clinical data, including sex, age and MRI findings, are summarized in Table I. All patients had experienced a right-sided ischaemic stroke in the middle cerebral arteries (MCA) region (Fig. 1a) and all were right-handed. They underwent rsfMRI and performed a passive movement task with the hemiplegic hand using fMRI at about 3 weeks post-stroke (mean 25.17 days; standard deviation (SD) 6.43 days). At that time, each patient had severe hemiplegia with no hand and finger motion. We assessed hand motor function of patients using the Brunnström-Fugl-Meyer motor recovery stage (BMS) at 3 weeks, 3 months and 6 months after stroke onset to measure prognosis of hand motor function. At 3 weeks post-stroke, BMS was one in all patients. MEP, which was performed once at 3 weeks post-stroke, could not be elicited in the abductor pollicis brevis of the left hand in the patients.
|
Table I. Patients demographic and clinical data |
|||||
|
Motor recovery patterns |
Age, years/sex |
MEP (abductor pollicis brevis) |
BMS |
BMS at 3 months post-stroke |
BMS at 6 months post-stroke |
|
Progressive recovery |
67/F |
Absent |
1 |
2 |
3 |
|
57/F |
Absent |
1 |
2 |
3 |
|
|
Fast late-onset recovery |
32/F |
Absent |
1 |
1 |
4 |
|
70/F |
Absent |
1 |
1 |
4 |
|
|
Poor recovery |
59/M |
Absent |
1 |
1 |
1 |
|
41/M |
Absent |
1 |
1 |
1 |
|
|
68/F |
Absent |
1 |
1 |
1 |
|
|
78/M |
Absent |
1 |
1 |
1 |
|
|
MEP: motor evoked potential; BMS: Brunnström-Fugl-Meyer motor recovery stage; F: female; M: male. |
|||||
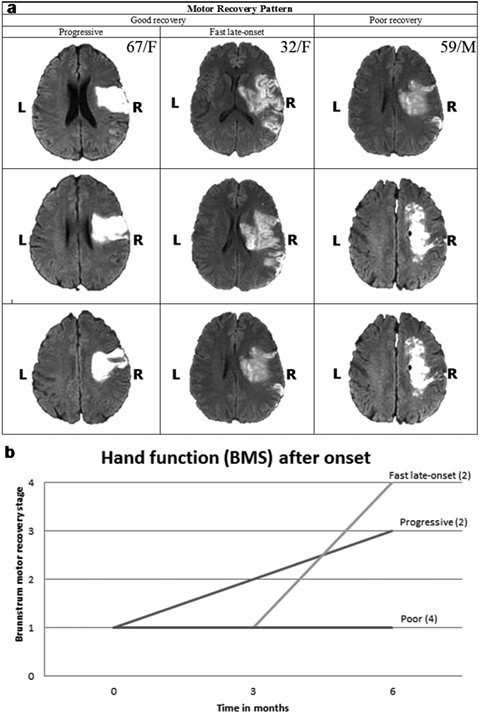
Fig. 1. (a) Representative diffusion-weighted magnetic resonance images for the stroke patients. (b) Hand function recovery patterns. Progressive recovery patients with progressive improvement of hand function at 6 months post-stroke, and patients with fast late-onset recovery with improvement of hand function at 6 months without any improvement up to 3 months after stroke.
At 6 months post-stroke, 4 patients had good hand function with BMS 3 or 4, while 4 patients still had no hand movement with BMS 1. The 4 patients who had good hand functions displayed different recovery patterns. That is, among these 4 patients, 2 showed progressive improvement in hand function from the stroke onset to 6 months, while 2 showed abrupt improvement in hand function at 6 months post-stroke without improvement at 3 months (Fig. 1b). According to the patterns of motor recovery, patients were divided into two groups, reflecting, respectively, good and poor recovery. The sensorimotor cortex was spared in all patients except one patient in poor recovery. Patients with good recovery were further divided into two subgroups: patients with progressive improvement of hand function during 6 months, and patients with abrupt improvement of hand function at 6 months without any improvement at 3 months.
All subjects signed an informed consent for the study and agreed to participate in the fMRI study. The study protocol was approved by the Institutional Review Board.
Methods
Transcranial magnetic stimulation measurement
Transcranial magnetic stimulation (TMS) was performed on the right primary motor cortex (tangential 3–4 cm lateral and posterior to Cz (the intersection of the nasion-inion line and both tragus lines) with 90-mm size round shape coil stimulator (Magstim® Rapid2, Magstim Co. Ltd, Dyfed, UK). The recording electrode was placed on the left abductor pollicis brevis (APB). The coil was held tangential to the scalp, with the handle angled backwards and 45º away from the midline. The inter-stimulus interval was 10 s. We maintained coil temperature not to exceed 35ºC. The threshold was defined as the minimum stimulation intensity required to evoke a peak-to-peak amplitude of > 50 μV in at least 5 of 10 consecutive trials. The latency and the amplitude were determined by averaging the values from 4 stimuli at 110% of threshold. The absence of an MEP was defined when we could not obtain a response after 3 successive discharges.
Magnetic resonance images acquisition
All magnetic resonance images (MRI) were acquired with a 3.0T GE HD scanner.
T1-weighted and diffusion magnetic resonance images
T1-weighted images were acquired as anatomical images using a 3D-FSPGR sequence with the following parameters: TR = 7.8 ms, TE = 3 ms, flip angle = 20, matrix = 256 × 256, FOV = 210 mm, 1.3 mm thickness, and no gap. Diffusion weighted images were obtained as confirmation of ischaemic lesion using the single-shot spin-echo, echo-planar imaging sequence with the following parameters: TR = 10,000 ms, TE = 92.3 ms, flip angle = 90°, matrix = 128 × 128, FOV = 220 mm, 4-mm thickness, and no gap. Diffusion was measured along 3 non-collinear directions with diffusion weighting (b = 1000 s/mm2) and without diffusion weighting (b = 0 s/mm2).
Resting-state functional magnetic resonance imaging
rsfMRI was performed using a gradient echo planar-imaging sequence with the following parameters: TR = 2000 ms, TE = 30 ms, flip angle = 90°, matrix = 64 × 64 and FOV = 210 mm, 4-mm thickness and no gap. During rsfMRI scans, 240 volumes were acquired and subjects had no other task but to stay alert and to keep their eyes closed during the scanning run.
Passive movement task with functional magnetic resonance imaging
The fMRI with a passive hand movement task was acquired using a gradient echo planar-imaging sequence with the following parameters: TR = 3000 ms, TE = 40 ms, flip angle = 90°, matrix = 64 × 64, FOV = 210 mm, 4-mm thickness, and no gap. An experimenter, who stood next to a patient, squeezed the left hand of the patient during the passive movement task. The passive left hand movement task began with a 30 s resting phase, followed by 30 s during which the left hand was squeezed by an experimenter. This sequence was repeated 4 times during 4 min and 80 volumes were acquired.
Analysis of task-related functional magnetic resonance imaging data
The fMRI data was analysed using the software package of Statistical Parametric Mapping 5 (SPM5) implemented in MATLAB (The Mathworks Inc., Natick, MA, USA) for imaging processing and statistical analysis. The images were corrected for slice timing effects and were realigned to the first image to adjust for residual head movement. The realigned images were spatially co-registered to the T1 image based on anatomical brain image of individual subjects and normalized into a Montreal Neurological Institute template. Subsequently, all images were smoothed with an isotropic Gaussian kernel, having 8-mm full width at the half maximum (FWHM). Low-frequency noise was removed using high-pass filter of 128 s.
Statistical analysis of the data from each subject was performed by using a general linear model approach to create the statistical map and the theory of Gaussian fields to make statistical inferences about regional effects with the SPM5. The pre-processed data were entered into first-level individual analysis by comparing brain activation during the passive motor task with brain activation during the baseline condition (passive motor task – resting baseline). The passive movement task was modelled as boxcars, of identical length to the total period of motor task prior to convolution with canonical haemodynamic response function. The explanatory variables and 6 additional regressors from the realignment procedure were used to generate a design matrix, and their corresponding regression coefficients were estimated on a voxel-wise basis by least-squares analysis. Then t-statistics were used to make statistical inferences about input of each regressor to the evaluated fMRI signal. The t-statistics created subject-specific statistical parametric maps (SPM{t}). The contrasts were applied to the parameter estimates to determine brain regions showing significant task-related signal increases and decreases associated with each of the passive motor task vs the resting baseline. Brain activations were identified as task-related signal increases during passive motor tasks, while brain deactivations were identified as task-related signal decreases during resting-phase. Significant activations and deactivations were identified at the single-subject level using threshold of uncorrected p < 0.005 and a minimum cluster extent of 32 contiguous voxels. Finally, the resulting activation maps were created to identify the anatomical correlates of the activity, and these were displayed by projection onto the individual T1-weighted images.
Interhemispheric connectivity scores
For each subject, we determined the bilateral primary motor areas (spheres of 5-mm radius) based on the motor task activation maps of individual subjects using MarsBaR (http://marsbar.sourceforge.net/), a region of interest tool. The interhemispheric connectivity (IHC) score analysis was conducted using the Functional Connectivity SPM5 toolbox (http://web.mit.edu/swg/software.htm) in the resting-state scan. To correct for co-fluctuations in blood oxygenation level dependent (BOLD) signal due to noise, BOLD signal from cerebrospinal fluid, white matter, and motion parameters were used as nuisance covariates (regressors). In addition, a band-pass filter (0.009–0.08 Hz) was used. Bivariate correlations were computed between selected regions of interest. These correlations were transformed into the β values and the functional connectivity scores using regressors and Fisher Z transforms, respectively. We represented functional connectivity maps, which correlated brain regions with ipsilesional sensorimotor area; and the IHC scores, which demonstrated functional connectivity scores of homologous sensorimotor area. The threshold value of functional connectivity map is defined in the β unit (voxels with regression coefficients > 0.65).
Statistical analysis
The IHC scores were analysed by one-way analysis of variance (ANOVA) among the 3 groups with the Statistical Package for the Social Sciences (Version 18; SPSS, Chicago, IL, USA). To assess the IHC differences between one group and another, post-hoc two sample t-tests were applied.
Results
Analysis of resting-state functional magnetic resonance imaging
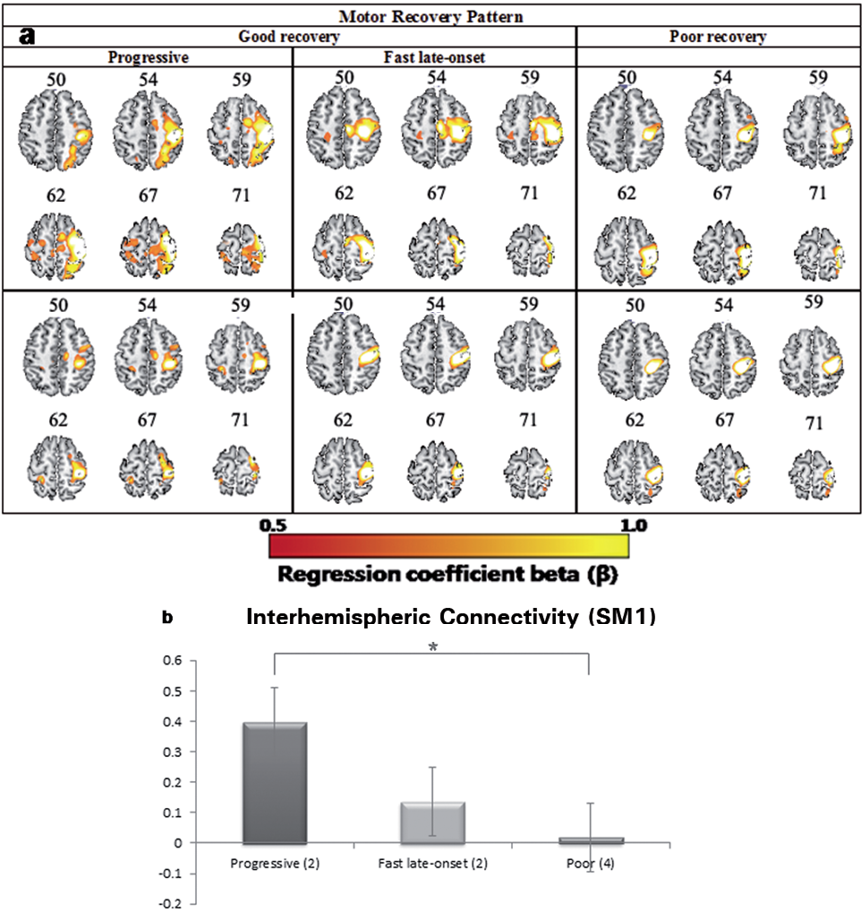
Functional connectivity maps of the cortical sensorimotor networks in stroke patients are shown in Fig. 2a. All patients displayed ipsilesional dominant functional connectivity. The groups with progressive and late-onset recovery both have SMA activation during rsfMRI as well as ipsilesional dorsal premotor activation. The mean IHC score between sensorimotor regions in patients with progressive motor recovery was much greater than the IHC scores in patients with fast late-onset recovery and in patients with poor recovery (Fig. 2b). Comparison with one-way ANOVA test showed a significant difference between the 3 groups (p < 0.05). Post-hoc comparisons with two-sample t tests indicated a significant difference between IHC scores in the progressive recovery group and the other two groups (p < 0.05). However, there was no significant difference between IHC scores in the group with fast late-onset recovery and the group with poor recovery (p = 0.538).
Fig. 2. (a) Representative resting-state functional connectivity maps of the cortical sensorimotor networks in stroke patients. (b) Mean interhemispheric connectivity score between primary sensorimotor regions in 3 recovery groups. Comparison with one-way analysis of variance test showed a significant difference between the 3 groups (p < 0.05).
Passive movement task with functional magnetic resonance imaging
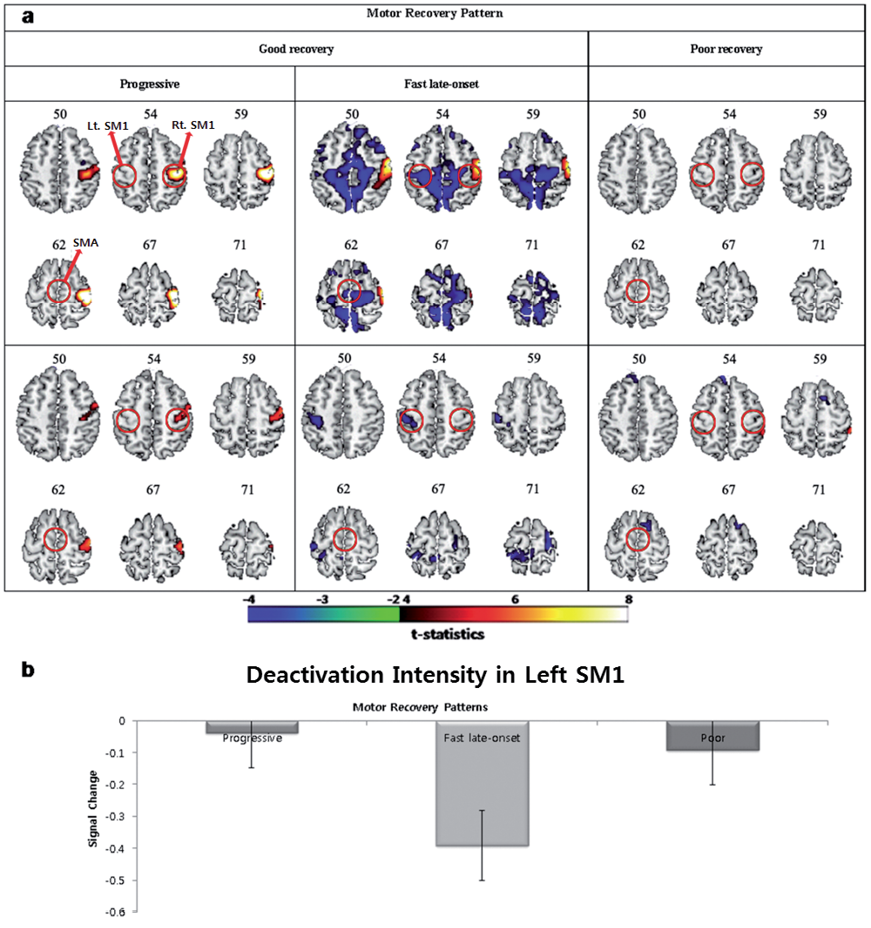
For the passive left/hemiplegic hand movement task, patients with progressive recovery exhibited positive BOLD activation in the ipsilesional sensorimotor area and no negative BOLD activity (deactivation) in the contralesional sensorimotor area (Fig. 3A). Patients with fast late-onset recovery showed positive BOLD activation in the ipsilesional sensorimotor area and exhibited deactivation in the contralesional sensorimotor areas (Fig. 3B). Patients with fast late-onset recovery also showed deactivations in SMA. In patients with poor recovery, both activation and deactivation were not observed for passive left/hemiplegic hand movements (Fig. 3C).
Fig. 3. Activation and deactivation patterns for the passive left/hemiplegic hand movement task. (a) Patients with progressive recovery, patients with fast late-onset recovery and patients with poor recovery. Red circles indicates the location of primary sensorimotor area and supplementary motor cortex. (b) Plotting mean deactivation intensities for contralesional sensorimotor area in 3 recovery groups.
Discussion
The present study is, to the best of our knowledge, the first to combine rsfMRI and a passive movement task with fMRI measurements in relation to motor recovery after stroke in patients who initially had no voluntary hand movements and no MEP of the hemiplegic hand. This study demonstrates that the combined use of rsfMRI and a passive movement task with fMRI can improve estimates of the potential for recovery of motor function in stroke patients. In particular, the deactivation pattern of the passive movement task with fMRI is important to estimate possible long-term motor recovery.
The rsfMRI data showed that the mean IHC scores between ipsilesional and contralesional motor regions were significantly higher in patients with progressive recovery than in patients with poor recovery. This finding was consistent with a previous observation that disruption of IHC scores between sensorimotor regions significantly correlated with upper extremity impairment (14). However, the current findings from IHC analysis also revealed that IHC alone is insufficient to predict delayed motor recovery shown in patients with fast late-onset recovery. That is, based on IHC scores at the time of rsfMRI examination (3 weeks after stroke onset), patients with fast late-onset recovery would be regarded as those who had less potential for motor recovery and were expected to show poor recovery. The present findings from the IHC analyses therefore suggest that, although the spontaneous activities in the motor network at rest would have a good prognostic value, it is necessary to measure the movement-related cortical activities in the motor network for better estimates of the potential capacities for motor recovery in stroke patients.
While passive movement is a form of sensory stimulation, provided by proprioceptive input, a previous study used passive movement to demonstrate that it can be useful in assessment of physiological changes associated with motor recovery after stroke, when patients show little mobility (15). More specifically, Matteis et al. (15) demonstrated that the increase in mean flow velocity in the MCA of the affected hemisphere is higher than in the MCA of the unaffected hemisphere during passive elbow movements in patients with good recovery, while there is only a slight bilateral increase in mean flow velocity with prevalence for the MCA in the unaffected hemisphere in patients with poor recovery. Although active and passive tasks are quite different, studies that used passive movement and active motor tasks also found largely overlapping patterns of activation (9, 13, 16). Thus, passive movement paradigms seem to be a suitable way to investigate the functionality of the sensorimotor network recruited during active movements, particularly in patients with severe impairment. However, our passive movement task with fMRI data revealed that patients with progressive recovery were not differentiated from patients with fast late-onset recovery, because both groups showed ipsilesional sensorimotor activation. Furthermore, a previous observation demonstrated that the ipsilesional sensorimotor activation, occurring/generated during passive movements of the affected hand in the early stage of stroke, had a low predictive value for the motor recovery of the hemiplegic hand (9).
Interestingly, however, patients with fast late-onset recovery showed significant deactivation in the contralesional sensorimotor area and SMA, while both progressive and poor recovery patients showed no deactivation in both ipsilesional and contralesional sensorimotor area for passive movement of the affected hand. The underlying physiological mechanism of the widespread deactivation in the patients with fast late-onset recovery remains unclear. However, a previous study demonstrated that the increased neuronal activation of the motor cortex in one hemisphere might induce reduced neuronal activity in the opposite hemisphere (17). Based on this previous observation, a possible interpretation for widespread deactivation in the contralesional sensorimotor area and SMA is that these brain areas reduce their neuronal activity in order to increase neuronal activation of sensorimotor area in the ipsilesional hemisphere. That is, strong deactivation patterns shown in patients with fast late-onset recovery might suggest that, although activation in the sensorimotor area was not involved during early recovery processes, the deactivation pattern might be a predictive factor for possible functional recovery of the affected hand at the late stage. Another possible explanation is “diaschisis” or “distributed injury hypothesis”, in which focal structural lesions lead to dysfunction in brain regions that are structurally intact, but connected to the area of structural damage (18, 19). Our IHC analysis revealed remote network dysfunction after a focal lesion in the motor network, suggesting that widespread alterations in motor network functional connectivity take place, while stroke induces a sudden local structural lesion. In terms of “diaschisis” or “distributed injury hypothesis”, our findings from IHC analysis seem to reflect the degree of dysfunction in remote brain regions that are structurally intact and thus, in part, reflect the potential capacity for motor recovery.
This study has some limitations. First, a small number of patients in the hospital were recruited. Secondly, we did not evaluate the longitudinal changes in activation and deactivation fMRI patterns during motor recovery after stroke. In particular, since there were no fMRI data 6 months after onset of stroke, we could not compare brain activation patterns between patients with fast late-onset recovery and those with progressive recovery at 6 months after stroke, in which both groups showed significant motor recovery. Thirdly, the results were reported at uncorrected p < 0.005 level, and thus we could not exclude a chance of type 1 error (a false-positive error). Finally, in the current study, we used a hand squeezing procedure performed by another person. This was not an automatized procedure for moving the upper limb passively, and thus there might be a difference in activation patterns due to inconsistency in the squeezing procedure.
In summary, this study demonstrates that the combined use of rsfMRI and a passive movement task with fMRI may be important to evaluate the potential recovery of motor function in stroke patients. The rsfMRI data show that IHC scores between homologous motor regions are a good indicator for progressive upper limb motor recovery after stroke, but that IHC alone is not enough to predict delayed motor recovery shown in patients with fast late-onset recovery. In patients with fast late-onset recovery, the strong deactivation of passive movement task with fMRI in the sensorimotor system, including contralesional sensorimotor area, is an indicator of possible delayed motor recovery.
AcknowledgementS
This work was supported by a grant from the Ministry of Health & Welfare (A092106) of Korea, and by Kyungpook National University Research Fund, 2013.
References

