Yngve Roe, MSc1,3, Erik Bautz-Holter, PhD2,3, Niels Gunnar Juel, MSc2 and Helene Lundgaard Soberg, PhD1,2
From the 1Faculty of Health Sciences, Oslo and Akershus University College of Applied Sciences, 2Department of Physical Medicine and Rehabilitation, Oslo University Hospital Ulleval and 3Faculty of Medicine, University of Oslo, Oslo, Norway
OBJECTIVE: To identify the most common problems in patients with shoulder pain, using the International Classification of Functioning, Disability and Health (ICF) as a reference.
DESIGN: A cross-sectional study.
SUBJECTS: Outpatients at a hospital with shoulder pain lasting longer than 3 months.
METHODS: Patients were interviewed with an extended version of the ICF Checklist version 2.1a. Patients’ problems in functioning, and the magnitude of the problem, were registered separately for each category. Categories identified as a problem in at least 5% of patients were reported. To describe the population, age, diagnosis, work participation and the Shoulder Pain and Disability Index (SPADI) were recorded.
RESULTS: A total of 165 patients with a mean age of 46.5 years (standard deviation 12.5) and a SPADI score of 47.4 (standard deviation 21.1) were included. Of the participants, 92.8% were either employed or students, 35.2% of whom were on sick leave. The primary result was the identification of 61 condition-specific second-level ICF categories: 19 in the body functions and structures component, 34 in activities and participation, and 8 in environmental factors.
CONCLUSION: The findings provide a comprehensive picture from the patient-perspective of the disability associated with shoulder pain. The findings may enhance multidisciplinary communication in clinical settings.
Key words: ICF; outcome assessment (health care); shoulder pain; cross-sectional studies, disability evaluation; World Health Organization; recovery of function; rehabilitation/cl [classification]; rehabilitation.
J Rehabil Med 2013; 45: 00–00
Correspondence address: Yngve Roe, Faculty of Health Sciences, Oslo and Akershus University College of Applied Sciences, Postboks 4 St Olavs plass, NO-0130 Oslo, Norway. E-mail: yngve.roe@hioa.no
Accepted Feb 7, 2013; Epub ahead of print Maj 17, 2013
Introduction
Shoulder pain is a common condition, with an estimated prevalence of between 7% and 26% (1). In a Norwegian middle-aged population cohort, pain in the neck or shoulder during the previous month was the most common health complaint, and almost three-quarters reported work-related pain (2). Many cases of shoulder pain are persistent or recurrent, and shoulder pain is a common cause of work absenteeism (3, 4).
The disability associated with shoulder pain has traditionally been explained by deficits in muscular and movement-related functions (5, 6). Findings from more recent research, however, indicate that the condition may also have an impact on mental function and general health (7–12). Moreover, physical and social factors in the work environment have been found to influence functioning (13–16). Although previous research provides a valuable contribution to the understanding of the impact of shoulder pain on functioning, it has often been limited to defined patients groups, rehabilitation settings or specific aspects of functioning. A number of different classifications are in use, and no multidisciplinary clinical practice guidelines exist (17–19).
As a result of the approval of the International Classification of Functioning, Disability and Health (ICF) in 2001, a system of concepts and a classification of functioning became available (20). The ICF provides a hierarchical classification system based on components, chapters and categories. The body functions and structures component is ordered according to body regions or systems, and the activities and participation component covers the complete range of domains, denoting aspects of functioning from both an individual and a societal perspective (20). The environmental factors component is systematically arranged in sequence from the individual’s most immediate environment to the general environment and may affect all functional components (20). Personal factors are not classified in the ICF because of their wide social and cultural variance (20). The ICF describes situations with regard to human functioning, and serves as a framework to organize information (20).
The ICF classification is comprehensive, as it comprises more than 1,400 categories. To increase its applicability in clinical assessments and research, ICF Core Sets have been developed. The Core Sets contain a selection of categories that describe the typical spectrum of problems in functioning of patients with specific conditions (21). The development processes were based on literature reviews, expert surveys and quantitative and qualitative clinical studies of patients (21). Currently, ICF Core Sets for a number of chronic conditions and settings are available, e.g. low back pain and vocational rehabilitation (22, 23). As part of the development process, patients’ problems in functioning were investigated in cross-sectional studies (24, 25). Until now, shoulder pain has rarely been investigated within the bio-psycho-social perspective, and to our knowledge, there are no condition-specific ICF categories for shoulder pain.
The aim of this study was to identify the ICF categories that best describe problems related to functioning and interactions with the environment due to shoulder pain from the patient’s perspective.
Methods
Study design
This study had a cross-sectional design and included outpatients with shoulder pain at the Department of Physical Medicine and Rehabilitation at Oslo University Hospital from November 2009 through February 2011. The study was approved by the Norwegian Regional Ethical Committee (number 2009/820a) and was conducted according to the Declaration of Helsinki.
Subjects
Patients aged 18 years and older, diagnosed with shoulder pain and symptoms lasting longer than 3 months, were eligible for the study. The exclusion criteria were shoulder joint replacement, surgery in the affected shoulder within the last 6 months, diagnosed rheumatic disease affecting the shoulder, generalized pain conditions, and insufficient Norwegian language skills.
Measures
Data were collected with two sets of case record forms, one for health professionals and another for patients. The case record form for health professionals included registrations of the patients’ characteristics and the nature of the patients’ work with regard to repetitive movements of the arm, use of the arm at or above shoulder level, and lifting 10 kg or more at work.
An extended ICF Checklist was derived for the patients from the ICF classification. The categories in the ICF classification use an alphanumeric coding system, in which the first letter refers to the component, followed by a numeric code that starts with the chapter number (e.g. d4 mobility), followed by the second-level category (e.g. d445 hand and arm use), the third-level category (e.g. d4452 reaching) and the fourth-level category, when appropriate.
The ICF Checklist in the current study was an extended version of the generic ICF Checklist Version 2.1a (26). The content of the condition-specific scales and clinical tests were extracted and linked to ICF categories by a researcher (Y.R.) to ensure that all relevant functions were covered (27, 28). Twenty-three additional second-level categories from these measures were added to the generic checklist. The final Extended ICF Checklist contained a total of 146 second-level ICF categories. Of these, 52 were from the body functions and structures component, 57 were from the activities and participation component and 37 were from the environmental factors component. The patients’ problems in each category were rated on an ordinal scale, with scores ranging from 0 to 4 (20). For the body functions components, the scores included no impairment, mild impairment, moderate impairment, severe impairment and complete impairment. For the body structures component, only the presence of impairment was rated, as either impairment or no impairment, in this study. In the activities and participation component, the categories were denominated no difficulty, mild difficulty, moderate difficulty, severe difficulty and complete difficulty and were rated according to reported performance. The environmental factors component included both barriers and facilitators of function, each categorized as mild, moderate, severe or complete. Additional options on the ICF qualifiers scale were 8 (not specified), 9 (not applicable) and C (comorbidity). The not specified option was avoided, and not applicable was registered only for mutually exclusive categories in the major life areas (d8-chapter). Comorbidity was registered on a separate form.
The case record form for patients contained both the Shoulder Pain and Disability Index (SPADI) and the Self-Administered Comorbidity Questionnaire (SCQ). The SPADI is a patient-reported condition-specific instrument comprising 13 items in the pain and disability domains (29, 30). Ratings are registered on an 11-point ordinal scale, from no pain/no difficulty (0) to worst pain imaginable/so difficult it required help (10). A summed score ranging from 0 to 100 (best to worst) is estimated by averaging the pain and disability sub-scores. The SCQ is a patient-rated instrument with a list of common health problems to which an additional question on neck pain was added (31). The respondent was asked to mark whether the health problem was present, whether treatment had been received and whether the problem limited activities.
Procedure
The outpatient clinic of the Department of Physical Medicine and Rehabilitation at Oslo University Hospital receives patients with musculoskeletal conditions who are referred from general practitioners. The patients undergo an assessment by a physician specializing in physical medicine. Based on standardized criteria, a diagnosis according to the International Classification of Diseases (ICD-10) is made and further interventions are recommended (32, 33).
The inclusion of the patients shown in Fig. 1 was based on the contributions of 7 physicians at the clinic. The clinic receives approximately 750 patients with shoulder pain annually (personal communication NGJ). Patients with an appointment on specific weekdays when the researcher (YR) would be present received a letter informing them about the study, and notifying them that they would be asked to participate after the consultation if they met the inclusion criteria. Overall, 375 patients received information about the study, and 165 (44%) patients were included. The distribution of gender and diagnoses of the included patients were in accordance with the general cohort of patients with shoulder pain at the clinic.
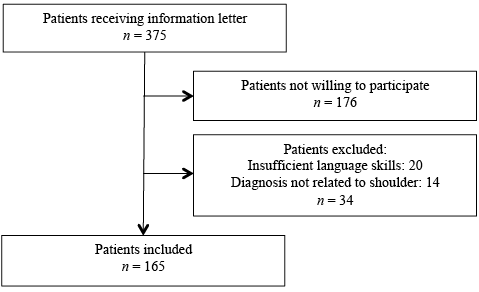
Fig. 1. Inclusion procedure.
The included patients participated in a structured interview using the case record form for health professionals and completed the case record form for patients. The interviews were administered by a physiotherapist and researcher (YR) who has experience with the ICF and with shoulder rehabilitation in clinical and educational settings. The ratings of the severity of functional problems in the Extended ICF Checklist were determined through discussion with the patient. When categories were not self-explanatory, examples from the inclusions of the ICF were provided. For example, the second-level category of emotional functions (b152) was exemplified by joy, sorrow, tension, fear, anger, etc. The ratings of structural impairment were based on the standardized diagnostic criteria (32, 33). The mean duration was approximately 40 min for the interviews and 20 min for the questionnaires.
Statistical analysis
Descriptive statistics are used to characterize the study population. Gender, educational level, employment status, primary ICD-10 diagnosis of the shoulder, comorbidity and the nature of the work were estimated as relative frequencies (%). Age and the SPADI total summary score were estimated with the mean and the standard deviation (SD).
The relative frequencies (%) of ICF categories that registered as impairment, limitation, restriction, barrier or facilitator for at least 5% of the participants were reported for each ICF component separately.
IBM SPSS Statistics, version 19 was used for the statistical analysis (IBM Corporation, Armonk, NY, USA).
Results
The characteristics of the included patients and their comorbidities are shown in Table I. There was a slight overrepresentation of women (54%). The diagnosis impingement syndrome (m75.4) was the most frequent, accounting for 43% of the cases. Additional neck pain was reported by almost two-thirds of the patients and low back pain was reported by more than one-third of the patients.
|
Table I. Characteristics of the patient population (n = 165) |
|
|
Characteristics |
|
|
Gender, male, % |
46 |
|
Age, years, mean (SD) [range] |
46.5 (12.5) [19–86] |
|
Education, % |
|
|
≤ 12 years in school |
56 |
|
University/college |
44 |
|
Employment status, % |
|
|
Remuneratively employed |
76.3 |
|
Student in higher education |
16.5 |
|
Other |
7.2 |
|
Duration of pain, % |
|
|
3–6 months |
15 |
|
6–12 months |
26 |
|
> 12 months |
59 |
|
Main ICD-10 diagnoses of the shoulder, % |
|
|
m75.4 Impingement syndromea |
42.9 |
|
m79.1 Myalgia |
18.0 |
|
m75.0 Adhesive capsulitis |
13.7 |
|
m24.3 Instability |
5.5 |
|
m75.1 Rotator cuff syndromeb |
5.0 |
|
m19.8 Acromioclavicular-joint rupture or arthrosis |
3.8 |
|
Other diagnoses |
11.1 |
|
Comorbidityc, % |
|
|
Neck pain |
66 |
|
Back pain |
35 |
|
Osteoarthritis (other than in shoulder) |
14 |
|
Depression |
12 |
|
Rheumatoid arthritis |
4 |
|
Other medical conditions |
37 |
|
SPADI total score, mean (SD) |
47.4 (21.1) |
|
aInclusive bursitis and partial thickness tears. bOnly full thickness tears. cMore than one comorbidity was registered in some participants. SD: standard deviation; SPADI: Shoulder Pain and Disability Index; ICD-10: International Classification of Diseases – version 10. |
|
With regard to employment status, 92.8% of the participants were either employed or students, 35.2% of whom were on sick leave. The remainder of the participants (7.2%) were retired, unemployed, received disability pension or were homemakers. The nature of the work varied; 82% reported repetitive movements of the arm, 29% reported frequent use of the arm at or above shoulder level, and 27% reported frequent lifting of 10 kg or more at work.
The 19 second-level ICF categories that were identified as a problem in the body functions and structures component are shown in descending order in Table II. The most frequent problems were related to the sensation of pain (b280), mobility of joint functions (b710), sleep (b134), muscle endurance functions (b740) and energy and drive functions (b130).
|
Table II. International Classification of Functioning, Disability and Health (ICF) categories of the body functions and structures component with relative frequencies (%), rated as impaired in at least 5% of participants |
||||||
|
Body functions and structures categories |
0 |
1 |
2 |
3 |
4 |
Sum 1–4 |
|
b280 Sensation of pain |
1.2 |
13.9 |
34.5 |
43.6 |
6.7 |
98.8 |
|
s720 Structure of shoulder region |
4.2 |
– |
– |
– |
– |
95.8 |
|
b710 Mobility of joint functions |
9.1 |
18.2 |
20.6 |
45.5 |
6.7 |
90.9 |
|
b134 Sleep functions |
21.2 |
20.6 |
23.0 |
30.9 |
4.2 |
78.8 |
|
b740 Muscle endurance functions |
26.1 |
15.8 |
23.0 |
32.1 |
3.0 |
73.9 |
|
b130 Energy and drive functions |
29.7 |
22.4 |
27.9 |
18.8 |
1.2 |
70.3 |
|
b730 Muscle power functions |
30.9 |
13.3 |
24.2 |
29.7 |
1.8 |
69.1 |
|
b720 Mobility of bones function |
32.1 |
24.8 |
21.8 |
21.2 |
0 |
67.9 |
|
b840 Sensation related to the skin |
36.4 |
24.2 |
20.6 |
18.2 |
0.6 |
63.6 |
|
b735 Muscle tone functions |
40.6 |
18.2 |
21.8 |
18.8 |
0.6 |
59.4 |
|
b126 Temperament and personality functions |
48.5 |
26.1 |
20.6 |
4.8 |
0 |
51.5 |
|
b152 Emotional functions |
53.9 |
24.2 |
14.5 |
7.3 |
0 |
46.1 |
|
s730 Structure of upper extremity |
56.6 |
– |
– |
– |
– |
43.6 |
|
b715 Stability of joint functions |
70.3 |
13.9 |
6.7 |
9.1 |
0 |
29.7 |
|
s710 Structure of head and neck region |
82.4 |
– |
– |
– |
– |
17.6 |
|
b140 Attention functions |
89.7 |
4.8 |
4.2 |
1.2 |
0 |
10.3 |
|
b144 Memory functions |
90.3 |
7.9 |
1.2 |
0.6 |
0 |
9.7 |
|
b770 Gait pattern functions |
92.7 |
4.8 |
1.8 |
0.6 |
0 |
7.3 |
|
b164 Higher level cognitive functions |
93.9 |
4.8 |
1.2 |
0 |
0 |
6.1 |
With respect to problems in the activities and participation 33 second-level ICF categories that were identified as a problem are shown in descending order in Table III. The most frequent problems were related to lifting and carrying objects (d430), remunerative employment (d850), recreation and leisure (d920) and changing basic body positions (d410). Of the 10 patients who were students, 6 reported difficulties in the higher education category (d830) (not shown in Table III).
|
Table III. International Classification of Functioning, Disability and Health (ICF) categories of the activities and participation component with relative frequencies (%), rated as a limited or restricted in at least 5% of participants |
||||||
|
Activities and participation categories |
0 |
1 |
2 |
3 |
4 |
Sum 1–4 |
|
d430 Lifting and carrying objects |
15.2 |
26.7 |
26.1 |
28.5 |
3.6 |
84.8 |
|
d850 Remunerative employment |
21.2 |
20.0 |
18.2 |
21.2 |
19.4 |
78.8 |
|
d920 Recreation and leisure |
23.6 |
18.2 |
27.3 |
25.5 |
5.5 |
76.4 |
|
d410 Changing basic body position |
24.8 |
20.6 |
24.8 |
26.7 |
3.0 |
75.2 |
|
d510 Washing oneself |
30.9 |
25.5 |
29.7 |
13.3 |
0.6 |
69.1 |
|
d540 Dressing |
33.3 |
26.7 |
27.3 |
12.1 |
0.6 |
66.7 |
|
d415 Maintaining a body position |
37.0 |
16.4 |
22.4 |
23.6 |
0.6 |
63.0 |
|
d640 Doing housework |
40.0 |
23.0 |
23.0 |
12.7 |
1.2 |
60.0 |
|
d620 Acquisition of goods and services |
48.5 |
26.7 |
18.8 |
6.1 |
0 |
51.5 |
|
d475 Driving |
62.4 |
15.8 |
12.1 |
8.5 |
1.2 |
37.6 |
|
d445 Hand and arm use |
66.1 |
17.6 |
13.3 |
2.4 |
0.6 |
33.9 |
|
d520 Caring for body parts |
70.3 |
16.4 |
9.1 |
4.2 |
0 |
29.7 |
|
d630 Preparing meals |
72.7 |
14.5 |
10.3 |
1.8 |
0.6 |
27.3 |
|
d465 Moving around using equipment |
73.9 |
15.8 |
6.7 |
3.0 |
0.6 |
26.1 |
|
d440 Fine hand use |
76.4 |
10.3 |
7.3 |
6.1 |
0 |
23.6 |
|
d770 Intimate relationships |
81.2 |
10.9 |
6.1 |
1.8 |
0 |
18.8 |
|
d530 Toileting |
81.8 |
7.9 |
8.5 |
1.8 |
0 |
18.2 |
|
d660 Assisting others |
84.2 |
10.9 |
3.6 |
1.2 |
0 |
15.8 |
|
d550 Eating |
86.1 |
11.5 |
2.4 |
0 |
0 |
13.9 |
|
d760 Family relationships |
86.1 |
8.5 |
4.8 |
0.6 |
0 |
13.9 |
|
d455 Moving around |
86.7 |
7.9 |
3.0 |
1.8 |
0.6 |
13.3 |
|
d750 Informal social relationships |
86.7 |
9.1 |
1.8 |
2.4 |
0 |
13.3 |
|
d740 Formal relationships |
89.7 |
7.3 |
2.4 |
0.6 |
0 |
10.3 |
|
d230 Carrying out daily routine |
90.9 |
2.4 |
4.2 |
2.4 |
0 |
9.1 |
|
d170 Writing |
91.5 |
2.4 |
2.4 |
3.6 |
0 |
8.5 |
|
d650 Caring for household objects |
92.1 |
5.5 |
2.4 |
0 |
0 |
7.9 |
|
d710 Basic interpersonal interactions |
92.1 |
5.5 |
1.8 |
0.6 |
0 |
7.9 |
|
d720 Complex interpersonal interactions |
92.1 |
4.8 |
1.8 |
1.2 |
0 |
7.9 |
|
d420 Transferring oneself |
93.3 |
4.8 |
1.2 |
0.6 |
0 |
6.7 |
|
d210 Undertaking a single task |
93.9 |
1.8 |
3.0 |
1.2 |
0 |
6.1 |
|
d730 Relating with strangers |
93.9 |
4.8 |
0.6 |
0.6 |
0 |
6.1 |
|
d220 Undertaking multiple tasks |
94.5 |
1.8 |
2.4 |
1.2 |
0 |
5.5 |
|
d470 Using transportation |
94.5 |
2.4 |
3.0 |
0 |
0 |
5.5 |
|
The higher education (d830) category was limited or restricted in 6 out of 10 of the patients registered as students. |
||||||
The 8 second-level ICF categories of the environmental factors component identified as a barrier or facilitator are shown in descending order in Table IV. No categories exceeded a frequency of 20%. Immediate family and friends (e310 and e320) were the most frequently reported facilitators, while social security services, systems and policies (e570) was the most frequently reported barrier.
|
Table IV. International Classification of Functioning, Disability and Health (ICF) categories of the environmental factors component with relative frequencies (%), rated as a barrier or facilitator in at least 5% of participants |
||||||||||||
|
Environmental factors categories |
Barrier |
Facilitator |
||||||||||
|
0 |
–1 |
–2 |
–3 |
–4 |
Sum (1–4) |
1 |
2 |
3 |
4 |
Sum (1–4) |
||
|
e310 Immediate family |
80.6 |
0.6 |
0.6 |
0 |
0 |
1.2 |
6.7 |
10.3 |
1.2 |
0 |
18.2 |
|
|
e320 Friends |
86.0 |
0 |
0 |
0 |
0 |
0 |
6.1 |
7.3 |
0.6 |
0 |
14.0 |
|
|
e570 Social security services, systems and policies |
86.2 |
1.8 |
4.2 |
4.2 |
0 |
10.2 |
1.8 |
1.2 |
0.6 |
0 |
3.6 |
|
|
e125 Products and technology for communication |
85.5 |
1.2 |
6.7 |
0.6 |
0 |
8.5 |
0.6 |
4.8 |
0.6 |
0 |
6.0 |
|
|
e325 Acquaintances, peers, colleagues, neighbours and community members |
86.8 |
0.6 |
4.2 |
0.6 |
0 |
5.4 |
4.2 |
3.6 |
0 |
0 |
7.8 |
|
|
e330 People in positions of authority |
88.6 |
0.6 |
3.0 |
1.2 |
0 |
4.8 |
3.6 |
3.0 |
0 |
0 |
6.6 |
|
|
e355 Health professionals |
91.6 |
1.2 |
1.8 |
0 |
0 |
3.0 |
2.4 |
3.0 |
0 |
0 |
5.4 |
|
|
e450 Individual attitudes of health professionals |
91.0 |
1.2 |
3.0 |
1.2 |
0 |
5.4 |
1.2 |
2.4 |
0 |
0 |
3.6 |
|
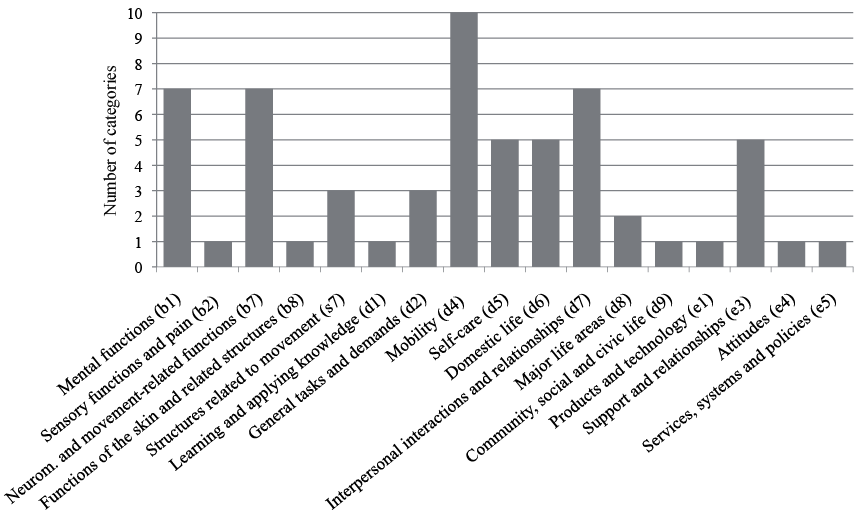
The distribution of categories according to ICF chapter-level in Fig. 2 shows that the highest number of categories were identified in the chapters of mobility (d4), with 10 categories, followed by the neuromusculoskeletal and movement-related functions (b7), mental functions (b1) and interpersonal interactions and relationships (d7) chapters, with seven categories each, and self-care (d5), domestic life (d6) and support and relationships (e3), comprising 5 categories each.
Fig. 2. Overview of International Classification of Functioning, Disability and Health (ICF) chapters containing one or more second-level categories identified as a frequent problem, barrier or facilitator (n = 61).
Discussion
The primary result of this study was the identification of a set of 61 second-level ICF categories reflecting common problems in functioning and environmental factors in chronic shoulder pain from the patients’ perspective.
The characteristics of the patients show that patients in the current study had a distribution of gender, age and diagnoses that paralleled a sample of patients in a general practice reported by van der Windt and colleagues (4). The mean SPADI-total score did not deviate substantially from the scores reported by Beaton and colleagues in a hospital-treated sample of patients with shoulder-related diagnoses, or from a study by Ostor and colleagues on patients in primary care (34, 35).
Problems in functioning that related to a total of 19 categories in the body functions and structures component are shown in Table II. The sensation of pain (b280) was a problem for almost all of the patients, and more than half of the patients rated their pain as severe or complete. The frequency estimate and severity ratings show that pain itself is a major issue in the understanding of shoulder pain. Pain has also been found to be an almost equally prevalent problem in other musculoskeletal disorders, such as low back pain (24).
Furthermore, 7 categories related to problems of neuromusculoskeletal and movement-related functions (b7) were identified. Of these, the most frequently reported problems were in the mobility of joint functions (b710), muscle endurance functions (b740), muscle power functions (b730) and mobility of bone functions (b720). Most of these categories reflect functions that are considered key elements in the clinical examination of shoulder pain (6, 36). The findings of the current study thus show that patients have perceptions of aspects of functioning that traditionally have been assessed by clinicians. However, one of the frequent functions, muscle endurance, has received less attention in the clinical literature. Brox and colleagues (37) found that isometric muscle endurance was associated with both emotional distress and increased pain in a group of patients with rotator cuff tendinosis, and they recommended muscle endurance testing as a psychophysiological measure in assessments. The findings indicate that patients have perceptions of aspects of functioning that are often assessed by clinicians, and future research should investigate the benefits of the improved participation of patients in the examinations.
Three categories were identified within the body structures component, of which the structure of shoulder region (s720) was the most frequently reported. The registrations were made according to the evidence-based diagnostic criteria of symptom localization and imaging used in the department (32, 33). Almost two-thirds of the patients reported additional neck pain, and more than one-third reported additional low back pain. Others have shown that additional pain or symptom sites may be predictive for patients’ disability. Cunningham and colleagues (38) suggested that persons with multiple pain sites were more likely to report disability, while Kamaleri and colleagues (39)found an almost linear relationship between the number of pain sites and overall health, sleep quality, and psychological health. Whether pain in the neck should be considered a comorbidity is, however, a matter of definition, which has been handled differently in different studies. However, we believe that only a few patients in the current study may be characterized as having multiple pain sites because generalized pain was an exclusion criterion.
In the area of mental functions (b1-chapter), problems related to 7 categories were identified. More than half of the participants had problems with sleep (b134), energy and drive functions (b130) and temperament and personality functions (b126). However, only 12% of the patients in the current study reported depression on the comorbidity form. Psychological factors have been found to be important in understanding the development or maintenance of shoulder pain (7, 11, 12). Van der Windt and colleagues (40) found that these factors were more strongly associated with persistent pain and disability in patients with low back pain than in those with shoulder pain, and they suggested that the influence of psychological factors on outcome varies across patients with different types of pain. By contrast, difficulties with mental function in the current study were found with somewhat higher frequencies than for the patients with low back pain in the cross-sectional study by Ewert and colleagues (24). Until now, how problems in mental functioning should influence clinical decision-making has been little discussed.
With regard to problems in activities and participation, a total of 33 categories were identified. Related to mobility (d4-chapter), problems in lifting and carrying objects (d430) and changing or maintaining a body position (d410 and d415) were the most commonly reported. When comparing the d4 mobility chapter findings with the other musculoskeletal cross-sectional studies, lifting and carrying appeared to be a functional problem that was very frequent in all conditions (24). Unlike shoulder pain, problems walking were also frequent among the other musculoskeletal conditions.
Activities of daily living were also affected. With respect to the self-care (d5) and domestic life (d6), problems in washing oneself (d510), dressing (d540), doing housework (d640) and acquisition of goods and services (d620) were the most frequent. Functioning according to self-care and domestic life has been considered important and are thus often implemented in the items of condition-specific scales (8, 10, 41). By contrast, for low back pain, no frequent functions related to self-care, and only 1 related to domestic life, were identified in the cross-sectional study (24). Nevertheless, the self-care and domestic life functions were added during the development of the ICF Core Set for low back pain, and these functions are also present in the other musculoskeletal Core Sets (22, 42).
Although problems in social participation were reported by less than 20% of the patients, 7 functions of interpersonal interactions and relationships (d7-chapter) were identified. These primarily concerned intimate relationships (d770), family relationships (d760) and informal social relationships (d750), and indicate that for some patients their shoulder pain has consequences for their social life. In an overview of psychosocial and behavioural factors in shoulder and neck pain, Linton (11) suggested that a better understanding of these factors might enhance the treatment and prevention of the condition. An almost equal number of low frequent functional problems in the interpersonal interactions and relationships (d7-chapter) were found among the other musculoskeletal conditions (24), and problems in intimate relationships (d770) were found to represent a common problem in all musculoskeletal ICF Core Sets (42).
A large majority of the working patients reported problems with remunerative employment (d850), and 6 of 10 of the students reported problems with higher education (d830). These findings are in line with previous findings of a negative relationship between shoulder pain and work (2, 3). Moreover, the high frequency of problems in remunerative employment was parallel to the other cross-sectional study on musculoskeletal conditions (24). In a recent cross-sectional study on patients in vocational rehabilitation, 40 activities and participation functions were identified as a problem, a substantially higher number than in the other studies (25). The finding from vocational rehabilitation shows that problems related to work performance are complex, and thus need to be classified by a range of ICF categories of the component.
Problems in recreation and leisure (d920) were reported by more than two-thirds of the patients. This category covers sports, playing, and engaging in handicrafts, hobbies and gatherings with others. However, we did not register whether the problems were related to sports or other recreational activities. Participation in sports is known to be affected in patients with shoulder pain (43). Problems in recreation and leisure were also reported by patients with low back pain and also found in all 5 condition-specific ICF Core Sets for musculoskeletal conditions (24, 42).
Eight environmental factors were identified as facilitators or barriers to functioning in the current study. Five of the 8 categories were in support and relationships (e3-chapter) and were primarily reported as facilitators. The findings of relevant environmental factors in the current study indicate that social factors may positively contribute to functioning for patients with shoulder pain. Although environmental factors have generally received little attention in shoulder pain research, there is some evidence to support the current findings (14–16). The cross-sectional study on musculoskeletal conditions also found few and low frequency categories according to the component (24). However, a number of categories of environmental factors were identified in other elements of the ICF Core Set development process for these conditions, indicating that structured interviews with limited time frames may not be the most adequate method to identify these factors (22, 24, 42).
The ICF chapters registered with the highest number of functional problems are shown in Fig. 2. The finding illustrates the complexity of the disability associated with chronic shoulder pain, and underscores the need to address a number of different functional domains in clinical decision-making (41).
The strength of this study is that it provides, for the first time, a comprehensive overview of functioning in shoulder pain within the ICF framework. However, this study has some limitations that should be considered. First, some condition-specific categories of interest may have been missed due to the development procedure of the Extended Checklist. For example, the handling stress and other psychological demands (d240) category occurred frequently in the vocational rehabilitation study, but it was not found in the measures used to extend the checklist in the current study (25). Secondly, few elderly patients and patients with rheumatic disorders were included in the current study, even though shoulder pain may be common in such patients (44, 45). The results may thus not be generalized to these patient groups. Thirdly, this study was conducted with a cohort referred to a university hospital. Therefore, the patients may not be representative of the general population of shoulder pain patients seen by general practitioners.
In conclusion, this study provides the first comprehensive overview of disability in shoulder pain from the perspective of patients, using the ICF as a reference. A set of 61 second-level ICF categories from the components of body functions and structures, activity and participation and environmental factors were identified. The categories reflect functional problems and relevant environmental factors in middle-aged patients with chronic shoulder pain. The findings may have implications for clinical decision-making and promote multidisciplinary communication. Future work should investigate whether the patient’s perspective is sufficiently addressed in the current practice of shoulder pain rehabilitation.
acknowledgements
The authors would like to thank the participants in this study and the staff working at the outpatient clinic of the Department of Physical Medicine and Rehabilitation at Oslo University Hospital – Ullevaal.
REFERENCES

