OBJECTIVE: To explore the effectiveness of neurorehabilitative training using an electroencephalogram-based brain– computer interface for hand paralysis following stroke.
DESIGN: A case series study.
SUBJECTS: Eight outpatients with chronic stroke demonstrating moderate to severe hemiparesis.
METHODS: Based on analysis of volitionally decreased amplitudes of sensory motor rhythm during motor imagery involving extending the affected fingers, real-time visual feedback was provided. After successful motor imagery, a mechanical orthosis partially extended the fingers. Brain–computer interface interventions were carried out once or twice a week for a period of 4–7 months, and clinical and neurophysiological examinations pre- and post-intervention were compared.
RESULTS: New voluntary electromyographic activity was measured in the affected finger extensors in 4 cases who had little or no muscle activity before the training, and the other participants exhibited improvement in finger function. Significantly greater suppression of the sensory motor rhythm over both hemispheres was observed during motor imagery. Transcranial magnetic stimulation showed increased cortical excitability in the damaged hemisphere. Success rates of brain–computer interface training tended to increase as the session progressed in 4 cases.
CONCLUSION: Brain–computer interface training appears to have yielded some improvement in motor function and brain plasticity. Further controlled research is needed to clarify the role of the brain–computer interface system.
Key words: rehabilitation; upper extremity; imagery; neuroplasticity.
J Rehabil Med 2011; 00: 00–00
Correspondence address: Keiichiro Shindo, Department of Rehabilitation Medicine, Keio University Tsukigase Rehabilitation Center, 380-2 Tsukigase, Izu-shi, Shizuoka 410-3293, Japan. E-mail: krugreims@yahoo.co.jp
Submitted February 4, 2011; accepted June 28, 2011
Introduction
Stroke is a leading cause of disability, which results primarily from motor impairment. Although many approaches have been used to improve recovery of upper extremity (UE) function, few interventions are available for patients with severe hemiparesis (1). Newer neurorehabilitation techniques using brain–computer interface (BCI) technology have been proposed for patients with severe paresis after stroke (2, 3). BCI is capable of bypassing the normal motor output neural pathways and directly translating brain signals into commands for control of external devices (4). Extrinsic feedback is expected to promote motor learning and to improve UE motor recovery after stroke (5). Approaches using BCI technology might thus facilitate neural network plasticity and restore function through motor relearning, in addition to its substitutive functions in improving patients’ quality of life.
BCI systems of this type usually estimate the patient’s motor intention from the changes in brain activity over primary sensorimotor cortex (termed the sensory motor rhythm; SMR) and display them through visual feedback. Indeed, magnetoencephalography (MEG)-based BCI (2, 6) and electroencephalogram (EEG)-based BCI (6–8) have been tested for their ability to improve motor function in patients with chronic stroke. A long series of interventions using BCI technology yielded some plastic changes in the SMR (2, 6) and improvement in motor performance (6–8). BCI systems are thus expected to help guide cortical reorganization by motor learning, and to make neurorehabilitative approaches more effective.
However, it remains unclear how neurofeedback training with BCI systems induce clinical and neurophysiological changes in stroke patients. In terms of the time and space needed to implement BCI training, EEG-based BCI is a realistic alternative for widespread clinical application (4). It is therefore important to determine how EEG-based BCI training impacts stroke patients clinically and neurophysiologically. The aim of this study was to explore the effectiveness of our neurofeedback training using EEG-based BCI for moderate to severe paresis of the affected UE in patients with chronic stroke.
Methods
Participants
Participants were recruited from among stroke outpatients at the Tokyo Metropolitan Rehabilitation Hospital. Inclusion criteria were: (i) first unilateral stroke; (ii) time from stroke onset longer than 180 days; (iii) age between 20 and 80 years; (iv) finger test score on the Stroke Impairment Assessment Set (SIAS (9), see Appendix I) less than 3; (v) passive range of motion greater than 0 degrees for affected wrist extension and –10 degrees for metacarpophalangeal (MP) joint extension; (vi) ability to walk independently in daily life with or without assistance; and (vii) Mini-Mental State Examination score over 23 (10). Exclusion criteria consisted of: (i) any improvement in the paretic UE function during 3 months before the enrolment; (ii) severe cognitive deficits, such as unilateral spatial neglect or aphasia, precluding BCI training; (iii) severe proprioceptive deficits or pain in the paretic UE, as measured of the SIAS (9); (iv) pacemaker or other implanted stimulator use; (v) history of seizures; (vi) use of anticonvulsants, selective serotonin reuptake inhibitors, or benzodiazepines; and (vii) other serious medical conditions.
Eight candidates (all men, mean 59 years) met the criteria and gave informed consent for participation (Tables I and II). All were right-handed, and 6 participants, except case C and D, had little or no detectable surface electromyogram (EMG) activity from the affected extensor digitorum communis (EDC) when they attempted to extend their fingers.
| Table I. Patient characteristics and clinical evaluations of the 8 male patients | |
| Case | Age Years | Type of stroke | Damaged lesion | Time since stroke Months | Specific treatments in acute stroke phase | Co-morbidity | MMSE | Proprioceptive deficit | Assistance for walking outside |
| A | 47 | Haemorrhage | R TH | 23 | None | HTN | 30 | Mild | Cane |
| B | 65 | Infarction | R CR, IC | 15 | IV tPA | HTN | 30 | None | SLB |
| C | 68 | Haemorrhage | R TH | 144 | None | HTN | 30 | Mild | Cane, SLB |
| D | 67 | Haemorrhage | R TH | 34 | None | HTN | 29 | Mild | Cane |
| E | 65 | Infarction | R TH, CR | 25 | None | None | 30 | None | Cane, SLB |
| F | 60 | Haemorrhage | R IC | 51 | None | HTN | 28 | Moderate | Cane, SLB |
| G | 54 | Haemorrhage | L PU, M1 | 23 | None | HTN | 26 | None | SLB |
| H | 46 | Haemorrhage | L PU | 24 | None | HTN | 27 | None | Cane |
| R: right; L: left; TH: thalamus; CR: corona radiata; IC: internal capsule; PU: putamen; M1: primary motor cortex; IV t-PA: intravenous tissue plasminogen activator; HTN: hypertension; MMSE: Mini-Mental State Examination; SLB: short leg brace. |
| Table II. Clinical evaluations and neurophysiological examinations at pre- and post-treatment in the 8 patients |
| Case | Treatment | SIAS Knee Mouth | SIAS Finger | MAL AOU | MAS at the paretic finger | rMT over damaged M1 % | Total sessions | Bipolar pairs of electrodes |
| A | Pre Post | 3 3 | 1a 1a | 0 0 | 2 2 | 70 50 | 20 | C3-C3A C3M-C3P |
| B | Pre Post | 2 2 | 1a 1a | 0 0 | 1+ 1+ | 80< 80< | 20 | C3-C3A C3M-C3A |
| C | Pre Post | 3 3 | 1b 1c | 0.50 0.93 | 1+ 1+ | 70 55 | 18 | C3P-C3L C3-C3P |
| D | Pre Post | 3 3 | 2 3 | 0.50 0.57 | 2 2 | 45 35 | 12 | C3M-C3A C3M-C3A |
| E | Pre Post | 2 3 | 1a 1a | 0 0.14 | 1 1 | 80< 80 | 13 | C4A-C4L C4M-C4P |
| F | Pre Post | 2 2 | 1a 1b | 0 0 | 2 2 | 80< 80< | 12 | C4M-C4A C4-C4A |
| G | Pre Post | 2 3 | 1a 1b | 0 0,25 | 1+ 1 | 80< 80< | 12 | C4-C4A C4-C4M |
| H | Pre Post | 4 4 | 1b 1c | 0.36 1.14 | 1+ 1 | 80< 80< | 12 | C4-C4A C4-C4A |
| SIAS: Stroke Impairment Assessment Set; MAL AOU: Motor Activity Log Amount of Use; MAS: Modified Ashworth Scale; rMT: resting motor threshold; M1: primary motor cortex. |
The study was performed in accordance with the Declaration of Helsinki under approval by the Tokyo Metropolitan Rehabilitation Hospital ethics committee, and was registered to the UMIN Clinical Trial Registry (UMIN000001971).
Brain–computer interface system settings
Participants were seated in a comfortable chair with the arms supported and relaxed on the armrest in pronation. A 15.4-inch computer monitor was placed 60 cm in front of their eyes. A motor-driven orthosis with a servomotor (S9351, Futaba Sangyo, Tokyo, Japan: 9.5 kg cm for output torque at 4.8 V supply) achieved finger extension-flexion movement at the MP joints (Fig. 1a). The EEG was recorded with Ag/AgCl electrodes (φ = 10 mm) placed as shown in Fig. 1b. It was filtered between 2 and 100 Hz, and digitized at 256 Hz using a biosignal amplifier (g.tec Guger Technologies, Graz, Austria). The surface EMG was recorded bilaterally from the EDC muscles (high-pass filter 5Hz; sampling rate 256 Hz).
Brain–computer interface training
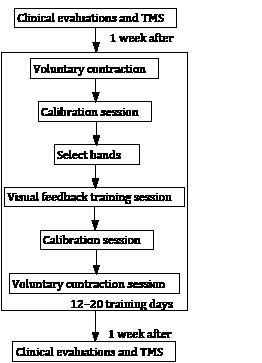
Each BCI training session consisted of 3 sessions: a voluntary contraction session, calibration session, and visual feedback training session (Fig. 2). BCI interventions were carried out for 1 h once or twice a week for a period of 4–7 months. The participants thus each had 12–20 training days.
Voluntary contraction session. The cursor moved from left to right side over a period of 8 s on the monitor, and the task cue was presented 5 s after the cursor had appeared. To help the participants imagine the affected hand opening easily, they were instructed to perform “unaffected hand opening” or “affected hand opening” voluntarily for 3 s. This training run consisted of 10 trials with 5 trials per class, alternately.
Calibration session. The calibration session was performed to adjust the EEG classifier parameters, as described elsewhere (11). After an arrow pointing to the left (“imagine paretic hand opening”) or no arrow (rest) was displayed for 1 s over a cross-shaped icon at the centre of a monitor, the participants performed the task for the next 4 s. This training run consisted of 40 trials, with 20 trials per class presented in randomized order.
Classification of SMR. SMR, representing the participant’s motor intention (12), was obtained from bilateral hemispheric EEGs every 30 ms, with a time-sliding window of 1 s during the task. On the first two trial days, C3 and C3A, and C4 and C4A were used as the bipolar pairs of electrodes. To highlight the most reactive SMR, the examiner determined the bipolar pairs of electrodes by visual inspection on the third trial day (Table II). The selected electrodes then remained the same during the succeeding trials.
The logarithms of alpha band (8–16 Hz) and beta band (16–26 Hz) components of SMR in the bilateral hemispheres were used for linear discriminant analysis (LDA, for the detail of the algorithm, see (13)) to judge whether the patient was in “Paretic hand opening” or “Rest” state. The parameters in LDA were determined by the EEG obtained during the calibration session using g.BSanalyze software (g.tec Guger Technologies, Graz, Austria). Consequently, LDA returned the value either “+1” (resting) or “–1” (opening paretic hand) every 30 ms according to the EEGs.
Visual feedback training session. The participants had to imagine the paretic hand opening or at rest for 5 s according to the task cue (Fig. 1c). The height of the cursor reflected the accumulated value of output of classification of SMR performed every 30 ms since the task started. Thus, the cursor fluctuated around the baseline if diminution of SMR was not clearly seen. The cursor goes down if the diminution of SMR was continuously observed. The gain of the cursor movement was within approximately one-tenth of the vertical range of the monitor during the resting phase in the calibration experiment. From the 4th training day, when the cursor reached the lower half on the right edge of the monitor, the motor-driven orthosis was triggered to extend the paralysed fingers from 90 to 50 degrees (Fig. 1a). Each training runs consisted of 10 trials, with 5 trials per class, presented in randomized order. Ten training runs were recorded per day, with a total of 100 trials.
Fig. 1. Brain–computer interface system settings. (a) Motor-driven orthosis. Left is neutral position, right is maximum extension position. It took approximately 3 s to open the orthosis to its maximum position, and 3 s to close it to the neutral position. The patient’s hand was fixed in the hook and loop fastener. (b) Electroencephalogram (EEG) measurement. Ten EEG electrodes were placed at C3 and C4, as designated according to the International 10/20 system, and 2.5 cm anterior (A), posterior (P), medial (M), and lateral (L) to C3 and C4. The ground and reference electrodes were located at position Fz and the left ear lobe, respectively. (c) Visual feedback monitor displayed the cursor as moving upward (rest) or downward (imagery) on the monitor based on classification of sensory motor rhythm.
Outcome measures
The following clinical evaluations and transcranial magnetic stimulation (TMS) were performed one week before and after the intervention (Fig. 2). Surface EMG activities of the affected EDC muscle and quantified EEG were compared between the first and last training days.
Fig. 2. Flow diagram of brain–computer interface training and evaluation. TMS: transcranial magnetic stimulation.
Clinical evaluations. The SIAS (9) is a standardized measure of stroke impairment, consisting of 22 subcategories, and has excellent inter-rater reliability (14, 15). Motor functions of the paretic UE are tested with the knee-mouth test and the finger test (see Appendix I). They are rated from 0 to 5, with 0 indicating complete paralysis and 5 no paresis. The amount of use scale of the Motor Activity Log-14 (MAL AOU) is a structured interview used to rate how much the arm is used in activities of daily living (range, 0–5), and has construct validity and reliability (16, 17). Spasticity for fingers was measured with the modified Ashworth Scale (MAS) (18).
Neurophysiological examinations. We used single-pulse TMS over the primary motor cortex of the affected hemisphere to assess changes in corticospinal tract excitability. The stimulator used was a Magstim 200 (Magstim, Whitland, UK), and the signals were recorded with a Neuropack MEB-2200 (Nihon Kohden, Tokyo, Japan). The outer diameter of each half-coil was 10 cm. The resting motor threshold (rMT) was defined as the intensity at which motor-evoked potentials from the affected first dorsal interosseous muscle larger than 0.05 mV were observed in at least 5 of 10 trials. For reasons of safety, stimulation intensity did not exceed 80% of the maximal output.
Time-frequency maps over both hemispheres, which showed the relationships between the tasks and the distributions of EEG band power, were compared pre- and post-BCI training. We also used the amplitude change of SMR as a feature representing cortical excitability of the sensorimotor area (11). Diminution of SMR is termed event-related desynchronization (ERD), and is expressed as the percentage power decrease in relation to the 1-s reference interval before the task in calibration session. Each ERD at the alpha and beta band was calculated every 0.1 s with a time-sliding window of 1 s and frequency (resolution of 1 Hz) determined according to the following equation:
ERD(f,t) = A(f,t) – R(f) × 100
R(f)
where A(f, t) is the power spectrum density of the EEG at time t and frequency band f, and R(f) is the power spectrum for the baseline period. Negative ERD values mean decreases of the power spectrum during motor imagery, indicating cortical activation. ERD was averaged over all calibration sessions for each hemisphere. We selected either the ERD at alpha or beta band, and compared the ERD pre- and post-BCI training using repeated measure analysis of variance (ANOVA) with PASW Statistics 17 (SPSS Inc., Illinoic, Chicago, USA). Also, success rate, i.e. how the result of the motor-driven orthosis was consistent with the task cues, was calculated at every visual feedback training session. Improvement in success rate was statistically tested with Spearman’s rank correlation test.
Results
All the participants finished the intervention without experiencing obvious adverse effects.
Clinical changes
Of the 5 participants with improvement in finger function, 3 had milder finger paresis (SIAS finger test score greater than 1a) before the training (Table II). Two exhibited improvement in arm paresis. Also, decreased spasticity in the paretic fingers was shown in 2 patients. Of the 5 cases with increased scores of the MAL AOU, 4 showed improvement in finger function. Through participation in our intervention, all cases indicated that they became more aware of use of their paretic UE in daily activities, and felt that they could relax it easier.
Neurophysiological changes
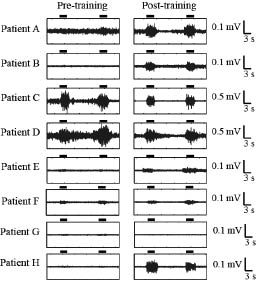
New voluntary EMG activity appeared in 4 patients who had little or no muscle activity before the training (Fig. 3), which indicated that all participants had improvement in finger function and/or voluntary EMG activity. In 2 patients with some voluntary movement, decreased muscle activities were shown during the rest condition after voluntary muscle contraction. rMT of the affected hemisphere were decreased in 4 cases, although it was too high to compare in the others (Table II).
Fig. 3. Comparison of electromyogram (EMG) activities pre- and post- brain–computer interface training. Comparison of EMG activities of the affected extensor digitorum communis muscle pre- and post-BCI training. The horizontal bars represent the period during which patients opened their paralysed hand for 3 s. Voluntary EMG activities newly appeared in 4 patients (A, B, E and H) who had little or no muscle activity before the training. In 2 patients (C and D) with some voluntary movement, decreased muscle activities were shown during the rest condition after voluntary muscle contraction.
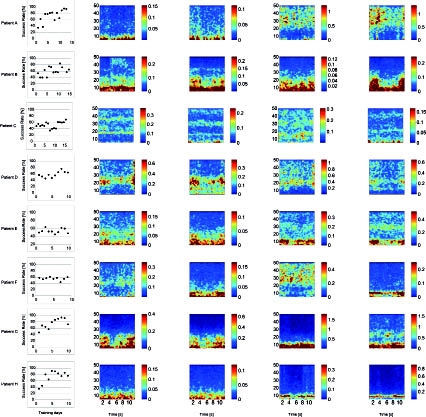
The success rate (Fig. 4a) tended to increase as the session progressed in 4 cases (rho = 0.72, 0.85, 0.68, and 0.75 for case A, C, D and G, respectively; p < 0.05). The rates apparently fluctuated due to poor concentration from lack of sleep (especially, sessions 7–10 in case C), the difficulty of maintaining imagery for 5 s, and the subject’s unrest when one trial ended in failure. Time-frequency maps (Fig. 4b–e) showing EEG changes during motor imagery became more clear after BCI training, though the bands with the most powerful change were different among individuals. We selected the ERD at the beta band in 3 patients (A, D and F) and at alpha band in the other 5 patients (Fig. 5). Two-factor [time (pre-, post-treatment), side (unaffected, affected hemisphere)] repeated measure ANOVA for the ERD showed no significant interaction of side and time (p = 0.31), but it became significantly greater over both hemispheres (p < 0.01, two-way ANOVA). Of the 6 participants who showed greater ERD changes over the affected hemispheres than those over the unaffected hemisphere, 4 showed decreased rMT of the affected hemisphere in the TMS study, which indicated increased cortical excitability.
Fig. 4. Success rate and time-frequency maps pre- and post-brain–computer interface training. (a) Changes in success rates according to the sessions from 4th training day. (b–e) Patients intended to move the paralysed hand from time 4 to 8 s. The colour bars show the power spectrum density (10 –12 [μV/Hz]). Blue indicates low power and red high power. The electroencephalogram changes over the unaffected hemisphere in (b) pre- and (c) post-BCI training, and over the affected hemisphere in (d) pre-and (e) post-BCI training.
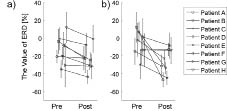
Fig. 5. Comparison of event-related desynchronizations (ERDs) pre- and post-brain–computer interface (BCI) training. The ERD over (a) the unaffected hemisphere and (b) the affected hemisphere between pre- and post- BCI training. After BCI training, the ERD became significantly stronger over both hemispheres (p < 0.01; two-way analysis of variance).
Discussion
With our EEG-based BCI training, using a strategy similar to that of Buch et al. (2), we found improvement in finger function and surface EMG activity of the affected finger extensors. Also, significantly greater suppression of the SMR over both hemispheres was observed during motor imagery. Facilitation of cortical excitability in the damaged hemisphere using the TMS was confirmed in patients with greater changes in SMR over the affected hemispheres. Some patients exhibited increased daily usage of the paralysed hand, and high success rate for control of the orthosis. Particularly noteworthy was the induction of voluntary muscle activity in patients with no or little remaining motor function. This result is very promising as a therapeutic strategy for severe impairment of the UE, since the new appearance of voluntary muscle activity induced by BCI training may open up the possibility of reinforcing it with other established interventions, such as EMG-triggered electrical stimulation (19).
The improvements induced with our EEG-based BCI neurofeedback training are thought to have some factors. Motor imagery is known to activate the lesioned brain similar to motor execution, and to induce corticospinal excitability in healthy individuals and post-stroke patients (20). It might therefore be applicable to patients with complete loss of motor function, though thus far its clinical effectiveness has been limited to mild to moderate hemiparesis (21). Our EEG-based BCI neurofeedback training induced improvement in finger function and/or voluntary EMG activity in all participants, but the changes in motor function appeared to be related to the severity of motor impairment rather than the intensity and duration of the intervention or diminution of SMR. For this reason, it may be that milder paralysis tends to be restored more easily than severer paralysis with any type of intervention (1). Also, motor imagery induced only short-term plasticity in enhancement of the area of representation of primary motor cortex and the volume of intrinsic hand muscle representation only over the damaged hemisphere in subacute stroke patients with mild to moderate hemiparesis (22). Our TMS study revealed lower rMT in the affected hand one week after BCI training. This finding suggested that BCI neurofeedback training facilitated corticospinal excitability as a lasting effect, even in patients with severe hemiparesis.
It has been reported that the majority of stroke patients showed changes in SMR during motor imagery over the affected hemisphere after the BCI training, although some showed changes over the unaffected hemisphere (2). Our results were consistent with those of the previous study (2), and supported that changes in SMR over the affected hemisphere might relate to improvement in motor control of the affected side, with decreased rMT of the affected hemisphere. On the other hand, ipsilateral activation of the unaffected motor cortex, shown during the paretic hand movement (23, 24), was considered to play an important role in the recovery of motor function after stroke (25). These results might explain the relationship between changes in SMR over the unaffected hemisphere and improvement in motor control of the affected side in some cases.
It has been shown previously that intensive passive opening and closing of the paretic hand led to improved motor function and increased cortical activation in patients with severe paresis (26). In our study, the mechanical orthosis produced some afferent inputs and mechanical stretches, which might contribute to improvement in motor control and neuroplastic changes. To reduce such effects, we set the mechanical orthosis to extend the paretic fingers partially, as well as for safety reasons. Additionally, the movement was repeated much less when compared with the previous study (26).
More frequent use of the affected UE was found in the present study. It was reported that mental practice improved motor performance and daily usage of moderately impaired UE in patients with chronic stroke (27). In particular, it is conceivable that more severe impairment and a longer period after stroke lead to decreased awareness and less usage of paretic limbs, the so-called “learned non-use” condition (28). For example, one patient (case E) stated that he had newly begun strength exercise for the affected arm of his own volition, suggesting that our BCI training might have raised awareness of and increased attempts to use the affected UE, and thus contributed in part to the recovery of motor function after the treatment. In addition, increased awareness of the paretic limb might have brought about its relaxation in resting condition.
However, there are other possible mechanisms, such as correction of hemispheric inhibition, neuroplastic changes toward more optimal reorganization induced by visual feedback of brain activity, and alterations in connectivity of the prefrontal lesion (29). This uncontrolled study was not enough to confirm possible mechanisms. The other limitations include the small sample size, and the lack of follow-up evaluation after the intervention. Further study is needed to confirm the effectiveness of our BCI training and clarify the mechanisms of improvement, including determination of the optimal intensity and duration of BCI training.
In conclusion, our BCI neurofeedback training appears to have induced some improvement in motor function and brain plasticity. BCI technology may be useful for restoring brain function in patients with stroke. In order to clarify the role of BCI system in our protocol, controlled trials need to be performed in the future.
AcknowledgementS
This study resulted from “Brain Machine Interface Development” under the Strategic Research Program for Brain Sciences by the Ministry of Education, Culture, Sports, Science and Technology of Japan.
References