Liisamari Krüger, MD, PhD,1, Timo Pohjolainen, MD, PhD,1, Ilkka Kaitila, MD, PhD,2, Hannu Kautiainen, MD3, Marja Arkela-Kautiainen, MD4 and Heikki Hurri1, MD, PhD,
From the 1Orton Rehabilitation, Orton Orthopaedic Hospital, 2Helsinki University Central Hospital, Helsinki, 3Unit of Family Practice, Central Finland Central Hospital, Jyväskylä, and Unit of Primary Health Care, Kuopio University Hospital and 4Lahti University of Applied Science, Lahti, Finland
OBJECTIVE: The purpose of the present study was to gain a comprehensive view of the quality of life and socioeconomic conditions in a more representative sample of patients with diastrophic dysplasia than previously presented.
METHODS: The study sample comprised 115 patients with diastrophic dysplasia, aged over 18 years. The patients were contacted, and 68 patients (59%) agreed to participate in the study. They answered a structured questionnaire, which included the items of RAND-36 and Finn-Health Assessment Questionnaire (Finn-HAQ) questionnaires. The Finn-HAQ items were linked to the categories of the International Classification of Functioning, Disability and Health (ICF). Population controls for matching the participating patients for age and sex were identified in the Finnish population registry. Demographic and social factors (educational status, employment status and household income) were collected in separated questions.
RESULTS: RAND-36 showed significantly lower physical functioning in the group of diastrophic dysplasia patients than in the control group. Also, the differences in scores for energy and social functioning were significant. In the mental component scales, no significant difference was found between the groups. When compared with the controls, we found significantly lower levels in all 3 ICF components of functioning in the group of patients when Finn-MDHAQ items linked to ICF were used. Almost 75% of patients with diastrophic dysplasia belonged to the group of people with minor/low income. Some or clear worsening of economic situation due to diastrophic dysplasia was reported by 25 (58%) female and 17 (68%) male patients.
CONCLUSION: In their daily living, patients with diastrophic dysplasia have marked physical difficulties, which affect their quality of life, participation in society and their financial situation. It seems that the mental situation is not greatly affected, but a more detailed study is needed to evaluate and illuminate the psychological consequences of this severe skeletal dysplasia. Overall, the pieces of information in the present study are of high importance when designing and reorganizing rehabilitation and in supportive therapy and treatment of patients with diastrophic dysplasia.
Key words: diastrophic dysplasia; physical functioning; socioeconomic situation; quality of life.
J Rehabil Med 2013; 45: 00–00
Correspondence address: Liisamari Krüger, Rehabilitation Orton, Tenholantie 10, FI-00280 Helsinki, Finland. E-mail: liisamari.kruger@orton.fi
Accepted Nov 6, 2012; Epub ahead of print Feb 6, 2013
Introduction
Diastrophic dysplasia (DD) is a congenital skeletal dysplasia of autosomal recessive type. It is caused by a mutation in the sulphate transporter gene SLC26A2 (DTDST) (1, 2). A mutation in this gene can cause a continuum of skeletal dysplasia phenotypes, including achondrogenesis type 1B (ACG1B), atelosteogenesis type 2 (AO2), diastrophic dysplasia (DTD), recessive multiple epiphyseal dysplasia (rMED) and “de la Chapelle dysplasia” (DLCD, neonatal osseous dysplasia).
Prenatal diagnosis of DD can be made by ultrasound and molecular genetic testing (1–3). In other cases, the diagnosis can usually be made at birth on the basis of clinical features: short and disproportioned statue, short limbs, joint deformities, cervical stenosis, cleft palate, tracheomalacia, deformed ear lobes, foot deformities and symphalangism of fingers (4–12).
In adulthood we can see disproportionate dwarfism, with a mean height of 130–140 cm. Progressive degenerative changes of the articular cartilage and severe joint deformities lead often to unavoidable hip and knee arthroplasties at an early age (4–7, 9–12). Scoliosis, which is commonly found, has different grades of severities that need operative treatment in many cases (9, 13). The mental status of patients with DD is normal (2, 7, 8, 14).
There is only one earlier study evaluating the health-related quality of life (HRQoL) of people with DD. The study was carried out in 1999 by a group of Finnish orthopaedists/scientists (15). They used a 15 dimensional (15D) questionnaire to compare the HRQoL of patients with DD with that of the general population. A total of 18 patients between 17 and 31 years of age participated in the study. The study showed that, although the overall HRQoL of the patients with DD was inferior to that of the controls, the patients showed greater adaptability to deviations in their health status than did the controls (15). The purpose of the present study was to gain a comprehensive view of the HRQoL and socioeconomic conditions in a more representative sample of patients with DD than previously presented. The ultimate aim is to develop psychosocial and physical rehabilitation programmes for individuals with chronic skeletal disorders, such as chondrodysplasias.
Materials & Methods
Patients and controls
Patients. In Finland the medical and orthopaedic treatment and follow-up of children with skeletal dysplasia, including DD, are centralized to the Children’s Hospital of the Helsinki University Central Hospital (HUCH). The families are referred to the clinical genetic units of the university hospitals for confirmation of the diagnosis and for genetic counselling.
The basic healthcare is provided by the local central hospitals and public well-baby centres. Most of the families also register themselves to the Finnish Association for Short People (FASP), which is a national patient support group.
There is no official patient register for patients with skeletal dysplasia in Finland. However, almost all the patients with DD in Finland are believed to have been ascertained at the HUCH and the FASP.
Patients for our study were identified and their data collected through the databases of HUCH and FASP. We were able to trace 130 adult patients with DD: 9 of the patients had died and 3 had left Finland; 3 of the patients proved to be under 18 years old and were not included in the group. A total of 115 patients with DD over 18 years of age were found in Finland. They were contacted to ask about their willingness to participate in the study. During the spring of 2008 a structured questionnaire was sent to 89 of the 115 patients who were interested in participating in the study. They received the questionnaire either in a traditional paper form or as e-mail, in accordance with their preferences. The final patient sample of 68 patients represents 59% of the known adult patients with DD in Finland.
Controls. For each participating patient, 4 age- and sex-matched population control subjects were randomly identified in the Finnish population registry’s sub-database. The sub-database included a random sample of > 7,000 people from Central Finland and was originally designed to identify a control population for a cohort of patients with rheumatoid arthritis. Thus, individuals from some age-sex strata were deliberately oversampled. However, within each age-sex stratum, the sampling process was purely random, assuring representativeness of the population. In 2007, the entire random sample population had been sent an extensive health questionnaire that included all questions that were used in the DD survey. The data obtained were then utilized in this study as data for the control subjects.
Methods
Questionnaire study. The patients completed a Finnish version of the validated RAND 36-item health survey 1.0 questionnaire (RAND-36) (16) and the Finnish version of the Health Assessment Questionnaire (HAQ) (17). The HAQ contains 20 questions covering different levels of activities of daily living (ADL): dressing and grooming, arising, eating, walking, hygiene, reach, grip and activities. The items of the HAQ questionnaire include standard 1–4 response options. Raw responses to the HAQ scales were recorded from 1–4 to 0–3, 0 representing good and 3 the poorest functional ability. Our questionnaire also included a 100-mm visual analogue scale (VAS) for the patient’s overall assessment of pain. A question about turning taps on and off was not included because it was not found relevant for “modern” daily living.
We examined the functioning of adult patients with DD and controls with a traditional applied function instrument adapted to a conceptual model, the International Classification of Functioning, Disability and Health (ICF), which belongs to the “family” of international classifications developed by the World Health Organization (WHO) for application to various aspects of health (18, 19). ICF provides functioning and health framework to be used in different healthcare settings to reflect the findings of clinical assessments conducted by health professionals (20). The ICF has two parts, each containing separate components. Part 1 covers Functioning and Disability, with components of body functions and structures, activities and participation. Part 2 comprises contextual factors including environmental and personal factors.
All the HAQ items were linked to the 3 ICF components and their domains of mobility, self-care and domestic life (Table I). ‘’Mobility’’ was divided into 3 subcategories: changing and maintaining body position, handling and walking, and moving. This subcategory included at least two questions scored from 0 to 3, and the highest score in each subcategory separately defined each patient’s score. Findings in the measurements of VAS were also linked to ICF as “Pain”. The linking rules advocated by Cieza and colleagues were applied (21).
|
Table I. Health Assessment Questionnaire items linked to the 3 International Classification of Functioning, Disability and Health (ICF) components and domains |
||
|
Item |
ICF component |
ICF domain |
|
a. Dress yourself, including tying shoelaces and doing buttons? |
Activity |
Self-care |
|
b. Shampoo your hair? |
Activity |
Self-care |
|
c. Stand up from an armless chair? |
Activity |
Mobility (body position) |
|
d. Get in and out of bed? |
Activity |
Mobility (body position) |
|
e. Cut your meat? |
Activity |
Self-care |
|
f. Lift a full cup or glass to your mouth? |
Activity |
Self-care |
|
g. Open a new milk carton? |
Activity |
Self-care |
|
h. Walk outdoors on flat ground? |
Participation |
Mobility (moving) |
|
i. Climb up 5 steps? |
Activity |
Mobility (moving) |
|
j. Wash and dry your entire body? |
Activity |
Self-care |
|
k. Take a tub bath? |
Activity |
Self-care |
|
l. Get on and off the toilet? |
Activity |
Self-care |
|
m. Reach and get a 2 kg object (bag of flour) from just above your head? |
Activity |
Mobility (handling) |
|
n. Bend down and pick up clothing from the floor? |
Activity |
Mobility (handling) |
|
o. Open car doors? |
Participation |
Mobility (handling) |
|
p. Open jars which have been previously opened? |
Activity |
Mobility (handling) |
|
q. Run errands and shop? |
Participation |
Domestic life |
|
r. Get in and out of car? |
Participation |
Mobility (moving) |
|
s. Do chores such as vacuuming, yard work? |
Participation |
Mobility (handling) |
|
Visual Analogue scale pain |
Body structure and functions |
Sensory functions and pain |
The RAND-36 is a measure of HRQoL containing 36 items on 8 scales: physical functioning, bodily pain, role limitation due to physical health problems (hereafter called role functioning/physical), general health, energy, role limitation due to personal emotional problems (hereafter called role functioning/emotional), emotional wellbeing, and social functioning. The raw responses in the questionnaire were re-coded according to the original version of RAND-36. Each item was scored on a 0–100 range, with the lowest and highest possible scores set at 0 and 100. The higher the recoded value of the item is, the better the HRQoL.
In our study we evaluated the economic situation of patients with DD to estimate achievement of that to HRQoL despite or beside DD. The participants were asked about their household income and about the consequence of DD on their financial situation. There is an international guideline for defining the limits of minor (low) household income. We compared the household income of patients with DD with the Finnish population in 2007 using the international guideline, found on the Statistic Finland (19) website. We estimated the prevalence for DD in Finland by using the 2008 demographic data for Finnish population.
Statistical analysis
The results were expressed as means with standard deviations (SD) or counts with percentages. The 95% confidence intervals (CI) were given for the most important outcomes. CIs for the effect sizes were obtained by bias-corrected bootstrapping (5000 replications). Statistical comparison between the genders was performed by t-test, bootstrap-type t-test (5000 replications), permutation test or χ2 test, when appropriate.
Results
Demographic and socioeconomic characteristics
Demographic and social factors (educational status, employment status and household income) were collected and are shown in Table II. The mean age of the patients was 44 years (43 years for female and 25 years for male patients) and the age distribution was from 18 to 75 years. In 2007, based on their financial situation, 13.5% of Finnish people were categorized as belonging to “minor/low income” households (22). The situation among patients with DD differs greatly from that: 51 of the 68 patients with DD (almost 75%) belong to the group of people with minor/low income. Some or clear worsening of economical situation due to DD was reported by 25 (58%) of the female and 17 (68%) of the male patients. A total of 30 of the 68 patients (44%) were getting income through the disability pension. Thirty-one persons (46%) were active in the work force, either employed or studying, and only 4 persons (5%) reported being unemployed.
|
Table II. Demographic and social factors |
|||
|
Variables |
Female (n = 43) |
Male (n = 25) |
p-value |
|
Age, years, mean (range) |
44 (18–75) |
44 (24–65) |
0.88 |
|
Marriage or common-law marriage, n (%) |
12 (28) |
10 (40) |
0.42 |
|
Educational status, n (%) |
0.60 |
||
|
Basic education only |
6 (14) |
4 (16) |
|
|
Vocational education |
22 (55) |
12 (48) |
|
|
Upper secondary school |
1 (2) |
2 (8) |
|
|
Upper secondary school and vocational education |
6 (14) |
5 (20) |
|
|
Higher education |
8 (19) |
2 (8) |
|
|
Employment status, n (%) |
0.73 |
||
|
Employed |
19 (44) |
8 (32) |
|
|
Unemployed |
3 (7) |
1 (4) |
|
|
Student |
3 (7) |
1 (4) |
|
|
Disability pension |
16 (37) |
14 (56) |
|
|
Pension |
2 (5) |
1 (4) |
|
|
Monthly household income, n (%) |
0.30 |
||
|
≤ 850 € |
16 (37) |
12 (42) |
|
|
851 €–1,680 € |
15 (35) |
8 (32) |
|
|
1,681 €–2,500 € |
8 (19) |
2 (8) |
|
|
> 2,500 € |
4 (9) |
3 (12) |
|
|
Some or clear worsening of economical situation due to diastrophic dysplasia |
25 (58) |
17 (68) |
|
Quality of life
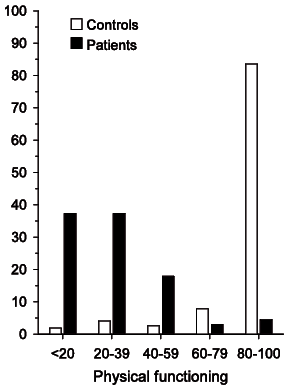
RAND-36 shows us that, in the group of the patients with DD, the physical functioning score, i.e. the physical component scales (PCS), including physical functioning, role functioning/physical, pain and general health, was significantly lower than in the control group (Table III, Fig. 2). Also the differences in scores for energy and social functioning were significant. In the mental component scales, including role functioning/emotional and emotional wellbeing, no significant differences were found between the groups (Table III).
|
Table III. RAND-36 Items of diastrophic dysplasia patients and controls |
|||
|
RAND-36 Item |
Controls n = 272 Mean (SD) [Median (IQR)] |
Diastrophic dysplasia patients, n = 68 Mean (SD) [Median (IQR)] |
p-valuea |
|
General health |
70 (20) [75 (55, 88)] |
55 (22) [60 (42, 75)] |
< 0.001 |
|
Physical functioning |
89 (19) [95 (86, 100)] |
27 (21) [25 (10, 40)] |
< 0.001 |
|
Emotional well-being |
79 (16) [84 (72, 92)] |
76 (18) [80 (64, 92)] |
0.24 |
|
Social functioning |
87 (20) [100 (75, 100)] |
78 (23) [87 (62, 100)] |
0.005 |
|
Energy/fatigue |
69 (20) [75 (60, 85)] |
63 (20) [65 (50, 80)] |
0.015 |
|
Pain |
78 (24) [90 (64, 100)] |
59 (22) [57 (45, 77)] |
< 0.001 |
|
Role limitations due to physical health |
82 (34) [100 (75, 100)] |
55 (43) [75 (0, 100)] |
< 0.001 |
|
Role limitations due to emotional problems |
83 (32) [100 (66, 100)] |
83 (29) [100 (66, 100)] |
0.99 |
|
aPermutation test. SD: standard deviation; IQR: interquartile range. |
|||
Fig. 2. Distribution between patients (n = 68) and controls (n = 272) concerning physical functioning (RAND-36) in different age groups.
Physical functioning
When using HAQ items linked to ICF, we found significantly lower levels of functioning in a group of patients compared with the controls. Significant differences in functioning between patients and controls emerged in all 3 ICF components: body functions (including pain), activity (general tasks and demands, mobility and self-care) and participation (mobility, domestic life, community, social and civic life) (Fig. 1).
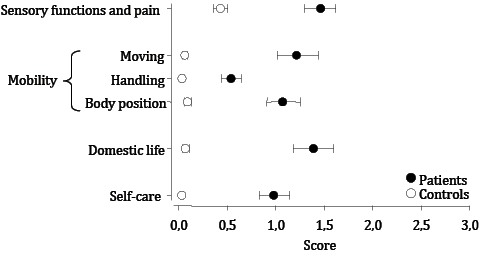
Fig. 1. Health Assessment Questionnaire items linked to the 3 International Classification of Functioning, Disability and Health (ICF) components and domains.
Discussion
Because the childhood healthcare of patients with DD in Finland is centralized, we were able to track them quite well. As a result, out of 115 adult patients in Finland, 68 participated in our study. Thus, the representation of this patient group in the study was good. A previous study (15) estimated the number of patients with DD in Finland to be 184. That included all patient age groups, not only adults. Advanced and intensified prenatal diagnostics has reduced the number of patients with DD (3, 15).
There has been increasing concern among specialists in charge for the healthcare of patients with DD in childhood, because there is no equivalent care system in adulthood. The patients sometimes report their own primary healthcare or local hospital as being incompetent or lacking knowledge regarding their rare condition. Thus, there is a considerable need for re-evaluation and reorganization within the healthcare and rehabilitation, especially for adult patients with DD. There is also a need for better awareness and knowledge of the prevailing situation of the HRQoL and functioning and disability among the patients with DD. Due to the improved diagnostic approach and medical and psychosocial healthcare at present, we can assume that the health condition and psychosocial situation of patients with DD will improve in the future.
Problems in daily living of patients with DD appear partly because of the problems related to being able to reach things caused by the short stature of a person with DD. For example, one’s everyday life can be impeded by not being able to reach the buttons in a lift or the items on a shelf, and by not being able to get on a bus or a tram. Therefore, the patient’s independence in life is limited. Because of their short stature, the patients with DD are often, in casual encounters, treated like children. Significant dissimilarity in body shape, when compared with normal population, could be a burden on its own. So both physical and mental aspects that are easy to observe could affect the quality of life.
Beginning at the time of birth, operative treatment is very commonly needed throughout the lifetime: first, correction of the cleft palate and foot deformities and, later on, arthroplasties and other corrections of joint and spine due of deformities and degenerative changes in articular cartilage (5–7, 9, 12, 23, 24). In 2004 the walking difficulties of Finnish patients with DD were explored. Physical examination, treadmill test, magnetic resonance imaging (MRI) and neurophysiological studies were carried out on 87 patients with a mean age of 31 years (range 3–56 years). The walking difficulties experienced by affected patients seemed to have a multifactor aetiology: flexion contractures of the knees, early and rapid osteoarthritis, equines or equinovarus foot deformities and obesity (25). In another study, the same researcher group investigated the thoracic and lumbar spine of patients with DD and found abnormal disc structures and rapid degeneration, explaining the decreased mobility of spine. In their study, these were considered as causative factors in the development of scoliosis (26).
In our study, both HAQ/ICF and RAND-36 data showed, in the patient group, significantly poorer physical functioning score than in the control group, whereas no significant difference between patients and controls was found regarding mental components in RAND-36. Despite the assumption that patients with DD do have problems in physical functioning, the sharpened nature of the results in HAQ when linked to categories of the ICF is startling: in all charted areas of functioning, the deviation between the patients and controls is quite augmented. Because of the overlapping of the mobility domain between the categories of activity and participation, we use partial overlap of the wide range of mobility items used in the HAQ and the social context connected with some of these items. There has been criticism concerning the confusion between the definitions of activity and participation and the lack of theoretical coherence in this part of ICF.
Interest in the measurement of HRQoL has increased and is important in all areas of medical science. Research in rehabilitation medicine and supportive therapy and treatment, particularly, would benefit of evaluation of HRQoL. Still, we must keep in mind that the concept of QOL is controversial, and there is a lack of international consensus on the definition of HRQoL. We used the RAND-36 questionnaire, which contains the same items as the Short Form 36-item questionnaire (SF-36), but with a slightly different scoring system. The results are nevertheless comparable.
In 1999, Vaara et al. (15) used a standardized 15D method to compare HRQoL of patients with DD with controls. They found the general shape of the profile of the patients with DD similar to that of the controls. When the 15 dimensions were ranked by their mean importance weight, the patients with DD valued the dimensions differently (27).
The 15D profile was derived by averaging the levels ticked by the respondents on each dimension. The profile indicates the group’s mean position on the dimensions.
This kind of mean 15D score was significantly lower in patients with DD than in the controls (15). As the differences were observed on all levels and in all dimensions, they reflected the tolerance of the patients with DD to changes regarding their own health status.
Our results on HRQoL in patients with DD differ from those of Vaara et al. (15). A different questionnaire was used, but we also had a markedly higher sample of patients with a very good representation of all patients with DD in Finland. By using RAND-36 and combining the interpretation with the results of HAQ, we had the chance to identify and separate physical restriction from mental fragility. Physical impairment of patients with DD is clearly seen in the scale of Physical functioning and in Role limitations due to physical health. Also, the scales of pain and general health in a group of patients differ significantly from those of the controls. Observing the scales that measure mental functions and capacity, there is no significant difference between patients and controls in any of the measured scales.
This is the first time that we have obtained, with the help of demographic data and evaluation of household income, a sound view of the economic situation of patients with DD. Based on the demographic data of Statistics Finland, 13.5% of Finnish people had a “minor/low income” in 2007. Comparing the income limit to the results of income evaluation among the patients with DD, we see that almost 75% of them remain within the “minor/low income” bracket. This means that the number of people with minor income among the patients with DD is almost 6 times more than in healthy population. At the same time, 62% of the patients with DD think that the disease has an influence on their economical situation. This is seen as due to low household income caused by lost work capacity or higher costs on account of the disease.
A great number of patients received income through the disability pension. Those persons presumably belong to the low-income group. A minority of patients (5%) reported being unemployed. Observing the patients’ educational situation, we notice that 24 of the 68 patients (35%) had graduated from upper secondary schools or had higher education. While we might expect higher income corresponding to high level of education, minor income can be explained by the great number of persons getting their income through the disability pension.
Unfortunately we do not have the equivalent demographic and socioeconomic characteristics of the control group, but we may look, in the literature, at comparable patient groups and their socioeconomic situation. A study among patients with achondroplasia (ACH) showed that children in this patient group received a normal education, but the reported occupational level of female adult patients was lower than that of their unaffected siblings (28). A large study in the USA investigated the QoL of 189 ACH patients and compared that with 136 unaffected first-degree relatives of the affected individuals. They found that the patients with ACH had lower annual income and less education than their healthy relatives. The study also revealed that, when focusing on advantages and disadvantages, the ACH patients were as likely to cite disadvantages relating to social barriers as they were to cite those relating to health and functioning (29). A survey of 472 chronically ill and disabled Norwegian adults with 4 different main diagnoses (asthma, haemophilia, osteogenesis imperfecta and rheumatic disease) showed that, compared with the total population, their level of education was lower, and fewer of them were active in the work force (30). Also, among adult patients with juvenile idiopathic arthritis, it was found that there was a high rate of unemployment despite the patients’ excellent educational attainment, which was comparable to that of local controls (31).
In conclusion, in their daily life patients with DD have marked physical difficulties, which affect their quality of life, participation in society, activity in the work force and their financial situation. Comparing the results of previous research in comparable patient groups, we can assume that socioeconomic reasons also significantly affect the QoL of patients with DD, although the physical impairment in this patient group is undoubtedly of more importance than in many other chronically disabled patient groups. It seems that the patient’s mental state itself is not heavily affected, but a more detailed study is needed to evaluate and illuminate the psychological consequences of this severe skeletal dysplasia. Overall, the pieces of information in the present study are of high importance when designing and reorganizing rehabilitation, supportive therapy and treatment of patients with DD.
References

