BACKGROUND: The Measure of Activity Performance of the Hand (MAP-Hand) is reliable and valid in patients with rheumatoid arthritis.
OBJECTIVE: To assess the validity and responsiveness of the MAP-Hand in patients with hand osteoarthritis.
METHODS: Patients were recruited from 2 rheumatology centres. The internal consistency of the MAP-Hand was assessed by Cronbach’s α. Content validity was evaluated based on patient interviews. Construct validity and responsiveness were based on predefined hypotheses of correlation between the MAP-Hand and concurrent measures.
RESULTS: Ten men and 201 women, mean age 62.8 years (standard deviation (SD) 6.8) and disease duration 12.5 (SD 7.5) years were included. A Cronbach’s α of 0.86 was determined. All 18 items in the MAP-Hand were described in the interviews. Sixty-seven percent of the correlation coefficients for baseline scores and 75% for change scores were in correspondence with the predefined hypotheses. A high correlation was found between the MAP-Hand and the Australian/Canadian Hand Osteoarthritis Index function score at baseline (rho = 0.76). A moderate correlation was found for change scores (rho = 0.52).
CONCLUSION: The content of the MAP-Hand adequately reflects described activity limitations in patients with hand osteoarthritis. The results suggest that the MAP-Hand has adequate internal consistency and responsiveness. Before the MAP-Hand is used in patients with hand osteoarthritis, evaluations of reliability and further construct validity are warranted.
Key words: osteoarthritis; hand; psychometrics; validity; responsiveness.
J Rehabil Med 2012; 00: 00–00
Correspondence address: Linda Fernandes, National Resource Center for Rehabilitation in Rheumatology, Department of Rheumatology, Diakonhjemmet Hospital, 0319 Oslo, Norway. E-mail: linda.fernandes1@gmail.com
Submitted July 2, 2011; accepted May 22, 2012
INTRODUCTION
Hand osteoarthritis (HOA) is common in people over 64 years of age; the estimated prevalence of symptomatic HOA is 13.1−26.2% in women and 7.2−13.3% in men (1–3). The distal interphalangeal (DIP) and proximal interphalangeal (PIP) joints, and the base of the thumb are usually affected (4, 5). The main symptoms of HOA are morning stiffness in one or more joints of the hand, and pain while performing activities involving hand movements (5). To monitor activity in HOA, the European League Against Rheumatism strongly recommends the use of validated outcome measures (5). In correspondence with earlier studies (6, 7), a systematic search to inform the current study demonstrated that only two of the patient-reported outcomes (PROs) were developed specifically for patients with HOA; the Australian/Canadian Hand Osteoarthritis Index (AUSCAN) (8) and the Functional Index of HOA (FIHOA) (9) (Appendix I). The item-generation of the AUSCAN and the FIHOA were developed mainly by health professionals, who pre-defined items that they considered important for HOA patients (6, 10). To our knowledge, there is no PRO of hand-related activities in HOA that has based item-generation on patients’ own descriptions of activity limitations.
In rheumatoid arthritis (RA), a new PRO measuring hand activity performance, the Measure of Activity Performance of the Hand (MAP-Hand), was developed recently and tested for construct validity by Rasch methodology (11). One advantage of the MAP-Hand is that item-generation was based on patient interviews. There are many similarities in the report of functional limitations in RA and HOA (5, 12). Both patient groups have decreased grip and pinch strength, and report similar levels of severity and difficulties in performing daily activities and hand-related activities (5, 12, 13). Furthermore, activity limitations have recently been found to be the major determinant of reduced health-related quality of life in patients with HOA (14), and both RA and HOA patients have reported “hand and finger function” as one of the most important priorities for improvement (15). Due to these overlaps in hand-related activity limitations in RA and HOA, the MAP-Hand may be a potential valid measure to monitor activity limitations in HOA. One advantage with an outcome that is valid for both RA and HOA is that it can be used across groups and it allows for comparisons between groups. In addition, it is more convenient for use in clinical practice. Instead of developing a completely new PRO for patients with HOA we therefore decided to test the validity of the MAP-Hand when used in patients with HOA; more specifically, to assess its internal consistency, content validity, construct validity and responsiveness.
PATIENTS AND METHODS
Patients
Patients diagnosed with HOA were recruited to the study from two Centres of Rheumatology in Norway. At Centre 1 (Trondheim), the patients were included between the years 2008 and 2010 from a randomized controlled trial (RCT) evaluating the effect of assistive technology (16). At Centre 2 (Oslo), two cohorts of patients with HOA were included. The first cohort was included between the years 2001 and 2003 from a longitudinal prospective cohort (17). The second cohort was included between the years 2005 and 2010 from a RCT evaluating a multidisciplinary and multifaceted intervention (18). All patients were diagnosed with HOA by rheumatologists or orthopaedic surgeons using the diagnostic criteria of the American College of Rheumatology (19). The study was approved by the Regional Committee for Medical Research Ethics and the Data Inspectorate. All patients received oral and written information about the study and signed an informed consent.
Measurements
All patients were interviewed about difficulties in performing activities of daily living. To structure the interviews, the patient-specific Canadian Occupational Performance Measure (COPM) was used (20). Administration of the COPM is a step-wise procedure. First, the patients were asked to describe activities in which they had experienced limitations. The patients were allowed to describe as many activities as they wished within the following 9 pre-defined areas: personal care, functional mobility, community management, paid/unpaid work, household management, play/school, quiet recreation, active recreation, and socialization. Thereafter, the patients scored each activity for importance on a scale ranging from 1 (not important at all) to 10 (extremely important). The 5 most important activities, i.e. the 5 activities with the highest score, were categorized as “prioritized activities”. Finally, the prioritized activities were scored for “Performance” and “Satisfaction with Performance” on a scale ranging from 1 (not able to do it, not satisfied at all) to 10 (able to do extremely well, extremely satisfied). After the interviews, patients completed the MAP-Hand (11), the AUSCAN (8), the Modified Health Assessment Questionnaire (MHAQ) (21), the pain subscale of the Arthritis Self-Efficacy Scale (ASES pain) (22), and pain and fatigue on visual analogue scales (0–100 mm) or numeric rating scales (0–10 points).
The MAP-Hand contains 18 gender- and season-neutral items of hand-related activity, scored on a 4-point scale ranging from 1 (no difficulty) to 4 (not able to do) (11). A total mean score was calculated. The AUSCAN comprises 3 domains; (i) pain (5 items), (ii) stiffness (1 item), and (iii) physical function (9 items). The items were scored on 5-point Likert scale, ranging from 0 (none) to 4 (extreme), and a mean score was calculated for each domain (8). The MHAQ includes 8 questions about performance of activities of daily living, scored on a 4-point Likert scale, ranging from 0 (without any difficulty) to 3 (unable to do). A total mean score was calculated (21). The pain subscale of the ASES contains 5 questions about the certainty of one’s own ability to cope with the pain, ranging from 10 (very uncertain) to 100 (very certain) (22). A mean score for the subscale was calculated. The patients were also clinically examined for the number of affected joints, defined as bone enlargements and deformations of the carpometacarpal (CMC) joints, metacarpophalangeal joints, DIP joints and PIP joints. In addition, they were tested for grip strength and grip ability. The maximum grip strength for each hand was measured in newton with the Grippit electronic instrument (Detektor AB, Göteborg, Sweden) (23). Force recordings were displayed on the Grippit electronic unit every 0.5 s during a 10-s period. The maximum of the 20 registrations were recorded and used for analysis. Grip ability was tested by performing the grip ability test (GAT) (24). Plain radiographs of CMC joint of the thumb (CMC1) were performed at Centre 1 to assess for radiological signs of thumb-base osteoarthritis. Standardized questionnaires were used to collect demographic data.
At baseline, all patients (n = 211) were interviewed about activity limitations, thus all 3 cohorts were included in the assessment of content validity. The MAP-Hand was developed in 2008, and therefore only patients from Centre 1 (n = 70) could complete it. Assessments of data quality, internal consistency, construct validity and responsiveness of the MAP-Hand were therefore based on data from Centre 1. A minimum of 50 participants has been suggested for analyses of construct validity and floor and ceiling effects (25).
Analysis
Demographic data were calculated as percentages or means (standard deviation (SD)) and outcome scores as means (SD) or medians (interquartile range). Differences between the included cohorts were calculated by χ2 test, independent t-tests, Mann-Whitney test, one-way analysis of variance (ANOVA), or Kruskal-Wallis test. The numeric rating scales were normalized to scale range 0–100 for between-group comparisons. Internal missing values were replaced by patient-specific mean scores, for analyses including total mean scores.
Data quality. Individual items within the MAP-Hand were assessed for missing data and centre and distribution item-response scores (including floor and ceiling effects). Floor and ceiling effects were present if 15% or more of the responders achieved the highest or lowest possible score, respectively (25).
Internal consistency. Internal consistency was defined as the interrelatedness among items (26). The MAP-Hand is based on a reflective model, i.e. all items are a manifestation of the same construct (hand-related activities) (11). Hence, we tested the interrelatedness by Cronbach’s α statistics for the total score and for each item if the item was deleted (27). A Cronbach’s α between 0.70 and 0.95 was considered an adequate internal consistency (25).
Content validity. Content validity was defined as the degree to which the content was an adequate reflection of the construct to be measured (26). For this purpose, semi-structured interviews according to the COPM were considered suitable. In order to compare the content of the COPM and the MAP-Hand, the activities described in the COPM were identified, categorized and listed. For example, for the described activities “opening jars”, “opening jam jars”, or “opening tomato juice jars”, opening jars was chosen as the category, as the two latter examples were regarded as more detailed descriptions involving the same hand grips and movements. The total number of activities and the number of patients describing and prioritizing each activity were calculated. Thereafter, all the COPM activities and the MAP-Hand items were compared and activities/items with the most precise content were linked. Continuing with the previous example, the activity opening jars in the COPM was linked with the item “opening jam jars” in the MAP-Hand. The proportion of number of linked activities was calculated and presented in Fig. 1.
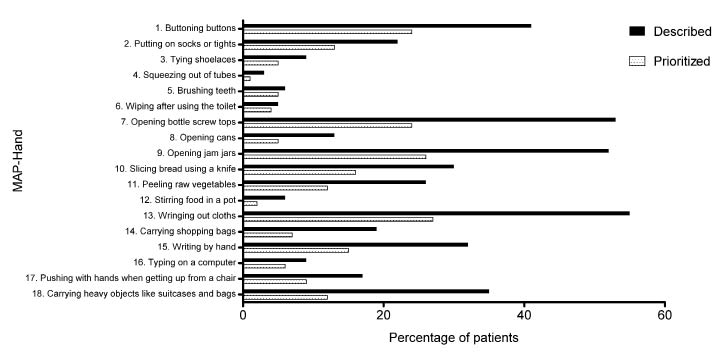
Fig. 1. Percentage of patients describing and prioritizing activities linked to the 18 items of the Measure of Activity Performance of the Hand (MAP-Hand) (n = 211).
Construct validity. Construct validity was defined as the degree to which the MAP-Hand was consistent with hypothesis (26). To evaluate construct validity, we pre-defined hypotheses of relationships between the MAP-Hand and concurrent measures. The MAP-Hand was expected to have a high negative correlation with COPM performance and a high positive correlation with AUSCAN function. Furthermore, the MAP-Hand was expected to have a moderate positive correlation with the MHAQ, pain and stiffness subscales of the AUSCAN, number of affected joints, and the GAT, and a moderate negative correlation with the ASES and the maximum grip strength test. The rationale behind expectations of high correlations between the MAP-Hand and AUSCAN function and COPM performance was because the 3 outcomes measure activity under the International Classification of Functioning, Disability and Health (ICF). Spearman’s correlation coefficients (rho) were calculated for the evaluation of the relationship between the MAP-Hand and the other included outcomes. A high correlation was defined as coefficients ≥ 0.60, moderate correlations as < 0.60 and ≥ 0.30, and low correlations as < 0.30 (28). Adequate construct validity was established if 75% or more of the correlations corresponded to the pre-defined hypothesis (25).
Responsiveness. Responsiveness is the ability of an outcome to detect change over time, if change has occurred, in the construct to be measured (25, 26, 29). Spearman’s correlation coefficients (rho) of change values (3-month follow-up scores – baseline scores) between the MAP-Hand and COPM performance, AUSCAN, MHAQ, ASES, maximum grip strength and GAT were assessed for responsiveness. Change values were not expected to correlate as highly as baseline values (construct validity). A moderate positive and a moderate negative correlation coefficient were expected between the MAP-Hand and AUSCAN function and ASES pain, respectively. The rationale for expectations of moderate correlations of change between the MAP-Hand and AUSCAN function was because both measure hand activities and both are standardized questionnaires. The ASES has been defined as a predictor for change in activity in patients with osteoarthritis (30). Hence, we expected that changes in ASES pain would correlate moderately with changes in the MAP-Hand. The remaining variables were expected to have a low correlation with the MAP-Hand (see Table V). Definitions of correlation levels (high, moderate, low) and adequacy of results (% of correlations in correspondence to hypotheses) were the same as for construct validity. SPSS 16.0 for Windows was used for all analyses.
RESULTS
Two men and 68 women were included at Centre 1, and 8 men and 133 women at Centre 2 (n = 211). They had a mean age of 62.8 years (SD 6.8) , disease duration of 12.5 years (SD 7.5), and a mean of 8.6 (SD 6.3) affected joints. All patients had been diagnosed with HOA. Baseline characteristics are shown in Table I.
| Table I. Patient characteristics |
| | Centre 1 RCT (n = 70) | Centre 2 Cohort 1 (n = 92) | Centre 2 Cohort 2 (n = 49) | p-value |
| Age, years, mean (SD) | 61 (7) | 63 (5) | 65 (8) | 0.002 |
| Disease duration, years, mean (SD) | 11 (8) | 14 (7) | − | 0.007 |
| Number of affected joints, years, mean (SD) | 13 (7) | 6 (5) | 7 (8) | < 0.001 |
| Sex, % female | 97 | 95 | 94 | 0.65 |
| Employed, % yes | 56 | 30 | 60 | 0.001 |
| Education >12 years, % yes | 39 | 35 | 71 | < 0.001 |
| Radiological OA sign of the CMC1, % yes | 74 | − | − | − |
| Comorbidity present, % yes | 63 | 48 | 80 | 0.001 |
| MAP-Hand (1–4), median (IQR) | 1.9 (1.7–2.2) | − | − | − |
| COPM performance (1–10), median (IQR) | 5.4 (4.1–7.1) | 4.4 (3.4–6.6) | 5.8 (4.0–6.6) | 0.14 |
| COPM satisfaction (1–10), median (IQR) | 4.0 (3.2–5,2) | 4.8 (2.8–6.0) | 4.4 (2.8–5.9) | 0.82 |
| AUSCAN function (0–4), median (IQR) | 2.1 (1.7–2.6) | 1.9 (1.1–2.4) | 2.3 (2.0–2.8) | 0.001 |
| AUSCAN stiffness (0–4), median (IQR) | 2.0 (2.0–2.0) | 2.0 (1.0–2.0) | 2.0 (1.0–3.0) | 0.47 |
| AUSCAN pain (0–4), median (IQR) | 2.0 (1.4–2.5) | 1.4 (1.0–2.0) | 2.1 (1.6–2.8) | < 0.001 |
| MHAQ (0–3), median (IQR) | 1.5 (1.3–1.7) | 1.5 (1.1–1.8) | − | 0.93 |
| Pain: VAS or NRS (0–100), median (IQR) | 45 (32–55) | 44 (27–57) | 60 (40–70) | 0.001 |
| Fatigue: VAS or NRS (0–100)), median (IQR) | 41 (21–54) | 45 (19–71) | 50 (15–60) | 0.60 |
| ASES pain (10–100), median (IQR) | 58 (48–64) | − | 70 (62–82) | < 0.001 |
| Maximum grip strength, N, mean (SD) | 152.3 (74.6) | 147.0 (87.5) | − | 0.39 |
| GAT, s, mean (SD) | 23.4 (6.3) | 34.8 (12.5) | − | < 0.001 |
| MAP-Hand: 1 = no difficulty, 4 = not able to do; COPM: 1 = not able to do it, not satisfied at all, 10 = able to do extremely well, extremely satisfied; AUSCAN: 0 = none, 4 = extreme; MHAQ: 0 = without difficulty, 3 = unable to do; VAS or NRS: 0 = none, 100 = extreme; ASES: 10 = very uncertain, 10 = very certain. SD: standard deviation; CMC1: carpometacarpal joint of the thumb; OA: osteoarthritis; MAP-Hand: Measure of Activity Performance of the Hand; IQR interquartile range; COPM: Canadian Occupational Performance Measure; AUSCAN: Australian/Canadian OA Hand Index; MHAQ: Modified Health Assessment Questionnaire; VAS: visual analogue scale; NRS; numeric rating scale (0–10 scales were normalized to 0–100 scales); ASES pain: pain subscale of the Arthritis Self-Efficacy Scale; GAT: grip ability test. |
Data analyses
Data quality. Few missing data were found. All items, except “Typing on a computer”, were completed by the patients (Table II). There were no floor or ceiling effects in the total score of the MAP-Hand. Of the item response scores, all 18 items had respondents scoring the lowest possible score and 14 out of the 18 items had respondents scoring the highest possible score (Table II).
| Table II. Data quality and Cronbach’s α of the Measure of Activity Performance of the Hand (MAP-Hand) (n =70). Range of possible scores (1–4 points), median (interquartile range) of total and item scores, number of missing values and percentage of patients responding the highest or lowest score. Higher score indicating more difficulties in performing the activity |
| Rank | Activities | Possible score | Median (interquartile range) | Missing n | Lowest % | Highest % | Cronbach’s α |
| Total score | 1–4 | 1.9 (1.7–2.2) | 0 | 0 | 0 | 0.86 |
| 1 | Buttoning buttons | 1–4 | 2.0 (2.0–2.0) | 0 | 23 | 0 | 0.86 |
| 2 | Putting on socks or tights | 1–4 | 2.0 (1.0–2.0) | 0 | 49 | 10 | 0.85 |
| 3 | Tying shoelaces | 1–4 | 2.0 (1.0–2.0) | 0 | 30 | 1 | 0.86 |
| 4 | Squeezing out of tubes | 1–4 | 2.0 (2.0–2.3) | 0 | 17 | 24 | 0.85 |
| 5 | Brushing teeth | 1–4 | 1.0 (1.0–1.3) | 0 | 76 | 1 | 0.86 |
| 6 | Wiping after using the toilet | 1–4 | 2.0 (1.0–2.0) | 0 | 66 | 9 | 0.86 |
| 7 | Opening bottle screw tops | 1–4 | 3.0 (2.0–3.0) | 0 | 3 | 9 | 0.87 |
| 8 | Opening cans | 1–4 | 3.0 (2.0–3.0) | 0 | 9 | 7 | 0.86 |
| 9 | Opening jam jars | 1–4 | 3.0 (2.0–3.0) | 0 | 3 | 9 | 0.86 |
| 10 | Slicing bread using a knife | 1–4 | 2.0 (1.0–2.0) | 0 | 30 | 14 | 0.86 |
| 11 | Peeling raw vegetables | 1–4 | 2.0 (2.0–3.0) | 0 | 13 | 1 | 0.85 |
| 12 | Stirring food in a pot | 1–4 | 2.0 (1.0–2.0) | 0 | 37 | 9 | 0.86 |
| 13 | Wringing out cloths | 1–4 | 2.0 (2.0–3.0) | 0 | 6 | 4 | 0.86 |
| 14 | Carrying shopping bags | 1–4 | 2.0 (2.0–3.0) | 0 | 9 | 1 | 0.86 |
| 15 | Writing by hand | 1–4 | 2.0 (1.0–2.0) | 0 | 63 | 1 | 0.87 |
| 16 | Typing on a computer | 1–4 | 1.0 (1.0–2.0) | 5 | 31 | 0 | 0.87 |
| 17 | Pushing with hands when getting up from a chair | 1–4 | 1.0 (1.0s–2.0) | 0 | 54 | 0 | 0.86 |
| 18 | Carrying heavy objects, such as suitcases or bags (over 5 kg/11 lb) | 1–4 | 2.0 (2.0–3.0) | 0 | 10 | 0 | 0.87 |
Internal consistency. An overall Cronbach’s’ α of 0.86 was found when the 5 missing values were imputed and 0.87 when no imputation for missing was made. Cronbach’s α ranged from 0.85 to 0.87 for individual items.
Content validity. The 211 patients described 311 different activities. These 311 activities were described 1737 times and prioritized 819 times. The described activities represented 8 of the 9 pre-defined areas in the COPM. The play/school area was not represented. No new activity category was required. The 2 most common areas for described activities were household management (37%) and personal care (17%). All items in the MAP-Hand were described and prioritized in the COPM-interviews, and 12 of the MAP-Hand items were among the 20 most commonly described activities in the COPM (Table III). The percentage of patients describing and prioritizing activities linked to the MAP-Hand ranged from 3% to 55% and 1% to 27%, respectively (Fig. 1). The items of the MAP-Hand represented 6 of the 9 areas in the COPM; personal care, functional mobility, community management, paid/unpaid work, household management, and quiet recreation. Activities not included in the MAP-Hand, but still described by 20 patients or more in the COPM were (described/prioritized); zipping (37/19), slicing cheese (22/15, women only), vacuuming (41/19), wiping the floor (39/14, women only), walking up/down stairs (37/17), holding a book (24/7), knitting (51/20, women only), sewing (33/13, women only), and skiing (46/15).
Construct validity. The correlation between the MAP-Hand and concurrent measures are presented in Table IV. The predefined hypotheses were ascertained in 6 out of 9 hypotheses (67%). The highest correlation with the MAP-Hand was AUSCAN function (rho = 0.76). Two measures correlated lower than expected with the MAP-Hand; COPM performance (rho = –0.25) and number of affected joints (rho = 0.03).
| Table IV. Construct validity. Spearman’s correlation coefficients (rho) of baseline values of the Measure of Activity Performance of the Hand (MAP-Hand) and patient-reported outcomes, clinical examination, and performance-based tests (n = 70). Expected positive (+) or negative (-) direction of correlation |
| | | MAP-Hand (rho) | Expected level and direction of correlation | |
| COPM | Performance | –0.25 | High (–) | No |
| AUSCAN | Function | 0.76 | High (+) | Yes |
| | Pain | 0.55 | Moderate (+) | Yes |
| | Stiffness | 0.25 | Moderate (+) | No |
| MHAQ | | 0.46 | Moderate (+) | Yes |
| ASES | Pain | –0.32 | Moderate (–) | Yes |
| Number of affected joints | 0.03 | Moderate (+) | No |
| Maximum grip strength | –0.32 | Moderate (–) | Yes |
| GAT | | 0.43 | Moderate (+) | Yes |
| Yes: expected correlation confirmed; No: expected correlation not confirmed; COPM: Canadian Occupational Performance Measure; ASES: Arthritis self-efficacy scale; AUSCAN: Australian/Canadian OA Hand Index; MHAQ: Modified Health Assessment Questionnaire; GAT: Grip Ability Test. |
Responsiveness. Sixty-six patients completed the MAP-Hand at baseline and at the 3-month follow-up. Four patients were excluded from the study due to hand surgery in the intervening period. The correlations between change scores are shown in Table V. The predefined hypotheses were ascertained for 6 out of 8 hypotheses (75%). The AUSCAN pain (rho = 0.34) and the MHAQ (rho = 0.39) correlated more highly than expected with the MAP-Hand.
| Table V. Responsiveness. Spearman’s correlation coefficients (rho) of change values between baseline and the 3-month follow-up for the Measure of Activity Performance of the Hand (MAP-Hand) and patient-reported outcomes, clinical examination, and performance-based tests (n = 70). Expected positive (+) or negative (-) direction of correlation |
| | | MAP-Hand (rho) | Expected level and direction of correlation | |
| COPM | Performance | –0.17 | Low (–) | Yes |
| AUSCAN | Function | 0.52 | Moderate (+) | Yes |
| | Pain | 0.34 | Low (+) | No |
| | Stiffness | 0.11 | Low (+) | Yes |
| MHAQ | | 0.39 | Low (+) | No |
| ASES | Pain | –0.34 | Moderate (–) | Yes |
| Maximum grip strength | –0.05 | Low (–) | Yes |
| GAT | | 0.06 | Low (+) | Yes |
| Yes: expected correlation confirmed; No: expected correlation not confirmed; COPM: Canadian Occupational Performance Measure; ASES: arthritis self-efficacy scale; AUSCAN: Australian/Canadian OA Hand Index; MHAQ: Modified Health Assessment Questionnaire; GAT: Grip Ability Test. |
DISCUSSION
The results of this study show that the MAP-Hand has a valid content and adequate internal consistency, and suggest that it has adequate responsiveness in patients with HOA. The MAP-Hand comprises a variety of activities of daily living and uses terminology that combines the patient perspective with the ICF model (11).
Earlier studies have highlighted the scarcity of PROs that monitor activity performance in patients with HOA and have emphasized the need for outcomes that include concepts that are described as important by patients themselves (10, 31, 32). This study is the first to include patients’ own descriptions of their activity limitations in a HOA-specific outcome. The main reason for using the COPM, rather than less controlled interviews, in the assessment of content validity was the intention of describing a collective meaning of what types of activities were experienced as problematic in the patients’ own environments. Another reason was that the original item pool for the MAP-Hand was generated by the COPM (11). The most commonly described activities in the COPM were linked to the items in the MAP-Hand. The linking procedure showed that all items were described and prioritized (Fig. 1), and 12 of the 20 most commonly described activities in the COPM were linked to the MAP-Hand (Table III). Four of the 20 most commonly described activities not linked to the MAP-Hand were either gender- or season-specific activities, meaning that they would be excluded from a discussion of potential activities to add to the MAP-Hand (11). That leaves 4 activities, i.e. vacuuming, zipping, walking up/down stairs, and holding a book or magazine, to be discussed as potential activities to add. Based on results from Rasch analysis, vacuuming and zipping have previously been excluded from MAP-Hand (11), stair walking is not a hand-specific activity, and holding a book or magazine was prioritized by one patient only. Thus, none of the 8 activities frequently described in the COPM-interviews but not linked the MAP-Hand (Table III) would be important enough to be added to the MAP-Hand. Considering that all items in the MAP-Hand were described and prioritized in the interviews and that 12 of the activities in the MAP-Hand were the most frequently described COPM-activities, we suggest that the content of the MAP-Hand adequately reflects and covers important activities for patients with HOA. However, the MAP-Hand has been developed and tested for content validity in Norwegian-speaking patients, and would need to be cross-culturally adapted before being used in other languages and cultures.
| Table III. Content validity. Rank order of the 20 most commonly described and prioritized activities in the semi-structured interview, the Canadian Occupational Performance Measure (COPM) (n = 211) |
| Rank | Activities | Area in COPM | Described n | Prioritized n | Linked |
| 1 | Wringing out cloths | Household | 117a | 58 | + |
| 2 | Opening bottles | Household | 111a | 50a | + |
| 3 | Opening jars | Household | 110a | 56 | + |
| 4 | Buttoning | Personal care | 87a | 50a | + |
| 5 | Carrying heavy objects | Community | 74a | 25a | + |
| 6 | Writing by hand | Work or quiet recreation | 67 | 31 | + |
| 7 | Slicing bread | Household | 64a | 34 | + |
| 8 | Peeling raw vegetables | Household | 55 | 25 | + |
| 9 | Knitting | Quiet recreation | 51 | 20 | − |
| 10 | Putting on socks or tights | Personal care | 47a | 28a | + |
| 11 | Skiing | Active recreation | 46a | 15a | − |
| 12 | Vacuuming | Household | 41a | 19a | − |
| 13 | Carrying shopping bags | Community | 40a | 14a | + |
| 14 | Wiping the floor | Household | 39 | 14 | − |
| 15 | Zipping | Personal care | 37a | 19a | − |
| 16 | Walking up/down stairs | Functional mobility | 37a | 17a | − |
| 17 | Raising from sitting | Functional mobility | 35a | 20 | + |
| 18 | Sewing | Quiet recreation | 33 | 13 | − |
| 19 | Opening cans | Household | 28 | 11 | + |
| 20 | Holding a book or magazine | Work or quiet recreation | 24a | 7 | − |
| aDescribed/prioritized by both sexes. +: linked to the Measure of Activity Performance of the Hand; −: not linked to the MAP-Hand; Household: household management; Community: community management. |
The baseline correlation between the MAP-Hand and the AUSCAN was high (rho = 0.76) and corresponded with the predefined hypothesis. An earlier study showed a correlation of rho = 0.88 between the AUSCAN function and the FIHOA (7). The high correlation can be explained by the PROs measuring the same construct; activity under the ICF (33). Correlation with COPM performance, on the other hand, was lower than expected (rho = –0.25). A possible reason for this low correlation might be the different formats of these two measures, despite the fact that they both measure activity. While the MAP-Hand represents a standardized self-reported outcome, the COPM is a patient-specific outcome, in which the patients themselves select the items to be scored. The 5 prioritized activities in the COPM may or may not be included in the MAP-Hand, depending on individual priority. A surprisingly low correlation was also found for the MAP-Hand and the number of affected joints (rho = 0.03). This finding contradicts earlier findings, which demonstrated a relationship between Heberden’s nodules, tenderness and pain, and activity performance measured with the FIHOA (34, 35). The low correlation in our study may indicate that activity performance was affected to only a very small degree by the number of joints with deformities in the included sample. According to Terwee et al. (25), 75% of the predefined hypotheses should correspond with the actual correlations in order to be defined as adequate content validity. In this study, 6 out of 9 (67%) predefined hypotheses corresponded with the correlation coefficients, hence the MAP-Hand did not achieve adequate construct validity. Since the AUSCAN stiffness variable showed low variation (median 2.0, interquartile range 2.0–2.0), presumably because the subscale includes only one item, correlation analysis may not be the optimal method for this variable. The construct validity of the MAP-Hand should therefore be tested further in future studies and the inclusion of single-item subscales for correlation analysis in samples with low variation may need to be reconsidered.
The results suggest that the MAP-Hand had an adequate responsiveness, as 75% of the correlation coefficients of change values were consistent with pre-defined hypotheses. To our knowledge, this is the first study to evaluate relationships of change values in HOA-specific outcomes, which is now a method recommended by the international COSMIN group (26, 36). We expected the MAP-Hand and the AUSCAN function to have the highest relationship of change values, since the two outcomes have several items in common and both measure hand-related activities in daily living. In other words, a one-unit change in the MAP-Hand would correlate more highly with a one-unit change in the AUSCAN function than with outcomes measuring other constructs, for example pain. This was confirmed in our analyses. Furthermore, since the MAP-Hand and the COPM performance represent two different types of outcome (as discussed above) we did not expect a one-unit change in the COPM to represent a concordant change in the MAP-Hand. However, the correlations between change scores of the MAP-Hand and the AUSCAN pain (rho = 0.34) and the MHAQ (rho = 0.39) were higher than expected. Changes in pain and overall activity limitations seemed to have a higher than expected correlation with change in hand-related activities. Future studies evaluating relationships of change scores in hand-specific outcomes may elucidate the current findings.
In comparison with the AUSCAN function, the MAP-Hand includes more items. An outcome that addresses a variety of activities covering different aspects and difficulty levels is likely to enhance the outcome’s sensitivity to the construct, as it covers a wide spectra of severity (here, difficulty level of activity performance), which are important components for discriminative ability and responsiveness to change (37). More items also make the MAP-Hand feasible as a basis for developing individually tailored rehabilitation plans. If necessary, supplementing the MAP-Hand with an open-scale outcome, such as the Patient-Specific Functional Scale, in which patients can add other activities of importance to daily functioning, has been suggested (38). This would provide clinicians with important information for goal-setting processes and in planning and evaluating interventions.
One limitation of this study is that there were few male participants. Furthermore, all participants were hospital recruited, and hence, the MAP-Hand should be further validated in primary-care-recruited samples and in samples with more male participants. The MAP-Hand was not assessed for test-retest reliability; consequently it should be evaluated for measurement error and reliability before use in clinical settings or intervention studies (27). Analyses of internal consistency should ideally include a sample of at least 100 participants, which was not achieved in this study (25). Future studies evaluating internal consistency should therefore consider including a larger sample than in the current study. Strengths of this study include a large sample, the application of inclusion criteria often used in clinical practice, recruitment of patients from different districts and with different need for healthcare (some patients were visiting the rheumatology centre for the first time while others had visited the centre many times). The large sample, variations within groups and differences between groups at baseline strengthen the results for content and construct validity. The included sample had a mean age representative of the HOA population (2, 39), and studies have shown that more women than men are affected by HOA (2, 3, 39).
In conclusion, the content of the MAP-Hand was found to be relevant and important for patients with HOA. The measurement properties of the MAP-Hand showed adequate internal consistency and content validity, and the results suggest adequate responsiveness to change. Reliability assessments and further construct validity assessments are needed to supplement the results of this validation study.
REFERENCES