OBJECTIVE: To investigate the sustained effect of a rehabilitation programme for patients with ankylosing spondylitis, and to compare the effect of this intervention given in a Mediterranean vs a Norwegian setting.
METHODS: A total of 107 patients with ankylosing spondylitis applying for rehabilitation were randomized to a 4-week inpatient rehabilitation programme in a Mediterranean country or in Norway. The participants were evaluated clinically before and after the rehabilitation period (week 0 and 4) and in week 16. The ASsessments in Ankylosing Spondylitis working group’s Improvement Criteria (ASAS-IC), and tests of spinal mobility and physical capacity were used to measure treatment response.
RESULTS: An ASAS20 improvement was still present at week 16 in 50% of the patients treated in a Mediterranean and 23% in a Norwegian centre (p = 0.006). The tests of spinal mobility, physical capacity, and almost all patient’s assessments of health status (ASAS-IC components) were still improved at week 16 after therapy in both climatic settings. While the improvements in physical capacity were comparable, the spinal mobility and ASAS-IC components improved more, and improvements were sustained longer, after rehabilitation in a Mediterranean setting.
CONCLUSION: Patients with ankylosing spondylitis benefit from a 4-week rehabilitation programme in Norway, but even more so from a similar programme in a Mediterranean setting.
Key words: ankylosing spondylitis; climate; rehabilitation; physical therapy modalities; treatment outcome; randomized controlled trials.
J Rehabil Med 2011; 43: 534–542
Guarantor: Yndis A. Staalesen Strumse, Section for Climate Therapy, Department of Rheumatology, Oslo University Hospital, Rikshospitalet, PO Box 4950 Nydalen, 0424 Oslo, Norway. E-mail: yndiss@medisin.uio.no, ystrumse@ous-hf.no
Submitted May 24, 2010; accepted February 21, 2011
INTRODUCTION
Ankylosing spondylitis (AS) is an inflammatory rheumatic disease that affects the axial skeleton, causing characteristic inflammatory back pain, stiffness, and often peripheral arthritis. The prevalence of AS is between 0.1% and 1.4% in Europe (1).
Physiotherapy and supervised exercise are widely accepted as part of the non-pharmacological treatment of patients with AS. However, the awareness of published evidence on physiotherapy in AS is unsatisfactory (2, 3). A Cochrane Review summarizing the available scientific evidence on the effectiveness of physiotherapy in the management of AS concludes that an individual home-based or supervised exercise programme is better than no intervention; that supervised group physiotherapy is better than home exercises; and that combined inpatient spa-exercise therapy followed by group physiotherapy are better than group physiotherapy alone (4).
Patients with AS report variation in health status according to season and weather conditions (5). High doses of ultraviolet radiation may induce immunosuppression (6). Low temperature and low atmospheric pressure increase the risk of joint pain in rheumatic patients (7) and intensify pain in arthritic rats (8). An increase in pain and rigidity were associated with both decreased temperature and increased relative humidity in patients with arthritis in Aikman’s study (9).
Climatotherapy is the use of climatic factors for therapy according to Gutenbrunner et al. (10). Climatotherapy includes the planned medical application of climatic factors that are effective for the prevention or treatment of diseases. Climatotherapy is performed in specific climates, e.g. high-altitude climates, sea coastal climates, and includes changes in climatic environment. Climatic factors with relevance for therapy are radiation (ultraviolet, light, infrared), thermal stimuli (temperature, wind, humidity, etc.) and air composition (pO2, therapeutic aerosols, absence of pollution and allergens, etc.). Psychological reactions from the experience of landscapes may also be a factor (10).
When a comprehensive rehabilitation programme is offered in a stable, warm, sunny and dry climate, climatotherapy is supposed to be part of the intervention. However, the main interventions offered through the Section for Climate Therapy are intensive physiotherapy, spa therapy and “self-management” group therapy (11). No previous controlled study has evaluated the efficacy of physiotherapy in a warm compared with a cold climatic setting for patients with AS. However, patients with RA participating in the same study did benefit more from rehabilitation in a warm than a cold climatic setting (12). Some uncontrolled studies have reported sustained improvements in self-reported health status after 3–6 months (13–16). Hashkes (17) found 60% responders to climatic therapy using the ASAS criteria for improvement (IC), but this study did not include any follow-up.
The current study was conducted to compare the sustained effect of a 4-week rehabilitation programme for patients with AS in a Mediterranean and a Norwegian setting, using the ASsessments in Ankylosing Spondylitis (ASAS) international working group’s core sets for physical therapy (PT) interventions (3), the ASsessments in Ankylosing Spondylitis working group’s Improvement Criteria (ASAS-IC)(18) and objective tests of physical capacity.
MATERIAL AND METHODS
Eligibility
A total of 107 patients with AS were recruited from the applicants to a rehabilitation programme in a Mediterranean country, administered by the Section for Climate Therapy at Oslo University Hospital, Rikshospitalet or from the applicants to the North Norway Rehabilitation Centre (RNNK) in Tromsø. The main inclusion criteria were: a diagnosis of AS (verified by a rheumatologist); a documented need for rehabilitation; age below 70 years; and reduced physical functioning, but ability to handle primary activities of daily living (P-ADL) without assistance. Eligible patients should not have attended a similar rehabilitation programme within the last 9–12 months before the intervention. Patients with concomitant diseases that might influence the effect of the rehabilitation programme were excluded: unstable heart, lung or endocrinological diseases, apoplexia cerebri, cancer, mental illness and any kind of abuse problem, in particular. The inclusion of patients was performed according to the doctor’s application and enclosed medical records.
Study design
The study was a randomized, controlled, parallel group trial. All eligible patients were invited to participate. Those accepting the invitation were randomly assigned to a 4-week rehabilitation programme in Norway (North Norway Rehabilitation Centre (RNNK) in Tromsø or Skogli Rehabilitation Centre AS in Lillehammer), or to a similar treatment in a Mediterranean country (Institute Igalo in Montenegro or Balcova Thermal Therapy Centre in Izmir, Turkey). Randomization was performed by a statistician with the Splus language for data analysis, and was stratified according to sex and type of articular involvement (axial/peripheral). The study period lasted from March 2003 until June 2004.
The participants were examined immediately before (week 0) and after (week 4) the intervention period. Three months later (week 16), all participants were re-examined at the Department of Rheumatology at Oslo University Hospital, Rikshospitalet or at the University Hospital of North Norway (UNN), Tromsø. The patients assessed their own health status using the visual analogue score (VAS) scales and indexes described in the outcome measures at week 0, 4, 16, and 28.
Intervention
Participants followed the regular rehabilitation programmes at all centres. The main components of the therapy offered were individualized physiotherapy with exercises, group exercises, passive therapy, relaxation, and patient education. The physiotherapy programme was mainly offered indoors from 08.00 h to 16.00 h 5 days a week.
Active physiotherapy. Individualized physiotherapy was given once daily on a couch, in the fitness department using specially constructed equipment, or in the pool (30 min daily in Balcova and in Tromsø, 30–60 min 4 times a week in Lillehammer, and for 20–30 min maximum 8 times a week in Igalo). Group training (8–15 patients) was given twice daily: in the gym and in a temperature-controlled swimming pool: 45+45 min daily in Balcova, 30+30 min daily in Tromsø and Lillehammer, with additional 60 min 2 times a week in Lillehammer, and in Igalo for 30+20 min 7 and 5 times a week, respectively. Additional, individual training was recommended at all therapy centres, in Lillehammer this was included as part of the compulsory programme 60 min daily.
The exercise therapy aimed at increasing endurance, mobility, and strength. While the Norwegian programme included more endurance training, the Mediterranean programme had more focus on mobility. The patients were given the opportunity to attend additional, voluntary, physical activities at all treatment centres. This programme varied across the different therapy centres, and the proportion of attending patients was higher at the Norwegian centres.
Passive therapy. This therapy comprised thermotherapy, massage, and electrotherapy. At the Mediterranean centres (thermo-)mineral water was used for balneotherapy in the swimming pools, bubble baths, and underwater massage. Two passive treatments of 10–15 min a day were usually given to each patient. At the Norwegian centres, patients received passive therapy only when this was indicated by the physiotherapist.
The programme included a 30–45-min supervised relaxation session 2–4 times a week at Lillehammer, Tromsø, and Balcova. At Institute Igalo activities such as yoga and tai-chi were offered.
Patient education. Disease-specific lectures about AS were given at all 4 centres, focusing on diet, physical activity, self-efficacy, coping techniques, and advice related to general health.
Medical treatment with disease-modifying anti-rheumatic drugs (DMARDs) was kept constant during the intervention and follow-up. However, disease-related adjustments were allowed.
Daylight and climate
The study period in the warm climate was in May–June 2003 at Institute Igalo in Montenegro and September–October 2003 at Balcova Thermal Therapy Center in Izmir, Turkey, both located by the Mediterranean Sea. Mean daylight time was 14 h and 59 min in Igalo and 11 h and 51 min in Balcova, computed using National Mapping Division’s sunrisenset program, version 2.2. The morning temperature in Igalo ranged from 15.6°C to 30.4°C, mean 24.4°C, and in Balcova from 15.0°C to 26.0°C, mean 20.1°C, measured at 08.00/07.30 h at the Therapy Centre. The mean number of days with precipitation above 1.0 mm during each 4-week rehabilitation period was 2 days in Igalo and 1 day in Balcova.
The study period in Norway was from March to May and from September to December 2003. The patients living in the northern parts of Norway received their rehabilitation programme at RNNK in Tromsø, which is located on the northern Norway coastline, while the patients living in the southern parts received their rehabilitation programme at Skogli in Lillehammer, which is located in the inland area. Mean daylight time was 12 h and 46 min in Lillehammer and 15 h and 41 min in Tromsø. The morning temperature in Lillehammer ranged from –9.3°C to 11.8°C, mean 1.7°C and in Tromsø from –6.0°C to 14.9°C, mean 3.0°C measured at 07.00 h at the Norwegian Meteorological Institutes. The mean number of days with precipitation above 1.0 mm during each 4-week rehabilitation period was 7.5 days in Lillehammer and 12.0 days in Tromsø.
Outcome measures
The patients were assessed for lumbar spinal mobility by the original Schober test: the increase with forward flexion of a 10 cm segment with the inferior mark at the level of the posterior superior iliac spines (19), and lateral lumbar flexion: the difference between the fingertips-to-floor distance in the upright position and at maximum lateral flexion (20). The medical examinations included chest expansion: the difference in the chest circumference between full expiration and full inspiration at the 4th intercostal space (21) and erythrocyte sedimentation rate (ESR, mm). Exercise capacity was measured by the 6-minute walk test (6MWT) (22), and physical capacity was measured by the timed-up-and-go (TUG) (23). The total TUG distance was 20 m, this walking distance and time were measured to calculate walking pace. The same assessor performed the medical examinations on the same patient throughout the whole study period.
The patients assessed their own health status by: patient’s global assessment of disease activity (VAS 0–10 cm), fatigue (VAS 0–10 cm), Bath Ankylosing Spondylitis Disease Activity Index (BASDAI) (24, 25), and Bath Ankylosing Spondylitis Functional Index (BASFI) (26, 27). The BASDAI index is a comprehensive self-administered instrument for assessing disease activity in AS. It consists of 6 10-cm VAS to measure severity of fatigue, spinal and peripheral joint pain, localized tenderness and morning stiffness (both qualitative and quantitative). The BASFI is a self-assessment functional index consisting of 8 specific questions regarding function in AS and 2 questions reflecting the patient’s ability to cope with everyday life. Each question is answered on a 10-cm VAS, the mean of which gives the BASFI score (0–10).
The ASAS-IC were used to measure treatment response. An ASAS20 improvement is ≥ 20% relative improvement and absolute improvement of ≥ 1 unit (on a scale of 0–10) in 3 or more of the following 4 domains: patient’s global assessment, patient’s perception of pain (question 2 of the BASDAI), inflammation (mean of question 5 and 6 of the BASDAI), and function (BASFI), with no worsening by ≥ 20% and ≥ 1 unit in the remaining domain (18). ASAS40 improvement was defined as attaining a ≥ 40% relative improvement and an absolute improvement of ≥ 2 units in 3 or more of the 4 domains, with no deterioration from baseline in the remaining domain (28).
The response at week 16 was chosen as a main outcome to evaluate sustained effect.
Ethics
The Regional Ethics Committee and The Norwegian Social Science Services/ Data Inspectorate approved the study, and written, informed consent was obtained from all participating patients.
Statistics
Sample size calculation was done on the basis of a zero hypothesis (H0) about no differences in the efficacy of rehabilitation in a Mediterranean or a Norwegian setting. A power of 80% was chosen, which means 80% probability to ascertain a difference and chose the alternative hypothesis (H1), when true. The chosen level of significance was 5%, thus the H0 was discarded for p-values < 0.05. The sample size calculation was based on a minimum clinically significant difference (MCSD) of 0.9 and 2.2 in standard deviation (SD) of the patient’s assessment of pain (VAS; 0–10 cm) measured in a population of rheumatic patients, and estimated 100 participants necessary in each group to detect this difference as significant. Sample size was calculated with the Sample power programme, and statistical analyses were undertaken with the SPSS version 13.0.
Age, years of education, disease duration and daily prednisolone dose are considered to be normal distributed continuous variables, all other data presented in Table I are of binomial, categorical nature. All patient’s assessments in Table II are uncategorized VAS scales considered to be of continuous nature, all baseline values except fatigue show normal distribution. All measures of spinal mobility and tests of physical capacity are normal distributed, continuous parameters, while the ESR value is continuous, but not normal distributed at baseline (Table III).
|
Table I. Baseline characteristics for ankylosing spondylitis patients receiving rehabilitation in a Mediterranean country or in Norway
|
|
|
Mediterranean
group
n = 65
|
Norwegian group
n = 42
|
|
Demographic data
|
|
|
|
|
Female sex, n (%)
|
27 (42)
|
19 (45)
|
|
|
Age, years, mean (SD; range)
|
48 (10; 28–70)
|
51 (8; 30–62)
|
|
|
Married or living with a partner,
n (%)
|
51 (79)
|
30 (71)
|
|
|
Years of education, mean (SD; range)
|
13 (3; 8–20)
|
12 (3; 7–17)
|
|
|
Employed full-time/part-time, n (%)
|
30 (46)/9 (14)
|
20 (48)/6 (14)
|
|
|
Once on sick leave during last 6 months, n (%)
|
17 (47)
|
14 (58)
|
|
Disease characteristics
|
|
|
|
|
Disease duration, years, mean (SD; range)
|
17 (10; 1–43)
|
18 (9; 3–33)
|
|
|
HLA-B27 positive, n (%)
|
57 (88)
|
38 (93)
|
|
|
Co-morbidity, n (%)
|
|
|
|
|
Hypertension
|
12 (19)
|
13 (31)
|
|
|
Metabolic disorders
|
8 (12)
|
2 (5)
|
|
|
Other diseasesa
|
7 (11)
|
6 (14)
|
|
Baseline drugs
|
|
|
|
|
NSAIDs or coxibs daily/when needed, n (%)
|
37 (58)/20 (31)
|
26 (62)/10 (24)
|
|
|
Analgesics daily/when needed, n (%)
|
6 (9)/42 (65)
|
4 (10)/19 (46)
|
|
|
DMARDs, n (%)
|
7 (11)
|
13 (33)*
|
|
|
Prednisolone, n (%)
|
4 (6)
|
9 (24)*
|
|
|
Daily prednisolone dose, mg, mean (SD; range)
|
5 (4; 2.5–10)
|
5
|
|
|
Biological treatment, n (%)
|
1 (2)
|
3 (9)
|
|
aCoronary artery disease (n = 3), renal diseases (n = 3), migraine (n = 3), asthma bronchiale (n = 2) and cancer (n = 2).
*p ≤ 0.01 vs patients treated in the Mediterranean group.
NSAID: non-steroidal anti-inflammatory drug; DMARD: disease-modifying anti-rheumatic drug; coxibs: cyclo-oxygenase-2 inhibitors; SD: standard deviation.
|
Table II. Responses in patient’s assessments of health status at 4, 16 and 28 weeks after initiation of rehabilitation (VAS; 0–10 cm)
|
|
Baseline values
|
Changes from baseline
|
|
Week 4
|
p-value
|
Week 16
|
p-value
|
Week 28
|
p-value
|
|
ASAS-IC component
|
|
|
|
|
|
|
|
|
|
Patient’s global
|
|
|
|
Mediterranean group
|
5.4 (2.0)
|
–3.7 (2.2)
|
< 0.001
|
–2.1 (2.6)
|
< 0.001
|
–1.5 (2.6)
|
< 0.001
|
|
|
|
Norwegian group
|
5.0 (1.9)
|
–1.7 (1.9)
|
< 0.001
|
–1.2 (2.2)
|
0.004
|
–0.5 (2.5)
|
0.630
|
|
|
|
Difference between the groups
|
|
|
< 0.001
|
|
0.073
|
|
0.069
|
|
|
Spinal pain (BASDAI 2)
|
|
|
|
|
|
|
|
|
|
|
Mediterranean group
|
6.2 (2.0)
|
–4.2 (2.5)
|
< 0.001
|
–2.3 (3.2)
|
< 0.001
|
–1.4 (2.3)
|
< 0.001
|
|
|
|
Norwegian group
|
5.8 (1.8)
|
–1.9 (1.9)
|
< 0.001
|
–0.8 (2.3)
|
0.081
|
–0.3 (2.3)
|
1
|
|
|
|
Difference between the groups
|
|
|
< 0.001
|
|
0.007
|
|
0.035
|
|
|
Morning stiffness (BASDAI 5 and 6)
|
|
|
|
|
|
|
|
|
|
|
Mediterranean group
|
4.9 (2.3)
|
–3.1 (2.1)
|
< 0.001
|
–2.2 (2.2)
|
< 0.001
|
–1.7 (2.2)
|
< 0.001
|
|
|
|
Norwegian group
|
5.0 (2.0)
|
–1.8 (1.6)
|
< 0.001
|
–1.2 (2.2)
|
0.004
|
–0.6 (2.0)
|
0.180
|
|
|
|
Difference between the groups
|
|
|
0.002
|
|
0.028
|
|
0.026
|
|
|
BASFI
|
|
|
|
|
|
|
|
|
|
|
Mediterranean group
|
4.3 (2.0)
|
–2.6 (1.7)
|
< 0.001
|
–1.3 (1.9)
|
< 0.001
|
–1.0 (1.8)
|
< 0.001
|
|
|
|
Norwegian group
|
4.3 (1.5)
|
–1.2 (1.2)
|
< 0.001
|
–0.5 (1.2)
|
0.029
|
–0.4 (1.2)
|
0.169
|
|
|
|
Difference between the groups
|
|
|
< 0.001
|
|
0.016
|
|
0.085
|
|
BASDAI
|
|
|
|
Mediterranean group
|
5.0 (1.7)
|
–3.3 (1.9)
|
< 0.001
|
–2.0 (2.3)
|
< 0.001
|
–1.3 (1.8)
|
< 0.001
|
|
|
Norwegian group
|
4.8 (1.3)
|
–1.6 (1.3)
|
< 0.001
|
–0.7 (1.7)
|
0.039
|
–0.3 (1.6)
|
1
|
|
|
Difference between the groups
|
|
|
< 0.001
|
|
0.001
|
|
0.004
|
|
Fatiguea
|
|
|
|
Mediterranean group
|
7.0 (3.6, 8.5)
|
–4.2 (2.7)
|
<0.001
|
–2.7 (3.3)
|
< 0.001
|
–2.3 (2.8)
|
< 0.001
|
|
|
Norwegian group
|
6.1 (3.5, 7.4)
|
–1.4 (2.6)
|
0.004
|
–1.5 (2.7)
|
0.004
|
–0.6 (2.9)
|
0.516
|
|
|
Difference between the groups
|
|
|
< 0.001
|
|
0.049
|
|
0.007
|
|
aMedian (25th, 75th centiles).
Baseline values are shown as mean (standard deviation (SD)), unless stated otherwise, and changes from baseline are shown as mean difference from baseline (SD). Number of patients treated was 65 in the Mediterranean group and 42 in the Norwegian group.
ASAS-IC: ASsessments in Ankylosing Spondylitis working groups Improvement Criteria; VAS: visual analogue scale; BASDAI: Bath Ankylosing Spondylitis Disease Activity Index; BASFI: Bath Ankylosing Spondylitis Functional Index.
|
Table III. Responses in spinal mobility, erythrocyte sedimentation rate (ESR) and tests of physical capacity at 4 and 16 weeks after initiation of rehabilitation
|
|
Baseline values
|
Changes from baseline
|
|
Week 4
|
p-value
|
Week 16
|
p-value
|
|
Spinal mobility
|
|
|
Anterior lumbar flexion (Schober), cm
|
|
|
|
|
Mediterranean group
|
3.3 (1.6)
|
0.7 (1.0)
|
< 0.001
|
0.5 (0.9)
|
< 0.001
|
|
|
|
Norwegian group
|
3.2 (1.5)
|
0.1 (0.5)
|
0.273
|
0.2 (0.5)
|
0.005
|
|
|
|
Difference between the groups
|
|
|
< 0.001
|
|
0.038
|
|
|
Lateral lumbar flexion, right, cm
|
|
|
|
|
Mediterranean group
|
8.6 (4.4)
|
4.9 (3.9)
|
< 0.001
|
4.5 (3.8)
|
< 0.001
|
|
|
|
Norwegian group
|
9.9 (5.7)
|
2.3 (3.5)
|
< 0.001
|
1.5 (2.8)
|
0.004
|
|
|
|
Difference between the groups
|
|
|
0.001
|
|
< 0.001
|
|
|
Lateral lumbar flexion, left, cm
|
|
|
|
|
Mediterranean group
|
8.3 (4.5)
|
5.1 (3.7)
|
< 0.001
|
4.7 (3.7)
|
< 0.001
|
|
|
|
Norwegian group
|
9.6 (5.4)
|
2.4 (3.3)
|
< 0.001
|
1.8 (3.1)
|
< 0.001
|
|
|
|
Difference between the groups
|
|
|
< 0.001
|
|
< 0.001
|
|
|
Chest expansion, cm
|
|
|
|
|
|
|
|
|
Mediterranean group
|
3.7 (1.6)
|
0.7 (1.4)
|
< 0.001
|
0.3 (1.5)
|
0.161
|
|
|
|
Norwegian group
|
3.9 (1.9)
|
0.2 (0.8)
|
0.348
|
0.3 (1.1)
|
0.285
|
|
|
|
Difference between the groups
|
|
|
0.023
|
|
0.792
|
|
ESR, mma
|
|
|
|
|
|
|
|
|
Mediterranean group
|
17.0 (10.0, 36.5)
|
1.0 (11.0)
|
0.978
|
–8.3 (10.9)
|
< 0.001
|
|
|
|
Norwegian group
|
12.0 (6.0, 30.5)
|
–3.5 (10.6)
|
0.079
|
–2.5 (10.6)
|
0.332
|
|
|
|
Difference between the groups
|
|
|
0.041
|
|
0.014
|
|
Tests of physical capacity
|
|
|
|
|
|
|
|
6-minute walk test (6MWT), m
|
|
|
|
Mediterranean group
|
559 (84)
|
84 (64)
|
< 0.001
|
68 (65)
|
< 0.001
|
|
|
|
Norwegian group
|
566 (99)
|
61 (53)
|
< 0.001
|
59 (54)
|
< 0.001
|
|
|
|
Difference between the groups
|
|
|
0.071
|
|
0.470
|
|
|
Timed-up and-go (TUG), speed (20 m/s)
|
|
|
|
Mediterranean group
|
1.5 (0.3)
|
0.2 (0.2)
|
< 0.001
|
0.2 (0.2)
|
< 0.001
|
|
|
|
Norwegian group
|
1.5 (0.3)
|
0.2 (0.2)
|
< 0.001
|
0.1 (0.2)
|
0.054
|
|
|
|
Difference between the groups
|
|
|
0.069
|
|
0.116
|
|
aMedian (25th, 75th centile).
Baseline values are shown as mean (standard devaiation (SD)), and changes from baseline are shown as mean difference from baseline (SD), unless stated otherwise. Number of patients treated was 65 in the Mediterranean group and 42 in the Norwegian group.
|
Binomial, categorical variables are presented by numbers (n) and percentages (%), and continuous variables are presented as mean and SD or median and 25th, 75th centiles according to whether the observations show normal distribution. To compare two groups, we used the Pearson χ2 test, or Fisher’s exact test when appropriate, for categorical variables, independent samples t-test for continuous variables with normal distribution, and Mann-Whitney U test for continuous variables without normal distribution.
The clinical response is given as the mean difference from baseline with corresponding SD. All mean differences were of continuous nature and normally distributed, hence paired samples and independent samples t-tests were used for within-group and between-groups analysis, respectively.
Since Bonferroni correction for multiple comparisons presumes independency between the variables tested, and the tests in this study were on the same subjects using highly correlated variables, adjustment for the number of variables was judged to be too conservative (29). However, Bonferroni adjustments for the number of tests between different time-points within a group were done by multiplication of the p-value obtained from each test by the number of paired comparisons done.
RESULTS
Patient disposition
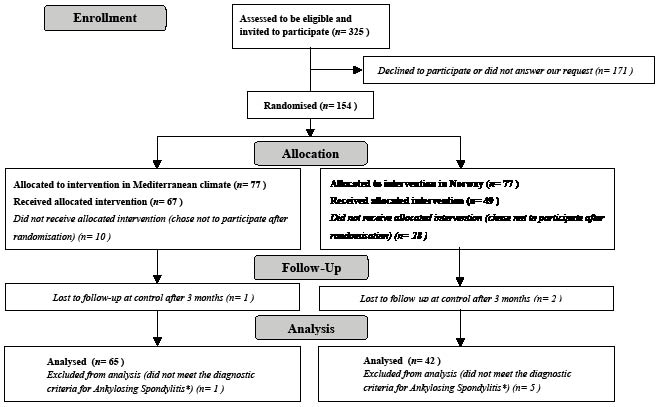
A total of 325 eligible patients with AS were invited to participate (Fig. 1). From these, 154 patients were randomized for treatment in a Mediterranean country, n = 77 or in Norway, n = 77, and 107 patients were analysed as completers, n = 65 in a Mediterranean country (40 in Turkey and 25 in Montenegro) and n = 42 in Norway (13 in Tromsø and 29 in Lillehammer). Further details of the patient flow are presented in Fig. 1.
Fig. 1. Patient flow. Summary of patient disposition, with non-participants in italics (n = 218) (171+10+1+1+28+2+5). *Patients excluded from the analysis did not meet the Modified New York Criteria for Ankylosing Spondylitis (1984) at the first medical examination (30).
The known reasons for withdrawal after randomization and before treatment were: practical considerations (n = 9), dissatisfaction with the randomization result (n = 4), acute trauma/hospitalization (n = 3), responsibility at home (n = 2), or no need for rehabilitation (improved health status) (n = 2). The reasons for withdrawal were comparable whether randomized to rehabilitation in a Mediterranean country or in Norway. Eighteen patients withdrew without giving any reason.
There was no significant difference between the participants (n = 107) (65+42 in the Mediterranean group and Norwegian group, respectively) and the non-participants (n = 218) (171+10+1+1+28+2+5) (see Fig. 1) of this study with regard to age (data not shown), but the proportion of men was higher among the non-participants (69% vs 57%, p = 0.029).
The patients who discontinued after randomization (n = 47) (10+1+1+28+2+5), were comparable to the completers (n = 107) (65+42) regarding age, sex, and type of articular involvement (axial/peripheral) (data not shown). A higher number of patients completed the study among those randomized to the Mediterranean group (n = 65), than those randomized to the Norwegian group (n = 42), (p ≤ 0.001), but the completers of the 2 groups did not differ in regard to age, sex, and type of articular involvement (axial/peripheral) (data not shown).
Patient baseline characteristics
The demographic and disease characteristics were comparable in the 65 patients treated in the Mediterranean setting (42% women, mean age 48 (range 28–70) years) and the 42 patients treated in the Norwegian setting (45% women, mean age 51 (range 30–62) years) (Table I). The number of patients using DMARDs or prednisolone at baseline was lower in the Mediterranean than in the Norwegian group (p = 0.007 and p = 0.011, respectively). However, the baseline values of all outcome measures were comparable (Tables II and III).
Efficacy
Clinical response was expressed as mean difference from baseline at 4, 16, and 28 weeks after initiation of the 4-week rehabilitation programme. Changes in the patient’s assessments of health status are presented in Table II, and the spinal mobility, erythocyte sedimentation rate (ESR), and tests of physical capacity in Table III.
At week 16, all examined variables, except spinal pain (BASDAI 2), chest expansion and ESR, improved significantly among patients in both study groups (Table II and III). The improvements at week 16 were larger for patients treated in Mediterranean countries than for those treated in Norway for all examined variables except for the patient’s global assessment and the tests of physical capacity. After 28 weeks, all patient’s assessments of health status (patient’s global, spinal pain, morning stiffness, BASFI, BASDAI, and fatigue) were still significantly improved in the Mediterranean group (all p ≤ 0.001), but not in the Norwegian group.
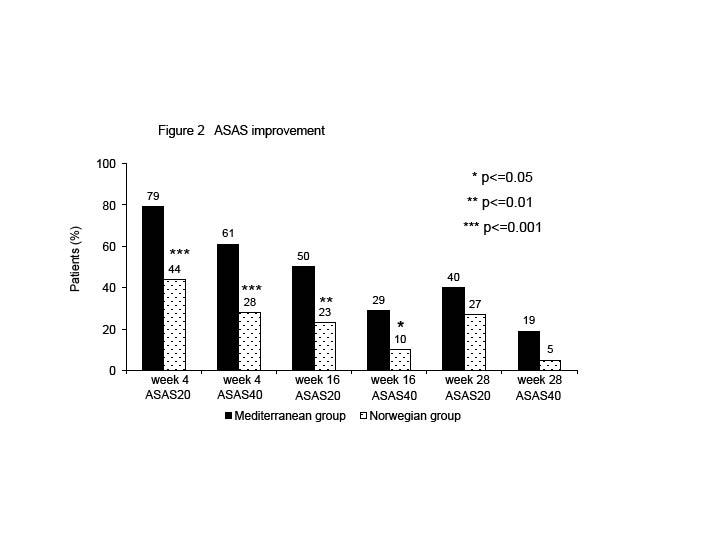
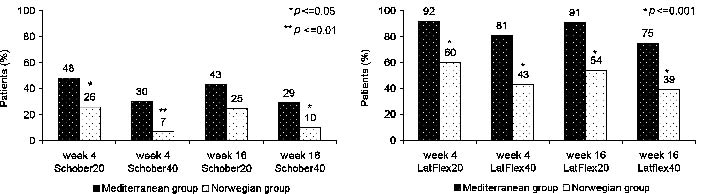
At week 16, the proportion of patients who met the ASAS20 and ASAS40 improvement criteria was 50% and 29% in the Mediterranean group and 23% and 10% in the Norwegian group (p = 0.006 and p = 0.022, respectively) (Fig. 2). The proportion of patients who achieved a 20% and 40% improvement in Schober’s test was 43% and 29% in the Mediterranean group and 25% and 10% in the Norwegian group (p = 0.066 and p = 0.025, respectively) (Fig. 3A). The proportion of patients with 20% and 40% improvement in lateral flexion was 91% and 75% in the Mediterranean and 54% and 39% in the Norwegian group (both p ≤ 0.001) (Fig. 3B).
Fig. 2. ASAS improvement. Values above the bars are the percentages of the patients who met the Assessments in Ankylosing Spondylitis working group’s improvement criteria (ASAS-IC), ASAS20 = 20% improvement and ASAS40 = 40% improvement. The responses are measured at week 4, week 16, and week 28 after initiation of treatment in the Mediterranean (n = 65) or in the Norwegian setting (n = 42). The differences between the groups are marked on the figure.
Fig. 3. Values above the bars are the percentages of the patients who had 20% and 40% improvement in A) anterior lumbar flexion (Schober) and B) lateral lumbar flexion on either the right or the left side. The responses are measured immediately after treatment (week 4) and 16 weeks after initiation of treatment in a Mediterranean centre (n = 65) or in Norway (n = 42). The differences between the groups are marked on the figure.
Medication
Thirty-one (48%) of the 65 Mediterranean group patients and 4 (10%) of the 42 Norwegian group patients had ceased or reduced their use of analgesics during the 4-week rehabilitation period (p ≤ 0.001). Seven patients (11%) had initiated or increased their use of analgesics 16 weeks after initiation of intervention in the Mediterranean group, compared with no patients in the Norwegian group (p = 0.041). There was no statistical difference in the number of patients who initiated/increased or ceased/reduced NSAIDs, DMARDs, biological drugs and prednisolone between the two groups within the study period (data not shown).
DISCUSSION
This study ascertains the effect of a 4-week rehabilitation programme for patients with AS performed either in a Mediterranean or in a Norwegian setting. Close to all patient’s assessments of health status, spinal mobility measures, and tests of physical capacity improved significantly 3 months after completion of the programme (week 16) in both climatic settings. The improvements in the patient’s assessments of health status and spinal mobility measures were larger when the rehabilitation was performed in a Mediterranean country rather than in Norway, while the tests of physical capacity showed comparable improvements in both groups.
The proportion of ASAS20/ASAS40 responders at 16 weeks after the rehabilitation programme was 50%/29% in the Mediterranean group and 23%/10% in the Norwegian group. The immediate (week 4) efficacy in the Mediterranean group (79% ASAS20 responders) was similar to that of anti-tumour necrosis factor alpha (TNFα) therapy previously found for patients with AS (31).
The obtained effects of the rehabilitation programme declined over time, in contrast to the continuous anti-TNFα therapy. This concurs with the uncontrolled study of Lubrano et al. (32), being the first to evaluate the effectiveness of a 3-week intensive rehabilitation programme by the ASAS response criteria. It is not known whether repeated rehabilitation periods would have an additive efficacy in patients with AS.
Brandt et al. (28) have suggested including spinal mobility and acute phase reactants to the original 4 domains ASAS-IC, which are a composition of patients’ health assessments. Schober’s test and thoracolumbar lateral flexion have proved to be among the most valid measures of spinal mobility, shown as significant correlations with radiological sum scores (33).
The participants in our study had both restricted anterior (Schober’s test) and lateral lumbar flexion, as well as chest expansion at baseline, when compared with normal values (19–21). The mean improvements in the Schober’s test of this study span from 0.1 to 0.7 cm, which are comparable to other studies of different exercise programmes for patients with AS (34, 35). In the study of Altan et al. (34), Schober improved from 3.19 to 3.65 cm after 3 weeks of intensive treatment, including daily balneotherapy and home exercises. This intervention was followed by a 30-min home exercise programme for 6 months, improving the mean Schober value to 4.12 cm in the intervention group. Pile et al. (36) have calculated the mean inter-observer variation to be 0.7 cm and the mean intra-observer variation to be 0.6 cm for the modified Schober’s test. The high degree of variation between each measure in individual patients makes it difficult to define the observed improvement to be of any clinical significance. According to Viitanen (33), the Schober’s test is both a valid and reliable measurement, but not very sensitive to change. When using measures insensitive to change, Felson et al. (37) recommend defining change on an individual basis, focusing on enumerating which patients improve in a trial, rather than on the mean level of improvement. Therefore, the fact that the percentage of patients achieving 20%/40% improvement in Schober was 43%/29% in the Mediterranean group and 25%/10% in the Norway group might be more illustrative than the mean change for the efficacy 16 weeks after initiation of intervention in this study.
Lateral lumbar flexion is a responsive measure judged by a high standardized response mean (0.84), and has been recommended among the spinal mobility measures (28). This concurs with our findings, and the percentage of patients having 20%/40% improvement in lateral flexion remained high at week 16: 91%/75% in the Mediterranean group and 54%/39% in the Norway group.
The obtained improvements in spinal mobility seem to be more stable than the ASAS improvements in this study. This might indicate that an intensive rehabilitation programme could postpone the stiffening process in the spinal column of patients with AS. According to Lubrano et al. (38), rehabilitation was superior to anti-TNFα therapy for improvements in anthropometric measures. Therefore, physiotherapy and physical exercise may be a substantial supplement to medical treatment in order to improve mobility in patients with AS. Warm and stable climatic conditions may enhance rheumatic patients’ capacity to perform physical exercise (15), and this might explain why the improvements were larger when the rehabilitation was performed in a Mediterranean setting.
The tests of physical capacity showed sustained, comparable improvements after 16 weeks for both patient groups. The mean change in the 6MWT is judged to be of clinical significance when compared with studies of patients with respiratory diseases (39). The improvements in TUG confirmed that the patients had improved their walking pace.
Methodological considerations
This study has some methodological limitations that have to be taken into consideration. More patients dropped out before the study started in the Norwegian group than in the Mediterranean group. This may have influenced the comparability of the two groups. The significantly higher percentage of patients using DMARDs and prednisolone in the Norwegian group at baseline (Table I) might indicate biased groups. However, the number of patients using this medication is low in both groups, and the number of patients that constitute the difference in DMARDS and prednisolone users, was only 6 and 5, respectively. Whether this difference is made by random, or as a real selection toward more affected patients in the Norwegian arm, might be an object of discussion. However, the baseline values of all outcome measures were comparable (Table II and Table III).
The fact that the actual sample size was lower than the calculated one does not seem to reflect the ability to detect statistical significant differences between the two groups in this study. The actual mean difference observed in the VAS spinal pain score at week 16 (Table II) was (–2.3 –(–0.8) = –1.5 cm), which is a larger value than the MCSD at 0.9 cm used to calculate the number needed to treat prior to study start. Thus, our assumption about differences in improvement was modest compared with the real power of this study.
Rehabilitation implies a multifactorial approach to a problem, or more often a complexity of problems associated with a disease or a trauma. The complexity of both patient problems and the modalities of intervention has resulted in more outcome measures in our study than recommended in a statistical view. In the theory, every 20th parameter is supposed to show a significant change by chance, when the chosen level of significance is set to be 0.05. Bonferroni adjustments for the number of tests between different time-points within a group have been done. But since Bonferroni correction for multiple comparisons presumes independency between the variables tested, and the tests in this study were on the same subjects using highly correlated variables, adjustment for the number of variables has been judged to be too conservative (29). However, the possibility that a statistically significant change may appear by chance is important to bear in mind when interpreting the results, which in turn increases the timeliness of an additional evaluation of clinical importance.
The climatic condition was a main difference between the Mediterranean therapy and the Norwegian therapy given in this study, but we cannot ignore that the rehabilitation programmes had some differences even though the main components were similar. The Norwegian programme tended to focus more on endurance training and the Mediterranean programme more on mobility. Passive therapy including balneotherapy was given on a larger scale in the Mediterranean than in the Norwegian centres. These differences in the physiotherapy programmes weaken the validity of a conclusion about the potential climatic influence in our study. Nevertheless, when the patients benefit more from the “Mediterranean package”, this might be the most interesting fact for patients, their medical therapists, and the health economy.
The evidence about the different components of a comprehensive rehabilitation programme differs. Uhlig et al. (40) have reviewed the effectiveness of comprehensive rehabilitation programmes, concluding that when effects on the various outcome measures are demonstrated, improvements can only with difficulty be attributed to a specific component of a comprehensive programme. Thus, the overall performance of comprehensive rehabilitation programmes, not the individual components, should be evaluated. Accordingly, our conclusion about the differences in efficacy of rehabilitation in warm and cold climatic settings must take the overall performance of the comprehensive rehabilitation programme into account, not only the relationship between climatic conditions and AS.
In conclusion, patients with AS had a sustained positive effect of a 4-week rehabilitation programme both in a Mediterranean and in a Norwegian setting. The improvements in the patient’s assessments of health status and spinal mobility measures were larger and better maintained at least 3 months after rehabilitation in a Mediterranean setting, while the improvements in physical capacity were comparable between the two groups. Future studies are needed to ascertain the most important contributing factors to these differences. Our findings support the ASAS/EULAR recommendations of non-pharmacological therapy (including education, exercise and physiotherapy) as an important part of the management of AS (3).
ACKNOWLEDGEMENTS
The authors are grateful to all persons participating in the study. We thank Karin Øien Forseth, MD, PhD, and Gunnstein Bakland, MD, for assistance with the data collection, Marianne Strand Svendsen for coordinating the participants, consultant Johan Kofstad at the Department of Medical Biochemistry for help with the blood tests analysis, and Biostatistic Unit at Oslo University Hospital, Rikshospitalet for help with the statistics.
Funding
This study was financed by the Section for Climate Therapy, Department of Rheumatology at Oslo University Hospital, Rikshospitalet, and supported by a grant from the Norwegian Foundation for Health and Rehabilitation via the Norwegian Rheumatism Association.
Competing interests
None declared.
REFERENCES