OBJECTIVE: To compare the effects of 4 weeks of intervention using conventional rehabilitation, intensive conventional rehabilitation and modified constraint-induced movement therapy on the hemiplegic upper extremity in stroke patients.
METHODS: Thirty stroke patients (mean age: 63.3, SD 9.63 years; mean time since stroke: 11.33, SD 8.29 weeks) were randomly divided into 3 groups: conventional rehabilitation, intensive conventional rehabilitation, and modified constraint-induced movement therapy (10 individuals in each). Motor function was assessed using the Wolf Motor Function Test before treatment, and 2 weeks and 4 weeks after treatment.
RESULTS: The constraint-induced movement therapy and intensive conventional rehabilitation groups improved their function ability scores in the Wolf Motor Function Test significantly more than the conventional rehabilitation group after 2 weeks of treatment (p < 0.05), but all groups reached comparable levels at the end of 4 weeks of intervention. However, only the constraint-induced movement therapy intervention proved to have robust and systematic effects on the function ability scores, as revealed by the large, positive and significant correlation between the initial scores and the scores 2 and 4 weeks after the intervention. The median performance time of the Wolf Motor Function Test decreased significantly in all groups after 4 weeks of treatment (p < 0.05), but only the modified constraint-induced movement therapy group showed significant improvements both 2 and 4 weeks after the initiation of treatment.
CONCLUSION: Compared with classical intervention, modified constraint-induced movement therapy showed an apparent advantage over both conventional intervention and intensive conventional rehabilitation for patients after stroke.
Key words: stroke; constraint-induced movement therapy; intensive therapy; upper extremity.
J Rehabil Med 2011; 00: 00–00
Correspondence address: Qiang Wang, Department of Rehabilitation Medicine, The Affiliated Hospital of Medical College, Qingdao University, No. 16, Jiangsu Road, Qingdao 266003, China. E-mail: sakulawangqiang@hotmail.com
Submitted July 28, 2010; accepted March 25, 2011
Introduction
Constraint-induced movement therapy (CIMT) is a physical rehabilitation technique that has attracted considerable attention as a means of treating the more-affected upper extremity and overcome learned non-use phenomenon (1, 2) following stroke. CIMT involves the restraint of the less-affected upper extremity over an extended period, in combination with intensive task-related training of the more-affected limb (3). In the past two decades, many studies have shown the efficacy of CIMT in treating patients with stroke in both chronic and subacute stages (4–8). Typical CIMT intervention requires supervised training of the more involved limb for 6–7 h per day over 10 days, with concurrent restraint of the less-involved limb for 90% of the stroke patients’ waking hours over the same 2-week period. In contrast to clinical efficacy of CIMT, the acceptance of CIMT among therapists and patients remains poor. For instance, in Page’s study, 68% of patients stated that they were not interested in participating in CIMT, citing concerns about the practice schedule and the restrictive device schedule. Therapists cited concerns about patient adherence and safety, and speculated that facilities may not have the clinical resources to provide CIMT (9). In this case, a variety of derivatives of CIMT were devised by employing less intensive training and shorter restraint time (10–13). The key element in CIMT therapy is mass practice. Other elements include placing the unaffected arm in restraint, “shaping” (a type of training through which a desired motor objective is approached in small steps of increasing difficulty), and focusing on stimulating the functions that remain, rather than on underlying impairments (14).
The effects of intensive therapy at the neuronal level and its subsequent functional manifestations as a result of cortical reorganization have become a focal point of interest in stroke rehabilitation research in the past decade (15). A review of stroke rehabilitation literature revealed 12 randomized controlled trials involving 2813 patients that compared specialized inpatient rehabilitation with conventional care. Although there is strong evidence that early augmented exercise therapy time (expressed as time dedicated to practice) may enhance functional recovery, there is a discrepancy regarding the benefits of intensive practice (16).
The goal of the present single-blind randomized clinical study was to compare the efficacy of modified CIMT (mCIMT) with that of intensive conventional rehabilitation (ICR) in motor recovery after unilateral stroke. Conventional rehabilitation (CR) was used as control.
PATIENTS and Methods
Participants and randomization
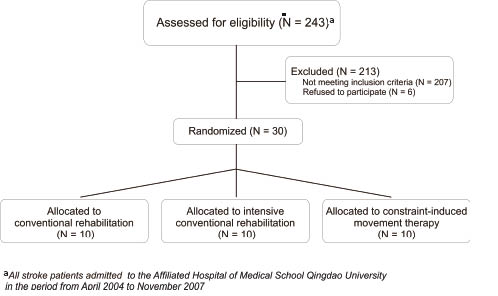
The current study aimed to recruit acute/subacute stroke patients who fulfilled all of the following inclusion criteria: (i) no excessive pain in the affected limb; (ii) ability to understand and follow verbal directions (using a Chinese aphasic battery) (17); (iii) no major cognitive deficit (Mini-Mental Status Examination score > 24) (18); (iv) active wrist extension of at least 20º, and 10º of active extension of the metacarpophalangeal joints; (v) ability to maintain standing for 2 min. Potential participants were assessed among the stroke patients admitted to the Affiliated Hospital of Medical School Qingdao University (n = 243) during the period April 2004 to November 2007 (Fig. 1). Given the difficulty of finding patients who fulfilled all the criteria, we stopped the recruitment process when we reached 30 patients; 10 per group. In this process, which lasted 3 years (2004–07), out of these 243 individuals, a total of 36 adult stroke patients were assessed as eligible and were invited to participate in the study; however, 6 patients who were eligible declined to participate. The remaining 30 participants who fulfilled the selection criteria were subsequently assessed at random (using a random numbers table) into 3 groups: a mCIMT group (10 individuals), an ICR group (10 participants), and a conventional rehabilitation CR group (10 patients). All the patients were aware of which group they were allocated to. Participants’ demographic and clinical characteristics are summarized in Table I; there were no significant differences among these groups for any of the characteristics listed. The study protocol was approved by the medical ethics committee of the Affiliated Hospital of Medical School Qingdao University, and each subject signed an informed consent.
| Table I. Descriptive characteristics of study participants (n = 30) |
| Group | | Age (years) Mean (SD) | Type of stroke | Time since stroke (weeks)Mean (SD) |
| M/ F n | Infarction n | Haemorrhage n |
| CR | 5/5 | 67 (7.45) | 8 | 2 | 9.4 (5.38) |
| ICR | 7/3 | 63.5 (9.63) | 8 | 2 | 12.7 (9.72) |
| CIMT | 4/6 | 59.4 (10.89) | 7 | 3 | 11.9 (9.59) |
| CR: conventional rehabilitation; ICR: intensive conventional rehabilitation; CIMT: constraint-induced movement therapy; SD: standard deviation. |
Fig. 1. CONSORT diagram showing recruitment and allocation of participants. aAll stroke patients admitted to the Affiliated Hospital of Medical School Qingdao University in the period from April 2004 to November 2007.
Intervention
Conventional rehabilitation. Participants in the CR group received 45 minutes of consecutive occupational therapy (OT) sessions, 5 days per week for 4 weeks. The therapy in the CR group involved strength, balance, manual dexterity exercises (e.g. grasp release, stacking cones), functional task practice when possible, and stretching/weight-bearing by the affected arm, and teaching of activities of daily living (ADLs) using the less-affected side.
Intensive conventional rehabilitation. Participants exposed to ICR received 3 h of consecutive OT sessions, 5 days per week for 4 weeks. The content of therapy was similar to CR, with emphasis on high-intensity endurance, strength and functional practice. On average, patients in this group received approximately 45 more h of training than the CR group (i.e. approximately 2.25 h of additional OT therapy per day for 20 sessions).
Modified constraint-induced movement therapy. Participants in the mCIMT group received 3 h of consecutive OT sessions, 5 days per week for 4 weeks. Therapy sessions consisted of performing tasks only with the affected upper extremity. Task movements included reaching, grasping, lifting and placing. The difficulty level of the practiced task was shaped gradually, with the goal being set just above the patient’s ability level to perform it. If this level was achieved, then the goal was set higher, thereby continually challenging the patient without overwhelming him or her (5). In addition to OT sessions, participants in this group were asked to wear a resting hand splint ensemble on their less-affected upper extremity that prevented use of that arm for approximately 90% of waking hours, excluding activities when risk of injury might increase for 20 consecutive weekdays. The caregiver recorded the amount of time the patient wore the restraint.
In all 3 types of intervention, the patients focused their rehabilitation efforts on the affected limb.
Procedures and outcome measure
The Wolf Motor Function Test (WMFT) was administered before therapy, and 2 and 4 weeks after the intervention period by the same rater, who was blinded to the group assignment. The WMFT is a graded neurological scale for assessing the function and dexterity of the affected upper limb in patients with moderate to severe upper extremity motor deficits. It contains 15 items, each of which tests single- or multiple-joint motions and functional tasks (19, 20). Some of these tasks involved limb manipulation alone (e.g. placing the forearm on a table, adjacent and parallel to its edge), while others require object or weight manipulation in addition to that of the upper limb (e.g. pulling a 1 lb weight across a given distance). The most prominent character of this scale is that both the performance time (median time to execute all timed tasks) and quality of movement (the degree to which the required task is accomplished) are explored. The median time is used for analysis because it is less sensitive to outliers than the mean score (20). The inter-rater reliability, construct validity and criterion validity of WMFT were found to be satisfactory in previous studies (19, 20). This scale has been used widely in the study of CIMT (4, 11, 12).
The mean functional ability (FA) scores and median performance time of the WMFT constituted the main outcomes assessing the efficiency of each intervention procedure. The FA score is computed for each task and can range from 0 (no attempt to use the upper extremity being tested) to 5 (movements appear to be normal), with a maximum total score of 75 points. The “normality” of the movement for the affected arm is often assessed in comparison with the non-affected arm.
Data analysis
The functional ability (FA) scores are measured on an ordinal scale; however, most papers in the literature (21–24), even those published by the author (25), treat these scores as being acquired on an interval scale; as such we used both parametric and non-parametric statistical tests for analysing FA and median time scores. Friedman’s test was used to test differences in treatment across multiple tests within each group, and Kruskal-Wallis one-way analysis of variance by ranks was used to assess group differences at each time-point (at time zero, 2 and 4 weeks after treatment). However, given that there are no non-parametric tests to assess interaction effects in a mixed design (group × time), where one independent variable is between groups and the other is a repeated measure, we employed a repeated measure analysis of variance (ANOVA) to assess this interaction effect for the FA scores and treated them as if they were measured on an interval scale. In this case, we used the one-sample Kolmogorov-Smirnov (K-S) test to check the normality of the distribution of values for the dependent variables (both functional ability scale and median time) at time zero (before the treatment). For the dependent variables, which were not normally distributed, a logarithmic transformation was applied and normality was assessed again. This ensured that there were no major violations of the statistical assumptions underlying the ANOVA analysis. Subsequently, we used ANOVA with repeated measures (pre-treatment, 2 weeks post-treatment, 4 weeks post-treatment) in order to compare the effects of the therapeutic intervention among the mCIMT, ICR and CR groups, followed by post-hoc analyses (using Bonferroni tests) assessing the pairwise differences in FA and median time scores and the post-hoc statistical power. When the post-hoc analyses sphericity assumption was violated, we used the Greenhouse-Geisser correction to report the results. The statistical software SPSS version 11.5 (SPSS Inc., Chicago, IL, USA) was used for data analysis.
In clinical research using repeated measurements to test the efficiency of a treatment or intervention, researchers often emphasize only the differences between interventions. However, these differences need to be taken into account together with the correlations between successive measurements. In this case, the correlation coefficient will inform about whether the intervention had a systematic and similar effect among all patients (i.e. a large, positive and significant correlation coefficient), whether it affected more the patients who had the worst symptoms or manifestations prior to the treatment or intervention (i.e. a large, negative and significant correlation coefficient) or whether it had an unsystematic therapeutic effect (i.e. a small correlation coefficient, positive or negative, but not significant). Based on these, we also computed the Pearson’s and Spearman’s correlation coefficients (parametric and non-parametric correlation coefficients, respectively) between the values obtained before treatment and those obtained 2 and 4 weeks after treatment for each group of subjects and for the variables of interest. Where the 2 coefficients agreed in statistical significance, we report only the Pearson’s coefficient.
Results
One-sample K-S tests revealed that, among the dependent variables (functional ability scale, median time), only the median time values of the WMFT measured prior to the intervention were not normally distributed (K-S Z = 1.51; p = 0.02). After the logarithmic transformation of this variable, the K-S test showed that the transformed values were normally distributed (K-S Z = 0.94; p = 0.33), thus warranting the use of ANOVA for this transformed variable. Prior to treatment, there were no significant differences between the 3 groups regarding the dependent variables assessed either with non-parametric (Kruskal-Wallis) or parametric (ANOVA) tests (χ2 = 2.01, degrees of freedom (df) = 2, p = 0.36 and F(2,27)= 0.51, p = 0.60 for FA; χ2 = 0.69, df = 2, p = 0.70 and F(2,27)= 0.17, p = 0.84 for median time). This ensures that all groups started from the same level and that any subsequent differences are probably due to the therapeutic intervention.
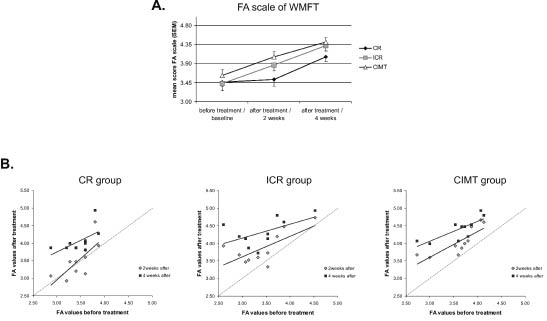
The mean FA scores of WMFT obtained before the intervention and 2 and 4 weeks post-treatment for each group are shown in Fig. 2A. The correlations between the initial assessment of FA and those 2 and 4 weeks after treatment for each group are shown in Fig. 2B. The repeated measures ANOVA shows that there is a significant interaction effect between groups and the time of measurement regarding this dependent variable (F(4,54)= 2.80, p = 0.03). This effect implies that the type of intervention (i.e. group assignment) had a different impact on FA changes in scores measured 2 and 4 weeks after treatment. Kruskal-Wallis tests showed that the 3 groups were different among themselves at 2 weeks (χ2 = 7.15, df = 2, p = 0.02) or 4 weeks (χ2 = 6.23, df = 2, p = 0.04) after onset of intervention. Post-hoc pairwise analyses, performed with Bonferroni tests to correct for multiple comparisons, revealed that the general interaction effect originated from significant differences between mCIMT and CR groups 2 weeks after treatment (F(2,27)= 3.58, p = 0.04); for the overall group differences 2 weeks after the intervention) and from marginally significant differences between the same groups 4 weeks after treatment (F(2,27)= 2.75, p = 0.08). The observed statistical power for the interaction effect was 0.75, for an alpha-level of 0.05. There were no significant differences in the changes in FA scores between the ICR and CR groups.
Fig. 2. (A) The mean score of the functional ability (FA) scale on the Wolf Motor Function Test (WMFT) test measured before, and 2 and 4 weeks after, treatment in the 3 groups. The error bars represent the standard error of the mean. (B) Scatter plots showing the correlation between the initial values of FA scores and those obtained 2 and 4 weeks after the intervention for the 3 groups. The dotted line in the graph shows the level of no change from baseline to post-treatment. CR: conventional rehabilitation; ICR: intensive conventional rehabilitation; mCIMT: modified constraint-induced movement therapy.
It is noteworthy that all groups benefited in general from their treatment, as revealed both by the Friedman’s tests (χ2 = 15.84, df = 2, p < 0.001 for the CR group; χ2 = 18.20, df = 2, p < 0.001 for the ICR group; and χ2 = 20.00, df = 2, p < 0.001 for the mCIMT group) and by significant Bonferroni tests between the initial and final values 4 weeks after the intervention (all p < 0.05); however, the CR group improved significantly only in the last 2 weeks of treatment (from the 2nd to the 4th week). While all correlation coefficients between the initial values and those after 2 weeks of treatment were large (greater than 0.7) and significant for each group, only the mCIMT group showed a significant correlation between the initial values and those 4 weeks after treatment (r = 0.78; p = 0.007; n = 10). This suggests that, regarding the FA measure, only the mCIMT intervention had a systematic effect among patients, affecting all of them to a similar extent even after 4 weeks of treatment. The ICR group scores were not significantly different from those of either the CR or the mCIMT groups, indicating that their performance was situated between that of the other two groups. This assessment is supported by the fact that after 4 weeks’ therapy, the FA scores exceeded 4.5 in one case in the CR group, 4 cases in the ICR group and 6 cases in the mCIMT group, suggesting that ICR or mCIMT is needed to gain a high level of function of the upper extremity.
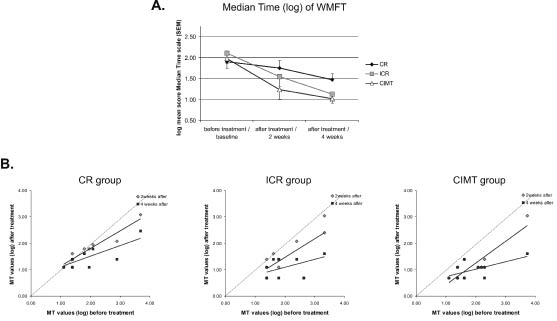
The median time scores (log) of the WMFT for each group are shown in Fig. 3A, and the correlations between the initial assessment and that 2 and 4 weeks after treatment are shown in Fig. 3B. Similar to FA, Friedman’s tests showed that the MT scores changed significantly from onset to 2 and 4 weeks after the intervention in each group (χ2 = 9.50, df = 2, p < 0.01 for the CR group; χ2 = 17.54, df = 2, p < 0.001 for the ICR group; and χ2 = 18.72, df = 2, p < 0.001 for the mCIMT group). The repeated measures ANOVA shows that there is a significant interaction effect between groups and the time of measurement regarding this dependent variable (F(4,54)= 2.81, p = 0.04). The post-hoc observed statistical power for the interaction effect was 0.65 at the alpha level of 0.05. However, unlike in the FA case, this interaction effect here originated from 2 different sources: (i) a significant difference between mCIMT and CR groups only 4 weeks after treatment (F(2,27)= 3.88, p = 0.03) and (ii) from a significant difference between the initial measurements and those post-treatment (both 2 and 4 weeks afterwards) only for the mCIMT and ICR groups (all Bonferroni tests, p < 0.05). The CR group did not show any significant differences between the initial measurements and those after treatment. Among the groups that changed the MT (median time) scores, only the mCIMT group showed significant and positive correlations between the initial and post-treatment values, both 2 and 4 weeks after treatment (r = 0.89; p = 0.001; n=10, 2 weeks post-treatment, and r = 0.64; p = 0.04; n = 10, 4 weeks post-treatment). The ICR group showed a significant correlation only 2 weeks after treatment, but not 4 weeks into the intervention (r = 0.72; p = 0.019; n = 10 2 weeks post-treatment and r = 0.57; p = 0.08; n = 10 4 weeks post-treatment). Again, the performance of the ICR group was situated between that of the other two groups.
Fig. 3. (A) Mean score (log) of the median time (MT) scale on Wolf Motor Function Test (WMFT) test measured before, and 2 and 4 weeks after, treatment in the 3 groups. The error bars represent the standard error of the mean. (B) Scatter plots showing the correlation between the initial values of MT scores and those obtained 2 and 4 weeks after the intervention for the 3 groups. The dotted line in the graph shows the level of no change from baseline to post-treatment. CR: conventional rehabilitation; ICR: intensive conventional rehabilitation; mCIMT: modified constraint-induced movement therapy.
Discussion
The CIMT treatment regimen proposed by Taub & Uswatte (26) has 3 components: (i) a repetitive, task-oriented training of the impaired extremity or function following shaping principles for several hours a day for 10 or 15 consecutive weekdays (depending on the severity of the initial deficit); (ii) constraining the patients to use the impaired extremity or function during waking hours over the course of the treatment, sometimes by restraining the unpaired extremity; and (iii) applying a package of behavioural methods designed to transfer gains made in the clinical setting to the real world. Although the third element is potentially essential for CIMT, many interventions are often defined only as a combination of intensive repetitive practice and constraining the use of the less-affected limb (27). It is thus not clear which component contributes to the beneficial effect of CIMT. The present study assessed the effects of mCIMT, ICR and CR therapeutic outcomes 2 and 4 weeks after intervention in patients with acute/subacute stroke.
The main result of this study is that improvement in motor function of the affected upper extremity did not differ significantly between patients who received mCIMT and those who received ICR. Regarding both the FA measure and median time (log), only the mCIMT group showed a significant correlation between the initial values and those 2 and 4 weeks after treatment. This suggests that only the mCIMT intervention had a systematic effect among patients, affecting all of them to a similar extent, and this effect was maintained even after 4 weeks of treatment. According to our knowledge, this result has not been reported previously for a patient population with characteristics similar to those of our sample. Patients receiving mCIMT had an apparent advantageous trend in their rehabilitation over those who received CR, whereas this trend was not seen when comparing ICR with CR. Clinically, these data support the idea that mCIMT effects are not only seen early in treatment (2 weeks after), but they are seen consistently among all patients even after 4 weeks, suggesting a very robust therapeutic effect. Thus, even though we did not observe statistically significant differences between ICR and mCIMT, we would recommend mCIMT over ICR intervention, given that the effect of mCIMT was better than CR, whereas ICR did not show such an advantage. In addition, mCIMT had systematic positive effects both 2 and 4 weeks after onset. Given that patients were in the early phase of recovery after stroke, it is not surprising that even those assigned to the CR group improved their performance. This makes the difference between mCIMT and CR even more remarkable.
Two systematic reviews investigated the impact of intensity of practice after stroke (28, 29). In Kwakkel et al’s (28) first review, the results support the hypothesis that augmented exercise therapy has small, but favourable, effects on ADL, particularly if therapy input is augmented at least 16 h within the first 6 months after stroke. Although there is strong evidence that early augmented exercise therapy time (expressed as time dedicated to practice) may enhance functional recovery, there is a discrepancy between the evidence for the benefits of intensive practice (28). Two studies have explored the effect of increased intensity of practice on arm function after stroke; however, both studies failed to find the differences in outcome between the intervention and control groups. In other words, increased intensity of practice for arm impairment after stroke does not appear to improve recovery of arm function (30, 31). The total augmented time of practice in the above 2 studies was less than 16 h (10 h and 15 h, respectively), therefore such findings may be due to the diminished intensity of the interventions. Wolf et al. (19) examined the relationship between the change scores on the log-mean Wolf Motor Function Test (lmWMFT) and the intensity of the supervised CIMT in participants with subacute and chronic stroke. The intensive training incorporates elements of repetitive task practice and adaptive task practice, also called shaping. They found that there was no relationship between intensity of treatment and the log-mean WMFT scores both in the immediate (3–9 months post-stroke) and the delayed group (1 year later). They suggested that functional improvements observed in the Exercise Intensity Trial might be attributable to training components other than the designated ratio of training approaches (adaptive and repetitive task practice) (32). However, they only explored the relationship between the intensity and lmWMFT; the difference in outcome of lmWMFT between low and augmented intensity was not analysed. Sterr et al. (13) investigated the effects of 3-h vs 6-h daily training sessions in CIMT. They found that the 3-h CIMT training schedule significantly improved motor function in chronic hemiparesis, but that it was less effective than the 6-h training schedule. In our study, there was a trend towards significance for the difference between the ICR and CR groups. We think that the intensive therapy plays an important role in CIMT, but in and by itself it is not an adequate explanation for the treatment success of CIMT. To obtain a favourable effect, the augmented time of intensive training should be at least 16 h within the first 6 months after stroke.
The use of the constraint on the patients’ unaffected arm raises many ethical issues. Investigations assessing the efficacy of the constraint element are therefore important, because this may inconvenience the patient, and it also requires clinician’s time and resources. Uswatte et al. (33) examined the effects of the type of training (task-practice, shaping) and restraint (sling, half-glove, no restraint) on treatment outcomes. The type of motor training (shaping, task-practice) and the physical restraint of the less-impaired arm (sling/hand-splint assembly, half-glove, no device) did not appear to be critical therapeutic factors with respect to immediate treatment outcomes. Task-practice with the more-impaired arm and physical restraint of the less-impaired arm during CIMT therapy, however, may have been important for retention of gains in long-term follow-up (32). In a recent study (34), stroke patients were randomized to mitt use or no mitt use on the less-affected hand for 90% of waking hours for 12 days. All patients received 3 h of arm and hand training per day for 2 weeks. As a result, no effect of using a restraint in patients with subacute stroke was found. When examining the effect of extended mitt use in a group of patients with chronic stroke, significant improvements in arm function were observed after 2 weeks of mCIMT group, but no further improvements could be demonstrated after an extended mitt use for another 3 months (35). In our study, improvement in motor function of the affected upper extremity did not differ significantly between patients who received mCIMT and those who received ICR. Taking CR as reference for comparison, mCIMT showed an apparent advantageous effect, whereas ICR did not. These findings indicate that restraint components in mCIMT may be minor compared with the intensity of the training. In fact, all the patients in our study were encouraged to use their affected upper extremity in their daily activities. They were aware of the importance of using the affected upper extremity to improve arm motor functions. This awareness may have had a similar effect to that of the restraint component in mCIMT to some extent and it may limit the need to restrain the unaffected upper extremity.
According to the findings in the present and previous studies, we believe that both intensive therapy and the restraint component contribute to the effect of mCIMT, but that the intensive therapy plays an important role. To obtain a beneficial effect of intensive therapy, the augmented time must accumulate to at least 16 hours within the first 6 months after stroke. If it is difficult to follow the mCIMT regimen in clinical practice, augmented practice, plus encouraging patients to use their affected arm in daily activities, may improve the function of the affected arm and hand motor performance.
Conclusion and limitations
The results of this study show that mCIMT had better therapeutic effects on improving the motor function of acute and subacute stroke patients than CR therapy. No statistically significant differences were observed between the results of mCIMT and ICR intervention. However, given that mCIMT was different from CR, whereas ICR was not, and that the mCIMT had a systematic effect both 2 and 4 weeks after the onset of treatment, unlike the other 2 forms of therapy, we would recommend mCIMT over ICR intervention. One limitation of the study, besides the small sample size, is that patients were in the early phase of recovery after stroke, during which significant improvements are expected even among those in the CR group. However, we believe that this makes the observed difference between mCIMT and CR even more remarkable and clinically relevant.
Acknowledgements
This research was supported by a grant from the Ministry of Human Resources and Social Security of the People’s Republic of China. We are indebted to our staff for their help in training patients and to Jing-li Zhao for his assessment of patients.
References