OBJECTIVE: To evaluate the activity and participation levels of adults with spastic diplegia 17–26 years after selective dorsal rhizotomy; to investigate relationships between subjects’ functioning and age, socio-economic-status, level of satisfaction and their perceptions of the post-operative outcomes.
DESIGN: Observational follow-up study.
Patients: Thirty-one subjects with spastic diplegia, age range 21–44 years, who underwent selective dorsal rhizotomy between 1981 and 1991.
METHODS: A semi-structured interview was used to gather data on patients’ characteristics and long-term experiences after the operation. The Functional Mobility Scale and Life-Habit questionnaire were completed.
RESULTS: Based on the Functional Mobility Scale 84% of subjects were reported as independent for a distance of 5 m, and 61% for 50 and 500 m. Eighty percent were independent in accomplishing all life habits, with most problems found for Mobility and Recreation. This was in agreement with the subjects’ perception, with strong correlations between Life-Habit questionnaire accomplishment and satisfaction levels. No significant associations were found between functioning and age at selective dorsal rhizotomy, current age and socio-economic status.
CONCLUSION: More than 15 years after selective dorsal rhizotomy, adults with spastic diplegia showed high levels of functioning, and similar levels of satisfaction with life habits. The majority had positive feelings about the neurosurgical procedure, although there is a need for better follow-up after subjects leave school.
Key words: cerebral palsy; dorsal rhizotomy; ICF model; activity; participation; function; mobility.
J Rehabil Med 2011; 43: 330–337
Correspondence address: Nelleke G. Langerak,Division of Physiotherapy, Faculty of Health Sciences, Stellenbosch University, South Africa. E-mail: nellekelangerak@hotmail.com
Submitted January 7, 2010; accepted October 29, 2010
INTRODUCTION
Cerebral palsy (CP) is the most common cause of physical disability in childhood, with approximately 80% of children classified with pyramidal (spastic) syndrome (1). CP cannot be cured, but biomedical, (re)habilitative and surgical interventions can prevent secondary abnormalities and improve functional abilities and quality of life (2). One of the treatment options to ameliorate the patients from the disabling spasticity is the neurosurgical procedure known as selective dorsal rhizotomy (SDR).
SDR entails cutting a fraction of the nerve rootlets in the lower spine, thus interrupting the abnormal reflex circuit that gives rise to uncontrolled spasticity. This procedure was first described almost 100 hundred years ago by Foerster (3), and reintroduced by Peacock (4) in the 1980s, who moved the site of rhizotomy from the conus medullaris region to the cauda equine. After the relocation of Peacock from Cape Town, South Africa, to Los Angeles, USA, SDR gained acceptance and is now used around the world (5).
The International Classification of Function, Disability and Health (ICF) model (6) provides a biopsychosocial framework to identify and quantify the effects of interventions particularly in clinical trials (7, 8) and has been shown to be useful in the field of CP (2, 9). Based on the different domains of this model, Steinbok (10) reported in his review article strong evidence of improvement in impairments and gross motor function based on randomized control studies, while good evidence for benefits in performance of daily activities during the first few years after SDR was reported as a result of some cohort studies.
As CP is the result of a non-progressive disturbance to the developing brain (11), it could be assumed that the short-term benefits from SDR as demonstrated by many studies (10) are maintained with ageing. However, it has been shown in people with CP (who did not receive SDR) that, as they become older, they may experience various secondary complications, which can result in, for example, decreased walking abilities (12, 13) and general limitations in activity levels and negative influences on their quality of life (14–16). In addition, age at time of surgery might have an influence on the level of functional deterioration, and the influence of environmental factors should not be underestimated (17). Long-term outcome studies are essential to guide future decisions in healthcare, education and social services (9).
Our research team has reported on long-term outcomes in the domains of body structure and function and the specific activity of mobility in a test setting (18–21). However, there is a difference between what children can do in such standardized, controlled environments (capacity), what they can do in their daily environment (capability), and perhaps most importantly, what they do in their daily environment (performance) (22). Therefore, the question remains: What are the long-term outcomes of SDR in adults with CP for the domains of activity (performance-level) and participation?
Tools that comprehensively measure levels of performance in the domains of activity and participation were reviewed by Resnik & Plow (23). They investigated 40 measures, and selected 5 questionnaires that linked questions to the 9 domains of the ICF model: Activity and Participation. The Life-Habit questionnaire (LIFE-H) was one of the selected questionnaires documenting the manner in which people carry out daily activities and social roles (accomplishment level), and evaluating their perception regarding the level of participation achieved (satisfaction level), with the interaction of personal and environmental factors (24).
The quality of activity performance in people with CP is often dependent on their functional mobility. Functional mobility can be defined as the manner in which people are able to move around in the environment in order to achieve daily activities and interact with society. Based on that concept, Graham et al. (25) developed the Functional Mobility Scale (FMS). This scale differentiates itself from other activity limitation measures by the incorporation of the environment and the possibility of using different assistive devices (26).
A combination of the LIFE-H questionnaire and the FMS gives an in-depth insight into people’s overall functioning. The aim of this study was to evaluate the activity limitations and restrictions in participation for adults with spastic diplegia, who had undergone SDR as children more than 15 years prior to this study. Secondary aims were developed to investigate possible relationships between subjects’ functioning and age (current age and age at SDR), environmental factors (socio-economic-status; SES) and their level of satisfaction, and subjects’ perceptions of the post-operative outcomes. The following aspects were therefore studied: (i) subjects’ functional mobility assessed by the FMS; (ii) quality of social participation based on LIFE-H 3.1. (accomplishment and satisfaction levels); (iii) associations between subjects’ age at SDR, current age and SES with FMS and LIFE-H outcomes; (iv) association between subjects’ LIFE-H accomplishment and satisfaction levels; and (v) the person’s perceptions of the SDR experience from their current perspective.
METHODS
Subjects
At present in South Africa, SDR is performed at only one institution, and each child with CP who fulfils the strict selection criteria for this procedure can be treated at no cost should they not have medical insurance. Subjects for this study were selected from a cohort of people with CP who underwent the same type of SDR procedure at Red Cross Children’s Hospital in Cape Town between 1981 and 1991. They were included if they were diagnosed with spastic diplegia, with or without mild unilateral upper extremity involvement, and excluded if they were diagnosed with dystonia, athetosis, ataxia or hypotonia. In addition, they only received this operation if they had access to ongoing physiotherapy both before and after SDR, together with adequate parental support. Clinical records were used to confirm that the aim of the SDR procedure was functional improvement, either to improve the gait pattern or to develop locomotion if the child was not yet ambulant. For logistical reasons, the subjects had to live in Cape Town or within a radius of 100 km at the time of data collection.
From all the subjects who underwent SDR in the specific time-frame, 47 fulfilled the inclusion criteria from the clinical record audit. We had very limited contact details for these subjects, except for the 7 who had also participated in our completed 20-year follow-up studies (18, 19). A central register of CP does not exist in South Africa, and so an intensive search based on peoples’ names and dates of birth was necessary. With the assistance of family and teachers, use of old medical records and internet contact websites, we were able to locate 37 possible subjects (79%) who were generally representative of the different socio-demographic backgrounds of those subjects who had undergone SDR in South Africa. Telephone contact was established, and we confirmed that 1 person had died (in an accident), and 5 people could not participate as they were unable to attend data-collection sessions for reasons other than health status (e.g. not in town, too busy with work and personal life). Each of the 31 subjects who were eligible and participated in the study completed an informed consent form. This study was approved by the Human Research Ethics Committee at the University of Cape Town.
Outcome measurements
Subject characteristics. A neurosurgeon (JCP) and a physiotherapist (NGL) assessed the subjects and rated their Gross Motor Function Classification System (GMFCS) level (27, 28) and whether they were classified as spastic diplegia with or without mild unilateral upper limb involvement. In addition, the subjects were questioned (based on a semi-structured interview) with regards to socio-demographic and SDR-related topics. The socio-demographic data included: age, gender, current health status, healthcare visits, marital status (children), living situation, SES, highest level of education attained, employment status and main source of income. SES was estimated by housing density, which was calculated as the number of people living in the house divided by the number of rooms (excluding the kitchen and bathroom) in the house (29). SDR-related characteristics included information about subjects’ age at SDR, follow-up time and their experiences with this neurosurgical procedure. With regards to these SDR experiences the following questions were asked: (i) Do you think the SDR operation was worthwhile?; (ii) Looking back, what do you feel is the most important thing you would have done differently (something we clinicians can learn from)?; and (iii) If you had to make the decision to undergo the SDR operation now by yourself (after experiencing the impact of this on your life), would you do it?
Functional Mobility Scale. Together with the subject, one of the two physiotherapists (NGL or SLH) completed the FMS. The FMS is an outcome measure to classify patients’ level of mobility in their daily environment (performance-level), where the possible use of an assistive device is taken into account. The scale is based on a 6-level ordinal grading system, ranging from 1 (use of wheelchair) to 6 (independent on all surfaces). Subjects are rated for 3 different distances; 5, 50 and 500 m (25). The FMS has been used in different studies (30, 31) and proven to be valid and reliable in children with CP (25, 32). The validity and reliability of FMS has not been tested in adults. However, its use seems to be feasible for all age groups and is currently used for studies with adults (personal communication, Adrienne Harvey).
Life-Habit questionnaire. One of the two physiotherapists (NGL or SLH) completed the LIFE-H 3.1 with each subject. Both strictly followed the published guidelines and completed the answers themselves, while consulting the subject thoroughly.
The LIFE-H is based on 77 life habits, which are related to Daily Activities (DA) and Social Roles (SR) items. DA comprises 6 categories (Nutrition, Fitness, Personal Care, Communication and Housing), while SR is subdivided into another 6 categories (Responsibilities, Interpersonal Relationships, Community Life, Education, Employment and Recreation). Each of these 12 categories incorporates 4–8 different life habits. For each of the categories of the DA and SR items a weighted Accomplishment (Acc) and Satisfaction (Sat) score is calculated. The weighted Acc-score is a result of the subject’s level of difficulty and need for assistance to accomplish the life habit (Appendix 1), while the Sat-score is based on the subject’s level of satisfaction to achieve the life habit in the specific manner as described for the Acc-score (Appendix 2).
The LIFE-H questionnaire’s measurement of accomplishment levels has been tested for validity and reliability in people of all ages (from children to older adults) and different diagnostic groups. The questionnaire has been used in different study cohorts of children (33–35) and adults (36, 37) with CP. The LIFE-H 3.1 showed acceptable content and convergent validity with similar constructs of other questionnaires (35), and demonstrated moderate to excellent test-retest and intra- and inter-rater reliability (24, 35). With regard to the satisfaction scale of the LIFE-H 3.1, Poulin & Desrosiers (38) reported high test-retest intra-class correlation coefficients. In addition, they emphasized that both the accomplishment level and the satisfaction level should be used for a correct interpretation of an individual’s actual level of participation.
Statistical analysis. Descriptive statistical analyses were used to summarize subjects’ characteristics. For the subjects’ level of activity and participation, mean values and standard deviations of the FMS and LIFE-H questionnaire outcomes were calculated. To investigate the outcomes of the LIFE-H more specifically, we categorized the results of the accomplishment component, based on the mean weighted score into 3 levels: (i) score ≥ 8.0: independent with no difficulties (with or without assistance); (ii) score 5–8: independent with difficulties (with or without assistance); and (iii) score ≤ 5.0: dependent, since the life habit is not carried out by the subject or accomplished with human assistance. The outcomes of the satisfaction level were categorized into 2 levels: (i) score < 0.0: dissatisfied; and (ii) score ≥ 0.0: satisfied.
Relationships between subjects’ characteristics and the outcome variables were examined. Spearman’s rank correlation analyses were performed to determine the bivariate correlation between age at SDR, current age, and SES with 5, 50 and 500 m FMS, as the data were non-parametric. Pearson’s correlation tests were used to examine the correlation of these 3 variables with mean LIFE-H Accomplishment outcomes (Acc-DA and Acc-SR) and for the Satisfaction (Sat-DA and Sat-SR) correlations. The mean Acc-DA and Sat-DA was calculated by taking the average of the scores on the 6 constituent items on the subscale, and the mean Acc-SR and Sat-SR was calculated on the average of the scores on the 5 constituent items of the subscale. A Bonferroni corrected alpha-level of p ≤ 0.008 was used as a threshold for statistical significance. Pearson’s correlations were performed to demonstrate any correlations between Accomplishment and Satisfaction LIFE-H scores for the mean DA- and SR-scores and the mean of the total scores.
RESULTS
Personal and selective dorsal rhizotomy-related characteristics
Table I presents detailed characteristics of the 31 adults with spastic diplegia, who participated in the current study. They were 21 years or older and had undergone SDR more than 15 years ago, and at the time of surgery 71% were between 2 and 7 years old. They were all ambulant, classified at GMFCS levels I–III and only 5 (16%) subjects had spastic diplegia with mild unilateral upper limb involvement. The majority of the study cohort had no other health issues. However, 1 subject was diagnosed with Crohn’s disease and another one with Graves’ disease, 5 (16%) subjects had squint, 2 females (6%) had regular bladder infections and 1 subject took medication for high blood pressure. As a result of these problems (which were unrelated to SDR), 5 subjects (16%) visited a specialist and 3 (10%) a general practitioner, while 2 subjects (6%) had received treatment from a physiotherapist to relieve back pain during the previous month.
|
Table I. Subject characteristics
|
|
Variable
|
Subjects
|
|
Current age, years, median (range)
|
26.8 (21–44)
|
|
Age at SDR, years, median (range)
|
5.2 (2–27)
|
|
Follow-up time after SDR years, median (range)
|
21.3 (17–26)
|
|
SESa, median (range)
|
1.0 (0.3–4.0)
|
|
GMFCS, n (%)
|
|
|
Level I
|
15 (48)
|
|
|
Level II
|
11 (36)
|
|
|
Level III
|
5 (16)
|
|
Gender, n (%)
|
|
|
|
Male
|
18 (58)
|
|
|
Female
|
13 (42)
|
|
Marital status, n (%)
|
|
|
Single
|
17 (55)
|
|
|
Relationship
|
8 (26)
|
|
|
Married
|
6 (19)
|
|
Living situation, n (%)
|
|
|
Alone
|
2 (6)
|
|
|
With (grand)parents
|
21 (68)
|
|
|
With partner (or others)
|
8 (26)
|
|
Highest obtained degree in education, n (%)
|
|
|
Primary school (grade 1–7)
|
1 (3)
|
|
|
Secondary school (grade 8–12)
|
13 (42)
|
|
|
Higher education
|
|
|
|
Courses
|
6 (19)
|
|
|
College
|
7 (23)
|
|
|
University
|
4 (13)
|
|
Employment/student, n (%)
|
|
|
Full-time job (> 36 h/week)
|
19 (61)
|
|
|
Part-time job
|
2 (7)
|
|
|
Unemployed
|
6 (19)
|
|
|
House-keeping
|
1 (3)
|
|
|
Looking for job
|
2 (7)
|
|
|
Student
|
1 (3)
|
|
Main income, n (%)
|
|
|
Paid job
|
22 (71)
|
|
|
Disability pension
|
7 (23)
|
|
|
Family income
|
2 (6)
|
|
aBased on housing density (number of people: number of rooms in the house) (26).
SDR: selective dorsal rhizotomy; GMFCS: Gross Motor Function Classification System; SES: socio-economic status.
|
Fourteen subjects (45%) had a partner and 6 (19%) had (non-disabled) children. None of the study cohort stayed in an institution, but lived alone, with parents, partner or other housemates. Two subjects (6%) had special adaptations in their houses. Eight subjects (26%) had a low SES based on their housing density ratio > 1.5 (e.g. 5 people in a house with 3 rooms), while 12 subjects (39%) had a housing density ratio of between 1.0 and 1.5 (e.g. 4 people/3 rooms), and 11 subjects (35%) had a ratio < 1.0 (e.g. 2 people/3 rooms). More than half of the study cohort had some form of higher education, such as a diploma or degree for attending a course (19%), college (23%) or university (13%), while 1 subject was still studying. He and another 21 subjects (71%) had a job, and their loan resulted in the main income, while 7 (23%) received a disability pension and 2 (6%) relied on the income of their partner or parents.
In response to the questions about the SDR operation, 23 subjects (74%) agreed that it had been worthwhile, while 7 (23%) answered that they “didn’t know”, and 1 had no positive feelings about this. Ten subjects (32%) realized that they should have done more exercise or sport and 6 (19%) regretted that they did not or could not carry on with physiotherapy after school; 4 (13%) had no idea if they should have done something different, while 11 (35%) were happy with what they had done in the last years. Twenty-five of the study cohort (81%) responded that they would have decided to undergo the operation now they could make independent decisions, 4 of them (13%) were not sure, while 2 (6%) would not have undergone the operation.
Functional Mobility Scale
For the distance of 5 m the subjects were rated as follows: 9 subjects (29%) at level 6: independent on all surfaces; 17 (55%) at level 5: independent on level surfaces; 1 (3%) at level 4: use of stick(s); and 4 (13%) at level 3: use of crutch(es). The outcomes of FMS at 50 and 500 m were similar in this study: 7 subjects (22%) were rated at level 6, 12 (39%) at level 5, and 12 at level 3.
Life-Habit questionnaire
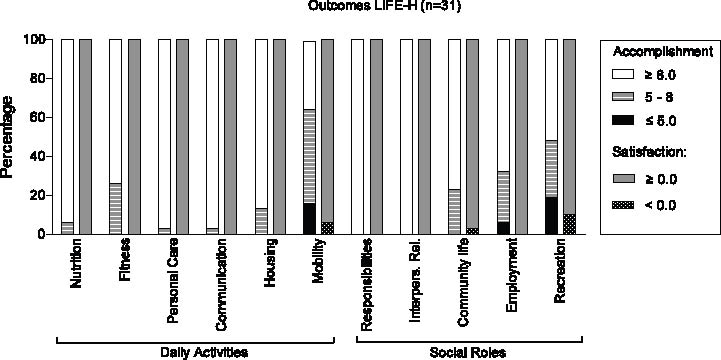
Table II shows the weighted mean scores with standard deviations and medians of the different categories of the LIFE-H questionnaire in regards to subjects’ Accomplishment and Satisfaction levels. In addition, Fig. 1 presents the percentages of subjects who were classified as independent with/without difficulties or dependent (accomplishment level) and satisfied or dissatisfied (satisfaction level) for the various daily activities and social role LIFE-H items.
|
Table II. Outcomes of the Life-Habit (LIFE-H) questionnaire
|
|
LIFE-H items
|
n
|
Accomplishment
|
Satisfaction
|
|
Mean
|
Median
|
SD
|
Mean
|
Median
|
SD
|
|
Daily activities
|
|
|
|
|
|
|
|
|
|
Nutrition
|
31
|
9.7
|
10.0
|
0.9
|
8.5
|
10.0
|
2.7
|
|
|
Fitness
|
31
|
9.0
|
9.7
|
1.3
|
7.4
|
7.5
|
2.6
|
|
|
Personal care
|
31
|
9.7
|
10.0
|
0.5
|
8.5
|
10.0
|
2.1
|
|
|
Communication
|
31
|
9.8
|
10.0
|
0.5
|
9.0
|
10.0
|
2.0
|
|
|
Housing
|
31
|
9.3
|
9.6
|
1.0
|
8.0
|
10.0
|
2.7
|
|
|
Mobility
|
31
|
7.1
|
6.7
|
2.0
|
5.3
|
6.3
|
4.1
|
|
|
Total daily activities
|
31
|
9.1
|
9.2
|
0.7
|
7.8
|
8.8
|
2.3
|
|
Social roles
|
|
|
|
|
|
|
|
|
|
Responsibilities
|
31
|
9.9
|
10.0
|
0.3
|
9.1
|
10.0
|
1.8
|
|
|
Interpersonal relationships
|
31
|
9.8
|
10.0
|
0.5
|
8.7
|
10.0
|
2.5
|
|
|
Community life
|
31
|
8.9
|
9.4
|
1.5
|
6.8
|
8.6
|
3.9
|
|
|
Educationa
|
13
|
9.1
|
10.0
|
0.8
|
5.8
|
10.0
|
7.3
|
|
|
Employment
|
31
|
8.4
|
8.9
|
2.2
|
63
|
5.0
|
3.4
|
|
|
Recreation
|
30
|
7.4
|
8.6
|
2.8
|
5.6
|
6.4
|
4.7
|
|
|
Total social roles
|
31
|
8.9
|
9.2
|
1.1
|
7.3
|
7.9
|
2.6
|
|
Total
|
31
|
9.0
|
9.1
|
0.8
|
7.6
|
8.7
|
2.3
|
|
aNot included for calculation of Total social roles and Total scores.
SD: standard deviation.
|
Fig. 1. Outcomes of Life-Habit (LIFE-H) questionnaire categorized. Accomplishment levels weighted score ≥ 8.0: independent and no difficulties; score 5–8: independent with difficulties; and score ≤ 5.0: dependent or not able to accomplish. Satisfaction levels with score ≥ 0.0: satisfied; and score < 0.0: dissatisfied.
With regard to daily activities, on average 81% of the subjects reported being independent and had no difficulties in accomplishing certain life habits. The subjects reported few problems with the items of Nutrition, Personal Care and Communication. Subjects faced the largest restrictions with the Mobility item. Sixteen percent of the subjects were dependent on human assistance or were not able to accomplish the different mobility tasks at all, 48% were independent but had difficulties and 36% had no difficulties with this. In line with this, 6% of the study cohort reported they were dissatisfied with Mobility, while all subjects were (very) satisfied with how they accomplished the other daily activities. However, the variability of Mobility weighted scores was relatively large.
We excluded Education from the analyses of the 6 social roles, as this item was not applicable for the majority of the subjects. For the remaining 5 items, on average 79% of the subjects had no problems to accomplish these 5 SR items indepdently. The highest accomplishment levels were scored for Responsibility and Interpersonal Relationships, for which none of them had any difficulties. This was in contrast to Employment and Recreation where relatively lower weighted scores were reported, with 6% and 19%, respectively, who did not accomplish this or only with human assistance, and also showed a greater variability compared with the other social role items. With regard to subjects’ satisfaction levels, all subjects were satisfied with Responsibilities and Interpersonal Relationships, while 10% were not satisfied with their level of Recreation and 3% with Community Life. Despite the fact that some subjects had difficulties with Employment, none of them reported being dissatisfied in this domain.
Associations
The estimated rank correlation coefficients as well as the p-values (two-tailed) regarding the relation between subjects’ characteristic variables (age at SDR, current age and SES), and the FMS outcomes, and with the Life-H data (estimated correlation coefficients, not ranked) are shown in Tables III and IV, respectively. There was no significant correlation between any of the characteristics and any of the FMS or Life-H outcomes.
|
Table III. Spearman’s rank correlations between Functional Mobility Scale (FMS) and subjects’ characteristic variables (n = 31)
|
|
Variables
|
5 FMS
|
50 FMS
|
500 FMS
|
|
r
|
p
|
r
|
p
|
r
|
p
|
|
Age at SDR
|
0.23
|
0.22
|
0.27
|
0.14
|
0.27
|
0.14
|
|
Current age
|
0.26
|
0.17
|
0.14
|
0.46
|
0.14
|
0.46
|
|
SES
|
0.18
|
0.35
|
0.24
|
0.19
|
0.24
|
0.19
|
|
p-values are 2-tailed; significant at p ≤ 0.008.
5FMS: FMS on 5m; 50FMS: FMS on 50m; and 500FMS: FMS on 500m; SDR: selective dorsal rhizotomy; SES: socio-economic status.
|
|
Table IV. Pearson’s correlations between Life-Habit questionnaire and subjects’ characteristic variables (n = 31)
|
|
Variables
|
Acc-DA
|
Acc-SR
|
Sat-DA
|
Sat-SR
|
|
r
|
p
|
r
|
p
|
r
|
p
|
r
|
p
|
|
Age at SDR
|
0.02
|
0.91
|
–0.16
|
0.40
|
–0.16
|
0.38
|
0.09
|
0.59
|
|
Current age
|
0.16
|
0.38
|
–0.10
|
0.58
|
–0.06
|
0.74
|
0.24
|
0.19
|
|
SES
|
0.29
|
0.11
|
0.11
|
0.56
|
–0.29
|
0.64
|
0.08
|
0.67
|
|
p-values are 2-tailed; significant at p ≤ 0.008.
Acc-DA: Accomplishment score for Daily Activities; Acc-SR: Accomplishment score for Social Roles; Sat-DA: Satisfaction score for Daily Activities; Sat-SR: Satisfaction score for Social Roles; SDR: selective dorsal rhizotomy; SES: socio-economic status.
|
A Pearson’s correlation analysis demonstrated a strong positive correlation between the total Accomplishment LIFE-H score and the total Satisfaction LIFE-H score, r = 0.78, p < 0.01 (two-tailed), which is based on daily activities and social roles outcomes. Therefore, strong positive correlations were demonstrated between Acc-DA and Sat-DA and Acc-SR and Sat-SR (r = 0.79, p < 0.01 and r = 0.73, p < 0.01, respectively).
DISCUSSION
In line with our previous long-term follow-up studies regarding adult impairments and functioning (capacity level) (18–20), this study also demonstrated high levels of functioning, but this time specifically in subjects’ functional performance level and participation in the community more than 15 years after SDR.
Functional Mobility Scale
The FMS was used as an outcome measure of subjects’ mobility levels in a daily indoors and outdoors setting. More than 15 years after SDR 84% of the study cohort was able to walk independently for 5 m, and 61% for 50 and 500 m, while the remainder had to use sticks or crutches. This is in line with the outcomes of our previous 20 year follow-up study (21), in which we reported that, in general, 79% of adults with spastic diplegia walked without assistive devices and 14% with crutches or cane. However, this is different from the studies of Andersson & Mattsson. (39) and Ando & Ueda (17), wherein patients who did not receive SDR were assessed and reported 49% and 57% of study cohorts respectively walked independently, while 30% and 43% walked with assistive devices. Nonetheless, it has to be taken into account that the mean age at which functional deterioration has been reported is approximately 37 years (13, 17), and that the age of our study cohort ranged from 21–44 with a median age of 27 years, while the mean age in the other two studies was mid-30s and the oldest participants were in their 50s.
In general, it is expected that subjects with a disability will be rated differently for the 3 distances. However, we found for each of the 31 subjects no difference in mobility between 50 and 500 m. No subjects rated a 1 or 2 for these distances, which means that nobody used a walker, frame or wheelchair. The FMS is a measure of subjects’ performance and is therefore influenced by personal and environmental factors. This issue might be an explanation for our conflicting outcomes, it may be that some subjects would have used one of these assistive devices, but could not access one for financial reasons. Unfortunately, we did not study this question and cannot give any answers, but we emphasize that this interesting issue should be taken into account for future research projects.
Life-Habit questionnaire
Accomplishment with daily activities. Based on the LIFE-H 3.1. we found that the majority of our study cohort were independent and had no difficulties in accomplishing any of the specific daily activities (Acc-DA). This outcome is similar for adults with CP who did not receive SDR, as reported in studies also based on the LIFE-H, Functional Independent Measure/Functional Assessment Measure (FIM/FAM) or Barthel Index (36, 40, 41).
More specifically, in our study cohort the greatest difficulties (highest level of dependency) were seen in the Mobility category. Donkervoort et al. (36) also reported for their 103 adolescents and young adults with CP who did not receive SDR, the lowest LIFE-H mean Acc-DA scores for the Mobility category. This score was not especially different to our outcome, while the percentage of subjects with Mobility difficulties was much higher. This latter fact can be explained by a much greater variability (standard deviation) in our study cohort, which might be due to an older and wider age range.
Accomplishment with social roles. In regards to the accomplishment of LIFE-H social roles we found that the majority (79%) was independent and had no difficulties in performing the different roles, which was just higher than the 76% of the subjects who did not receive SDR as reported by Donkervoort et al. (36). We found most problems in the categories Employment and Recreation, while Donkervoort et al. (36) showed fewer problems accomplishing the Recreation tasks. Problems with employment for people with disabilities are world-wide phenomena, while there might be differences in facilities related to recreational activities. South Africa is a developing country and the facilities might be not as well organized as in the Netherlands.
Satisfaction with life habits. Unfortunately the level of satisfaction to accomplish different tasks has not been reported often in the literature. We found that the subjects of our study cohort reported being (very) satisfied, with some exceptions for the Mobility (Sat-DA) and Recreation (Sat-SR) category.
Associations
It has been shown that with increased age adults with spastic diplegia presented deteriorated walking ability (12, 13). However, based on the FMS and LIFE-H outcomes, we found no significant correlation between age and overall functioning.
In addition, no associations were found for FMS and LIFE-H with SES either. However, we agree with Ando & Ueda (17) that functional status may be determined by factors intrinsic to CP. We also believe that other environmental factors play an important role in the development of patients’ functional level and should be included in any evaluation and clinical interpretation of patient status.
Strong statistically significant correlations were found for the total LIFE-H Accomplishment and Satisfaction levels (r = 0.80), and also for the subscales of total DA (r = 0.82) and SR (r = 0.66) scores. This is in contrast to the recently published study of Poulin & Desrosiers (38), where correlations of 0.43 for the averages of all categories were reported, and 0.36 for DA and 0.24 for SR. They used the LIFE-H questionnaire in a population of older adults with functional disabilities, aged ≥ 65 years, which might be the reason for this difference.
Selective dorsal rhizotomy experience
In line with the high level of satisfaction as reported for the LIFE-H questionnaire life habits by our subjects more than 15 years after SDR, the majority of this study cohort reported that they found the SDR operation worthwhile and would have elected to receive the operation if they had to decide themselves. However, more than half of the cohort reported a lack of physical activity and physiotherapy after they left school. The lack of care with transition into adulthood has also been described in other studies, and different research groups have emphasized the demand for better long-term follow-up with guidance, training programmes and healthcare after leaving school (12, 39, 42).
Limiting factors
One of the aspects that has to be noted is that our sample size of 31 subjects was relatively small, meaning that our outcomes should be seen as an important indication of long-term outcomes, but not as definitive. We believe we achieved a high participation rate given the long time between surgery and this follow-up assessment. From inspecting the original hospital data we are also confident that the people we were able to locate and who gave their consent were representative of the group; that is to say, those involved do not represent a skewed sample.
In addition, as part of this study we did not have a CP control group, but rather compared our outcomes with information published by other Western research groups. We should emphasize that this study was conducted in South Africa, and the health environment is not as well developed as in Western countries. We also do not know if cultural differences have an influence on peoples’ level of coping, which in turn might be related to patients’ functioning and satisfaction in life. However, we believe it is important that long-term outcome data, across meaningful domains, is reported broadly.
In conclusion, with this first published long-term follow-up study we can suggest that adult with spastic diplegia (with or without mild involvement of unilateral upper limb) and who have undergone SDR as children have a high level of functioning within the Activity and Participation components of the ICF model. This outcome has important implications for clinicians, patients and parents when they consider the most effective treatment option.
In addition, subjects’ accomplishment levels are strongly correlated with their levels of satisfaction, which is in line with their positive feelings about the SDR operation. However, it has to be noted that there is a great demand for better and more care as people with CP make the transition from adolescence to adulthood.
ACKNOWLEDGEMENTS
This study was funded by the Medical Research Council of South Africa.
REFERENCES
|
APPENDIX 1. Calculation weighted Accomplishment score (Acc-score)
|
|
Acc-score
|
Difficulty level
|
Assistance Type
|
|
9
|
No Difficulty
|
No assistance
|
|
8
|
No Difficulty
|
Assistive device or adaptation
|
|
7
|
With Difficulty
|
No assistance
|
|
6
|
With Difficulty
|
Assistive device or adaptation
|
|
5
|
No Difficulty
|
Human assistance
|
|
4
|
No Difficulty
|
Assistive device or adaptation and human assistance
|
|
3
|
With Difficulty
|
Human assistance
|
|
2
|
With Difficulty
|
Assistive device or adaptation and human assistance
|
|
1
|
Accomplished by a proxy
|
–
|
|
0
|
Not accomplished
|
–
|
|
N/A
|
Not applicable
|
–
|
|
Formula weighted Acc-score:
|
(∑Acc-scores x10):(number of applicable life habits x9)
|
|
Range weighted Acc-score:
|
0 to 10
|
|
APPENDIX 2. Calculation weighted Satisfaction score (Sat-score)
|
|
Sat-score
|
Satisfaction level
|
|
10
|
Very satisfied
|
|
5
|
Satisfied
|
|
0
|
More or less satisfied
|
|
–5
|
Unsatisfied
|
|
–10
|
Very unsatisfied
|
|
Formula weighted Sat-score:
|
(∑Sat-scores):(number of applicable life-habits)
|
|
Range weighted Sat-score:
|
–10 to 10
|